

Abstract
Background
Physical inactivity is an important modifiable risk factor for non-communicable disease. The degree to which physical activity affects the life expectancy of Americans is unknown. This study estimated the potential years of life gained due to leisure-time physical activity across the adult lifespan in the United States.
Methods
Data from the National Health and Nutrition Examination Survey (2007–2010), National Health Interview Study mortality linkage (1990–2006), and US Life Tables (2006) were used to estimate and compare life expectancy at each age of adult life for inactive (no moderate-to-vigorous physical activity), somewhat active (some moderate-to-vigorous activity but <500 metabolic equivalent min/week) and active (≥500 metabolic equivalent min/week of moderate-to-vigorous activity) adults. Analyses were conducted in 2012.
Results
Somewhat active and active non-Hispanic white men had a life expectancy at age 20 that was around 2.4 years longer than the inactive men; this life expectancy advantage was 1.2 years at age 80. Similar observations were made in non-Hispanic white women, with a higher life expectancy within the active category of 3.0 years at age 20 and 1.6 years at age 80. In non-Hispanic black women, as many as 5.5 potential years of life were gained due to physical activity. Significant increases in longevity were also observed within somewhat active and active non-Hispanic black men; however, among Hispanics the years of life gained estimates were more variable and not significantly different from 0 years gained.
Conclusions
Leisure-time physical activity is associated with increases in longevity in the United States.
INTRODUCTION
Concern about the deleterious health effects of a physically inactive lifestyle is at an unprecedented level. Less than half of the adult population meet physically active guidelines of 150 minutes per week of moderate-to-vigorous physical activity (MVPA).1,2 This is troubling as physical activity protects against the development of several chronic diseases and premature mortality.3,4
The benefits of physical activity are usually expressed by comparing the relative risks of disease and mortality in physically active and inactive groups.3,4 While informative to researchers and practitioners, the general public may not understand or be captivated by these statistical estimates. Another way to express the benefits is to compare the life expectancy of physically active and inactive persons. Health messages that focus on life expectancy are easy to understand, and they may motivate inactive persons to adopt an active lifestyle.5
Research on increases in life expectancy due to physical activity is sparse.6–10 The five studies addressing this question suggest that physical activity increases life expectancy by 1.3 to 5.5 years. While informative, these studies have important limitations. None were based on representative datasets, four of five were based on older cohorts,6,7,9,10 only one considered whether the effects vary by age,6 and none considered racial/ethnic variations. As the effects of physical activity may vary according to these demographic characteristics, and because it is important to have tailored health messages,11 age, sex, and race/ethnic specific data are needed. Therefore, the objective of this study was to estimate the years of life gained due to leisure-time physical activity for the adult American population. Estimates were provided across the adult lifespan, for both sexes, and in different racial/ethnic groups.
METHODS
Overview of Calculation Method
The years of life gained due to leisure-time physical activity were estimated using the following information: (1) The proportion of varying levels of leisure-time physical activity in each year of adult life obtained from the 2007–2010 National Health and Nutrition Examination Survey (NHANES); (2) The hazard ratio (HR) for death associated with varying levels of leisure-time physical activity obtained from the 1990, 1991, and 1995 National Health Interview Survey (NIHS), with mortality follow-up to 2006; (3) The probability of death during each year of life obtained from the 2006 US life tables. All analyses were conducted in 2012.
Proportion of Physical Activity Categories
The proportion of the population within three physical activity categories were obtained from the 2007–2010 NHANES, a representative sample of the noninstitutionalized US population.12 Hispanics, non-Hispanic blacks, and older adults were oversampled, and sample weights were used to produce unbiased estimates. Herein, only non-Hispanic white, non-Hispanic black, and Hispanics were examined; the sample sizes of other racial/ethnic groups were insufficient.
The NHANES physical activity questionnaire asked participants to report the number of days in a typical week and the average duration per day they partook in the following activities for ≥ 10 consecutive minutes: (1) walking or bicycling for transportation; (2) moderate intensity sports, fitness or recreational activities (activities that result in moderate increases in heart rate and breathing); and (3) vigorous intensity sports, fitness or recreational activities (activities that result in large increases in heart rate and breathing). Assuming a metabolic equivalent (MET) of 4.0 for walking/bicycling, 4.0 for moderate intensity, and 8.0 for vigorous intensity activities,3,13 these data were used to estimate the MET min/week of MVPA that fell outside of routine activities of daily living and work. Participants were placed into inactive (0 MET min/week), somewhat active (some activity but <500 MET min/week), active (≥500 MET min/week) leisure-time physical activity categories.14 Five hundred MET min/week of MVPA is equivalent to the public health guidelines for physical activity (e.g., 150 minutes of moderate activity or 75 minutes of vigorous activity or an equivalent combination of the two intensities).3,14
For each sex and racial/ethnic group, and specific to each age, we estimated the proportion of individuals who were physically inactive, somewhat active, and physically active. Because of the small number of participants within each one year age group, within each sex and race/ethnicity specific group we estimated the probability of being in each physical activity category using separate logistic regression models run on cubic polynomial age terms (age, age2, age3).15 Thus, the proportion of participants within each activity category across age was calculated using a smoothing procedure based on moving averages. All logistic models were fit using SAS version 9.2 (SAS Inc., Carry, NC).
Hazard Ratio for Death within Physical Activity Categories
To estimate the HR for death we used data from the 1990, 1991, and 1995 NHIS and its linked mortality files. The NHIS is an annual nationally representative cross-sectional survey.16 The 1990, 1991, 1995 cycles were the only pre-2000 cycles that included a questionnaire that could assess adherence to physical activity guidelines. The NHIS mortality files combine the survey data with mortality data from the National Death Index through Dec 31, 2006. The final analysis sample consisted of 95,358 adults (aged ≥ 18 years), of whom 18,568 died, with a total of 912,781 person years of follow-up. Analyses took into account the sample weights and complex survey design.
The NHIS physical activity questionnaire asked participants the frequency they partook in 20 common leisure-time physical activities (and 2 other activities not on that list) over the past 2 weeks, the average duration of activity on each occasion, and the intensity of these activities (moderate – moderate increase in heart rate and breathing; vigorous – large increase in heart rate and breathing). As explained above for NHANES, the average MET min/week of MVPA was calculated for each participant, and they were placed into the same inactive, somewhat active, and active categories.
Age, smoking (never, former, current), annual household income (<$10,000; $10,000–$19,999; $20,000–$34,999; $35,000–$49,999; ≥$50,000; did not report), and occupational activity were included as confounders in the HR estimates. An a priori decision was made to force all of these confounders into the regression models as they are known correlates of leisure-time physical activity and mortality. For occupational activity, if employed, participants were assigned a MET for their occupation type.17 If their major activity was keeping house, participants were assigned an occupational MET of 2.43, the average of 9 housework and food preparation activities.18 If their major activity was going to school, participants were assigned an occupational MET of 1.91, the average of 13 taking classes and homework activities.18 Unemployed and retired participants were assigned an occupation MET of 1.61, the average of 21 socializing and relaxing activities.18
The HRs were generated using Cox proportional hazard models in SAS version 9.2 (SAS Inc., Carry, NC). Variables in the models were physical activity, age, age2, smoking, income, and occupational MET. Interaction terms between age and physical activity were considered, but because these were not significant, they were not retained. The Schoenfeld residuals indicated that there were no violations of the proportional hazards assumption.
Probability of Death at Each Age
The 2006 US life tables were used to derive information on the probability of death during each year of life starting at age 18.19 For each one year age interval within each sex and racial/ethnic group, we obtained an estimate of the probability of death conditional on having lived to the start of that interval.
Estimate of Years of Life Gained Due to Leisure-Time Physical Activity
The approach and calculations used to estimate the years of life gained due to leisure-time physical activity is based upon the methods developed by Fontaine and colleagues20 and refined by Finkelstein and colleagues.21 More details on this approach and the specific formulas used for the calculations are provided in their papers.20,21 Briefly, we performed the following calculations within each sex and racial/ethnic group. First, the probability of death in each 1 year age group from the US life tables,19 which is unconditional on leisure-time physical activity, was multiplied by an age- and physical activity category-specific adjustment factor. This adjustment factor equalled the HR for the physical activity category of interest, divided by the sum of the product of the proportion of people in each physical activity category and their respective HR for mortality. Second, using the adjusted probability of death estimates, the median life expectancy within each physical activity category at each age was estimated. Third, at each age we calculated the years of life gained due to leisure-time physical activity as the difference between the life expectancy of a person in the inactive category and similar persons in the somewhat active and active categories.
Estimate of Hours of Life Gained per Hour of Leisure-Time Physical Activity
The hours of life gained per hour of leisure-time physical activity participated in were also estimated. These estimates were based upon the years of life gained estimates for the active category, the remaining life expectancy at age 20 within the active category, and the amount of leisure time required to achieve the physical activity guideline every week over the remaining life expectancy (150 min/week of moderate or 75 min/week of vigorous activity14). Because life expectancy gains at mid-life and old age reflect both past and future physical activity, the hours of life gained estimates were only calculated for age 20.
RESULTS
Descriptive data are in Table 1. Irrespective of sex and race/ethnicity, there was a noticeable difference in the proportion of NHIS and NHANES participants in the active category. The HR estimates for mortality for the three physical categories are in Table 2. Within non-Hispanic white and non-Hispanics, the somewhat active and active categories had a reduced mortality risk, with HR values in the range of 0.74 to 0.83 for the somewhat active category and 0.58 to 0.82 for the active category. Leisure-time physical activity was not associated with a lower mortality risk in Hispanics.
Table 1.
Summary of surveys providing leisure-time physical activity data
| Population Subgroup | NHIS (1990, 1991, 1995)
|
NHANES (2007–2010)
|
||||||
|---|---|---|---|---|---|---|---|---|
| Unweighted Sample Size | Inactive, % | Somewhat Active, % | Active, % | Unweighted Sample Size | Inactive, % | Somewhat Active, % | Active, % | |
| Non-Hispanic White Men | 31,975 | 55.6 | 16.3 | 28.1 | 2,950 | 38.7 | 14.7 | 46.6 |
| Non-Hispanic Black Men | 4,547 | 61.1 | 13.3 | 25.6 | 1,218 | 38.9 | 13.5 | 47.6 |
| Hispanic Men | 3,449 | 61.5 | 12.8 | 25.7 | 1,749 | 40.2 | 12.7 | 47.1 |
| Non-Hispanic White Women | 42,195 | 60.9 | 17.5 | 21.6 | 2,973 | 43.3 | 17.1 | 39.6 |
| Non-Hispanic Black Women | 8,321 | 68.5 | 14.1 | 17.4 | 1,274 | 52.3 | 19.1 | 28.6 |
| Hispanic Women | 4,871 | 68.2 | 13.7 | 18.1 | 1,941 | 48.8 | 16.3 | 34.9 |
Table 2.
Mortality risks across the leisure-time physical activity categories within the NHIS.
| Population Subgroup | Unweighted Sample Size | Person Years of Follow-Up | Number of Deaths | Physical Activity Category
|
||
|---|---|---|---|---|---|---|
| Inactive | Somewhat Active | Active | ||||
| Non-Hispanic White Men | 31,975 | 434,290 | 6575 | 1.00 | 0.80 (0.74.–0.87) | 0.80 (0.74–0.85) |
| Non-Hispanic Black Men | 4,547 | 59,976 | 1113 | 1.00 | 0.74 (0.59–0.94) | 0.82 (0.67–0.99) |
| Hispanic Men | 3,449 | 47,292 | 385 | 1.00 | 1.13 (0.79–1.61) | 0.88 (0.65–1.21) |
| Non-Hispanic White Women | 42,195 | 578,876 | 8582 | 1.00 | 0.83 (0.77–0.90) | 0.75 (0.70–0.81) |
| Non-Hispanic Black Women | 8,321 | 115,513 | 1483 | 1.00 | 0.76 (0.61–0.94) | 0.58 (0.45–0.75) |
| Hispanic Women | 4,871 | 67,735 | 430 | 1.00 | 1.04 (0.74–1.47) | 1.01 (0.70–1.46) |
Data presented as hazard ratio (95% confidence interval) and were adjusted for age, age2, smoking, income, and occupational activity.
Figure 1 illustrates the potential years of life gained for the active category across the adult lifespan. There were noticeable differences across age, race/ethnicity, and sex. Table 3 presents the years of life gained for the somewhat active and active categories at ages 20, 30, 40, 50, 60, 70, and 80 years. Somewhat active and active non-Hispanic white men had an estimated life expectancy at age 20 that was around 2.4 years longer than the inactive men; this life expectancy advantage decreased to 1.2 years by age 80. Similar observations were made in non-Hispanic white women, with a higher life expectancy within the active category of 3.0 years (95% CI: 2.2, 3.8) at age 20 and 1.6 years (95% CI: 1.2, 1.9) at age 80. The patterns were even more striking in non-Hispanic black women, with as many as 5.5 (95% CI: 3.0, 8.0) years of life gained due to physical activity. Significant increases in longevity were also observed within somewhat active and active non-Hispanic black men; however, among Hispanic men and non-Hispanic women the years of life gained estimates were more variable, and regardless of age, were not significantly different from 0 years gained.
Figure 1.
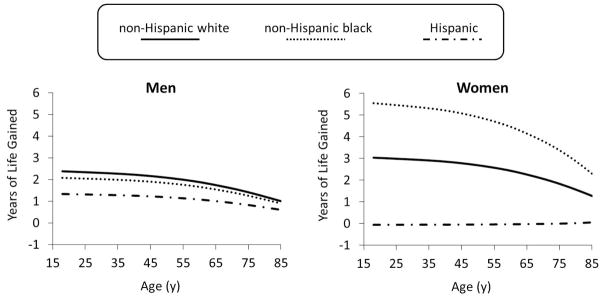
Potential years of life gained in the active category across the adult lifespan
Table 3.
Potential years of life gained in the somewhat active and active categories at different ages
| Age (y) | Non-Hispanic White
|
Non-Hispanic Black
|
Hispanic
|
|||
|---|---|---|---|---|---|---|
| Somewhat Active | Active | Somewhat Active | Active | Somewhat Active | Active | |
| Men | ||||||
| 20 | 2.3 (1.4, 3.2) | 2.4 (1.7, 3.2) | 3.1 (0.6, 5.4) | 2.1 (0.1, 4.2) | −1.3 (−4.8, 2.4) | 1.3 (−0.9, 4.4) |
| 30 | 2.3 (1.4, 3.1) | 2.3 (1.7, 3.1) | 3.0 (0.6, 5.3) | 2.0 (0.1, 4.1) | −1.2 (−4.7, 2.4) | 1.3 (−1.3, 4.3) |
| 40 | 2.2 (1.4, 3.0) | 2.2 (1.6, 3.0) | 2.9 (0.6, 5.1) | 2.0 (0.1, 3.9) | −1.2 (−4.6, 2.3) | 1.3 (−1.5, 4.2) |
| 50 | 2.1 (1.3, 2.8) | 2.1 (1.5, 2.8) | 2.7 (0.6, 4.8) | 1.8 (0.1, 3.7) | −1.1 (−4.3, 2.2) | 1.2 (−1.7, 4.0) |
| 60 | 1.9 (1.2, 2.5) | 1.9 (1.4, 2.5) | 2.5 (0.5, 4.3) | 1.7 (0.1, 3.3) | −1.0 (−3.8, 1.9) | 1.1 (−1.8, 3.6) |
| 70 | 1.6 (1.0, 2.1) | 1.6 (1.2, 2.1) | 2.1 (0.4, 3.7) | 1.4 (0.1, 2.8) | −0.8 (−3.2, 1.6) | 0.9 (−1.8, 3.0) |
| 80 | 1.2 (0.7, 1.6) | 1.2 (0.9, 1.6) | 1.6 (0.3, 2.8) | 1.1 (0.1, 2.1) | −0.6 (−2.4, 1.2) | 0.7 (−1.9, 2.3) |
| Women | ||||||
| 20 | 2.0 (1.1, 2.8) | 3.0 (2.2, 3.8) | 2.9 (0.6, 5.2) | 5.5 (3.0, 8.0) | −0.4 (−3.9, 3.1) | −0.1 (−3.7, 3.7) |
| 30 | 1.9 (1.1, 2.7) | 2.9 (2.2, 3.7) | 2.8 (0.6, 5.0) | 5.4 (2.9, 7.8) | −0.4 (−3.8, 3.0) | −0.1 (−3.6, 3.6) |
| 40 | 1.8 (1.0, 2.6) | 2.9 (2.1, 3.5) | 2.7 (0.6, 4.8) | 5.2 (2.8, 7.5) | −0.4 (−3.6, 2.9) | −0.1 (−3.5, 3.5) |
| 50 | 1.7 (1.0, 2.4) | 2.7 (2.0, 3.3) | 2.5 (0.6, 4.5) | 4.9 (2.6, 7.1) | −0.4 (−3.4, 2.8) | 0.0 (−3.3, 3.3) |
| 60 | 1.6 (0.9, 2.2) | 2.4 (1.8, 3.0) | 2.3 (0.5, 4.1) | 4.5 (2.4, 6.4) | −0.3 (−3.1, 2.5) | 0.0 (−3.0, 3.0) |
| 70 | 1.3 (0.7, 1.9) | 2.1 (1.5, 2.5) | 1.9 (0.4, 3.5) | 3.8 (2.0, 5.5) | −0.3 (−2.6, 2.1) | 0.0 (−2.5, 2.5) |
| 80 | 1.0 (0.6, 1.4) | 1.6 (1.2, 1.9) | 1.5 (0.3, 2.6) | 2.9 (1.6, 4.1) | −0.2 (−2.0, 1.6) | 0.0 (−1.9, 1.9) |
95% confidence intervals presented in parentheses.
The hours of life gained per hour of leisure-time physical activity accumulated during the adult lifespan were estimated for age 20 (Table 4). Twenty year old men were estimated to gain as much as 2.6 hours of life per hour of moderate activity and as much as 5.4 hours of life per hour of vigorous activity. Twenty year old women were estimated to gain as much as 5.6 hours of life per hour of moderate activity and as much as 11.3 hours of life per hour of vigorous activity.
Table 4.
Hours of life gained in the active category per hour of moderate and vigorous activity
| Sex | Non-Hispanic White
|
Non-Hispanic Black
|
Hispanic
|
|||
|---|---|---|---|---|---|---|
| Moderate Physical Activity | Vigorous Physical Activity | Moderate Physical Activity | Vigorous Physical Activity | Moderate Physical Activity | Vigorous Physical Activity | |
| 20 year old male | 2.6 | 5.2 | 2.3 | 5.4 | 1.4 | 2.9 |
| 20 year old female | 3.2 | 6.4 | 5.6 | 11.3 | −0.1 | −0.1 |
Additional analyses were performed to consider whether using more conservative MET values to calculate leisure-time physical activity energy expenditure influenced the results (i.e., 3.0 METs for walking/bicycling and moderate activity, 6.0 METs for vigorous activity). This change had a minimal effect on the relations between leisure-time physical activity and mortality and the years of life gained estimates did not fall outside of the 95% CI shown in Table 3. Additional analyses were performed to consider whether the years of life gained estimates were affected by differences in the proportions of NHIS and NHANES participants in the three activity categories. The maximal effect on this difference on the years of life gained estimates was 0.1 years.
DISCUSSION
Leisure-time physical activity has a meaningful association with life expectancy, at least within the non-Hispanic population, with as much as 5.5 years gained at age 20 for non-Hispanic black women. The time in life gained due to leisure-time physical activity greatly exceeds the time it takes to accumulate this activity over the adult lifespan, particularly if the activity is performed at a vigorous intensity.
The years of life gained estimates for the active category are congruent with the range of 1.3–5.5 years reported in previous studies examining this question.6–10 The present study extends these observations by presenting nationally representative estimates and by presenting variations by sex, age, and race/ethnicity, which were quite meaningful. The present study also examined the hours of life gained, at entry into adulthood, for each future hour of leisure-time physical activity participation. While not addressed in their original study,6 in a response to several letters written about their paper, Paffenbarger and colleagues22 noted that for male Harvard alumni aged 40–70 years, 2.0–2.5 hours of life were gained per hour of future exercise accumulated to age 80. The estimates for 20 year old non-Hispanic white men in the present study – the population group that most closely approximates Harvard alumni – suggest that 2.6 hours are gained per hour of moderate activity and 5.2 hours were gained per hour of vigorous activity accrued in adulthood. A key benefit of vigorous activity in comparison to moderate activity is that an individual only needs to be active for half as long to expand an appropriate amount of energy (e.g., 500 MET min/week). Discrepancies in the life expectancy estimates across studies are likely due to differences in study populations, physical activity questionnaires, and the cut-points used to define the activity groups.
The years of life gained estimates for leisure-time physical activity compare favorably to estimates for obesity and other behavioral risk factors. At age 30 the active non-Hispanic men and women in the present study gained from 2.0–5.4 years. Fontaine and colleagues20 estimated that, at age 30, moderately obese (BMI = 33 kg/m2) whites lose 2 years of life while moderately obese blacks do not lose any years. Other findings suggest that at age 30 vegetarian men and women have a 1.5 year longer life expectancy than non-vegetarians.10 Finally, results from male British doctors suggest that smokers who quit at age 30 increase their life expectancy by 10 years.23
Only one previous study has examined the relationship between physical activity and mortality within Hispanics.24 In that study of Puerto Rican men, mortality risk was reduced with increasing physical activity such that the most active quartile had a 45% reduction in risk. We can only speculate as to why there was no association between leisure-time physical activity and mortality within the Hispanics in our study. It is possible that physical activity does not benefit Hispanics to the same extent as other ethnicities, although this is not supported by studies examining the effect of physical activity on other health outcomes.25–27 Perhaps most of the physical activity of Hispanics is occupational in nature, and therefore not captured by the current study, which focused on leisure-time activity. However, including occupational activity as a covariate only had a slight effect on the relation between leisure-time physical activity and mortality risk, and occupational activity was not an independent predictor of mortality in Hispanics (data not shown). The Hispanic category includes a mixture of ethnic groups, each of which varies considerably. Finally, because the types of leisure-time physical activity assessed in NHIS reflect conventional American behaviors, the activity of Hispanics may have been underreported since it was not assessed in a culturally sensitive manner.28,29
It is hoped that the findings of this study can be used by clinicians and the public health community to help develop effective messages on the importance of physical activity. Simple messages on changes in life expectancy are more easily understood than relative risk estimates and might influence physical activity behaviors.5 Because people are more likely to increase their activity in response to a gain-framed message than a loss-framed message,11 the longevity estimates were presented as the years of life gained due to activity rather than the years of life lost due to inactivity. Finally, because it is important to tailor messages to the individual,11 the sex, age, and race/ethnicity specific estimates should be used when developing messages for individual patients and clients.
This study was not void of limitations. First, the calculations assumed that people’s leisure-time physical activity is constant over time. Second, the leisure-time physical activity measures were self-reported, and such reports are prone to social-desirability and recall biases.30,31 Assuming that these biases are non-differential, the HRs for mortality and the years of life gained estimates in the active groups would have been underestimated. Third, the leisure-time physical activity questionnaires used in NHIS and NHANES changed over time. Therefore, there were comparability issues for the physical activity measures in these two surveys that may have had a subtle impact (≤0.1 years) on the years of life gained estimates. Fourth, the relatively small sample size of non-Hispanic blacks and Hispanics resulted in imprecise estimates within these groups. Finally, dietary intake, obesity, and alcohol were not controlled for as data on these variables were not collected in all NHIS cycles.
In conclusion, leisure-time physical activity has a meaningful association with longevity. Although adhering to a physically active lifestyle over the lifespan is a substantial time investment, this is a sound investment that is likely more than compensated for by the years of life gained.
Acknowledgments
Janssen and Carson had full access to the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Funding for this project was provided by the Heart and Stroke Foundation of Ontario. Janssen was supported by a Canada Research Chair. Carson was supported by a CIHR - Frederick Banting and Charles Best Doctoral Award. Katzmarzyk is supported, in part, by the Louisiana Public Facilities Authority Endowed Chair. Lee is supported, in part, by a grant from the National Institutes of Health (CA154647).
Footnotes
Conflicts of Interest: Janssen has received honoraria, speaker fees, and consulting fees from several non-profit and government organizations that have an interest in physical activity and health. Blair serves on the scientific advisory boards of Technogym, Alere, Jenny Craig, Clarity, and Santech. He also receives honoraria and speaker fees from numerous government and commercial organizations. In the past five years he has received research funding from the National Institutes of Health, Department of Defense, Coca Cola, and Body Media. Lee has served on the scientific advisory board of Virgin HealthMiles. She has received honoraria from several non-profit and government organizations. In the past five years she has received research funding from the National Institutes of Health and Dow Corning.
References
- 1.Office of Surveillance Epidemiology and Laboratory Services of the Centers for Disese Control and Prevention. Behavior Risk Factor Surveillance System. 2009. [Google Scholar]
- 2.Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40:181–8. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- 3.Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008. Washington, DC: U.S. Department of Health and Human Services; 2008. (available at: http://www.health.gov/PAguidelines/Report/) [DOI] [PubMed] [Google Scholar]
- 4.Warburton DE, Charlesworth S, Nettlefold L, Ivey A, Bredin SS. A systematic review of the evidence for Canada’s physical activity guidelines for adults. Int J Behav Nutr Phys Act. 2010;7:39. doi: 10.1186/1479-5868-7-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ziegelmann JP, Lippke S, Schwarzer R. Subjective residual life expectancy in health self-regulation. J Gerontol B Psychol Sci Soc Sci. 2006;61:P195–201. doi: 10.1093/geronb/61.4.p195. [DOI] [PubMed] [Google Scholar]
- 6.Paffenbarger RS, Jr, Hyde RT, Wing AL, Hsieh CC. Physical activity, all-cause mortality, and longevity of college alumni. N Engl J Med. 1986;314:605–13. doi: 10.1056/NEJM198603063141003. [DOI] [PubMed] [Google Scholar]
- 7.Franco OH, de Laet C, Peeters A, Jonker J, Mackenbach J, Nusselder W. Effects of physical activity on life expectancy with cardiovascular disease. Arch Intern Med. 2005;165:2355–60. doi: 10.1001/archinte.165.20.2355. [DOI] [PubMed] [Google Scholar]
- 8.Wen CP, Wai JP, Tsai MK, et al. Minimum amount of physical activity for reduced mortality and extended life expectancy: a prospective cohort study. Lancet. 2011;378:1244–53. doi: 10.1016/S0140-6736(11)60749-6. [DOI] [PubMed] [Google Scholar]
- 9.Karvonen MJ, Klemkola H, Virkajarvi J, Kekkonen A. Longevity of endurance skiers. Med Sci Sports Exerc. 1974;6:49–51. [PubMed] [Google Scholar]
- 10.Fraser GE, Shavlik DJ. Ten years of life: Is it a matter of choice? Arch Intern Med. 2001;161:1645–52. doi: 10.1001/archinte.161.13.1645. [DOI] [PubMed] [Google Scholar]
- 11.Latimer AE, Brawley LR, Bassett RL. A systematic review of three approaches for constructing physical activity messages: What messages work and what improvements are needed? Int J Behav Nutr Phys Act. 2010;7:36. doi: 10.1186/1479-5868-7-36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.National Health and Nutrition Examination Survey Data. [Accessed January 2012];US Department of Health and Human Services, Centers for Disease Control and Prevention, 2012. at [ http://www.cdc.gov/nchs/about/major/nhanes/datalink.htm]
- 13.Pate RR, O’Neil RR, Lobelo F. The evolving definition of “sedentary”. Exer Sport Sci Rev. 2008;36:173–8. doi: 10.1097/JES.0b013e3181877d1a. [DOI] [PubMed] [Google Scholar]
- 14.U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans. Washington, DC: ODPHP; 2008. (available at: www.health.gov/paguidelines) Publication No. U0036;2008. [Google Scholar]
- 15.Heo M, Faith MS, Mott JW, Gorman BS, Redden DT, Allison DB. Hierarchical linear models for the development of growth curves: an example with body mass index in overweight/obese adults. Stat Med. 2003;22:1911–42. doi: 10.1002/sim.1218. [DOI] [PubMed] [Google Scholar]
- 16.National Center for Health Statistics. Information cited in: American Lung Association, Epidemiology and Satistical Unit, Trends in Chronic Bronchitis and Emphysema. 2000. National Health Interview Survey, 1982–1999. [Google Scholar]
- 17.Tudor-Locke C, Ainsworth BE, Washington TL, Troiano R. Assigning metabolic equivalent values to the 2002 census occupational classification system. J Phys Act Health. 2011;8:581–6. doi: 10.1123/jpah.8.4.581. [DOI] [PubMed] [Google Scholar]
- 18.Tudor-Locke C, Washington TL, Ainsworth BE, Troiano RP. Linking the American Time Use Survey (ATUS) and the compendium of physical activities: methods and rationale. J Phy Act Health. 2009;6:347–53. doi: 10.1123/jpah.6.3.347. [DOI] [PubMed] [Google Scholar]
- 19.Arias E. United States life tables by Hispanic origin. Vital Health Stat. 2010;2:1–33. [PubMed] [Google Scholar]
- 20.Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB. Years of life lost due to obesity. JAMA. 2003;289:187–93. doi: 10.1001/jama.289.2.187. [DOI] [PubMed] [Google Scholar]
- 21.Finkelstein EA, Brown DS, Wrage LA, Allaire BT, Hoerger TJ. Individual and aggregate years-of-life-lost associated with overweight and obesity. Obesity (Silver Spring) 2010;18:333–9. doi: 10.1038/oby.2009.253. [DOI] [PubMed] [Google Scholar]
- 22.Paffenbarger RS, Jr, Hyde RT, Wing AL. Letter to editor in response to “Physical activity and longevity of college alumi”. N Engl J Med. 1986;315:400–1. doi: 10.1056/NEJM198603063141003. [DOI] [PubMed] [Google Scholar]
- 23.Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ. 2004;328:1519. doi: 10.1136/bmj.38142.554479.AE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Crespo CJ, Palmieri MR, Perdomo RP, et al. The relationship of physical activity and body weight with all-cause mortality: results from the Puerto Rico Heart Health Program. Ann Epidemiol. 2002;12:543–52. doi: 10.1016/s1047-2797(01)00296-4. [DOI] [PubMed] [Google Scholar]
- 25.Gilliland FD, Li YF, Baumgartner K, Crumley D, Samet JM. Physical activity and breast cancer risk in hispanic and non-hispanic white women. Am J Epidemiol. 2001;154:442–50. doi: 10.1093/aje/154.5.442. [DOI] [PubMed] [Google Scholar]
- 26.Mayer-Davis EJ, D’Agostino R, Jr, Karter AJ, et al. Intensity and amount of physical activity in relation to insulin sensitivity: the Insulin Resistance Atherosclerosis Study. JAMA. 1998;279:669–74. doi: 10.1001/jama.279.9.669. [DOI] [PubMed] [Google Scholar]
- 27.Sacco RL, Gan R, Boden-Albala B, et al. Leisure-time physical activity and ischemic stroke risk: the Northern Manhattan Stroke Study. Stroke. 1998;29:380–7. doi: 10.1161/01.str.29.2.380. [DOI] [PubMed] [Google Scholar]
- 28.Crespo CJ, Smit E, Carter-Pokras O, Andersen R. Acculturation and leisure-time physical inactivity in Mexican American adults: results from NHANES III, 1988–1994. Am J Public Health. 2001;91:1254–7. doi: 10.2105/ajph.91.8.1254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Stewart A, Napoles-Springer A. HRQL assessment in diverse population groups in the US. Medical Care. 2000;38:102–24. [PubMed] [Google Scholar]
- 30.Hayden-Wade HA, Coleman KJ, Sallis JF, Armstrong C. Validation of the telephone and in-person interview versions of the 7-day PAR. Med Sci Sports Exerc. 2003;35:801–9. doi: 10.1249/01.MSS.0000064941.43869.4E. [DOI] [PubMed] [Google Scholar]
- 31.Friedenreich CM, Courneya KS, Neilson HK, et al. Reliability and validity of the Past Year Total Physical Activity Questionnaire. Am J Epidemiol. 2006;163:959–70. doi: 10.1093/aje/kwj112. [DOI] [PubMed] [Google Scholar]