

Abstract
Background:
Although the majority of patients report substantial gains in physical function following primary total knee replacement, the degree of improvement varies widely. To understand the potential role of preoperative pain due to other musculoskeletal conditions on postoperative outcomes, we quantified bilateral knee and hip pain and low back pain before primary total knee replacement and evaluated its association with physical function at six months after total knee replacement.
Methods:
A prospective cohort of 180 patients having primary unilateral total knee replacement reported joint-specific pain in right and left hips and knees (Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC] pain) as well as the low back (Oswestry Disability Index) before surgery. Participants also completed the Short Form-36 (SF-36), including the physical and mental component summary scores, before and at six months after surgery.
Results:
Of the 180 patients, 110 (61%) were women; the mean age was 65.1 years, the mean body mass index (BMI) was 32.5 kg/m2, and mean SF-36 physical component summary score reported before the total knee replacement was 33.1. Before total knee replacement, 56.1% of the patients reported no or mild pain in the nonoperatively treated knee, hips, and low back. In addition, 22.2% of the patients had moderate to severe pain in one location; 12.8%, in two locations; and 8.9%, in three or four locations. Women reported more moderate to severe pain than men did in the nonoperatively treated knee (30% versus 11%; p < 0.004) and ipsilateral hip (26% versus 11%; p < 0.02). At six months, the mean physical component summary score was lower among patients with a greater number of preoperative locations of moderate to severe pain. After adjusting for age, sex, BMI, and SF-36 mental component summary score, moderate to severe preoperative pain in the contralateral knee (p = 0.013), ipsilateral (p = 0.014) and contralateral hip (p = 0.026), and low back (p < 0.001) was significantly associated with poorer function at six months after total knee replacement.
Conclusions:
Preoperative musculoskeletal pain in the low back and nonoperatively treated lower extremity joints is associated with poorer physical function at six months after total knee replacement. The degree of functional improvement varies with the burden of musculoskeletal pain in other weight-bearing locations.
Level of Evidence:
Prognostic Level II. See Instructions for Authors for a complete description of levels of evidence.
Numerous studies have noted that patient-related factors, such as advanced age, female sex, body mass index (BMI) of >35 kg/m2, and poor social support, emotional health, and quadriceps strength, are associated with poorer function after total knee replacement1. However, much of the variability in physical function after primary total knee replacement remains unexplained.
Coexisting medical and musculoskeletal comorbidities have been suggested to explain some of the variable functional outcome, although the data are inconclusive. One study described poorer function in patients with coexisting arthritis and hypertension2. Another study found that, after adjusting for baseline physical function, coexisting medical conditions were not independently significant in predicting function after total knee replacement3. Among studies of musculoskeletal comorbidities, those related to pain in joints other than the operatively treated knee, in particular, have described interesting results. For instance, preoperative pain in the nonoperatively treated knee was associated with poorer knee performance at three years after total knee replacement4. Low back pain was shown to predict poorer physical function after primary total knee replacement5 and was associated with poorer function scores at twelve months and twenty-four months after revision total knee replacement6. These data warrant further investigation and discussion with regard to the importance of musculoskeletal comorbidities in patients undergoing total knee replacement.
The goals of the present prospective research study were to (1) define the prevalence of musculoskeletal pain in the low back, hips, and nonoperatively treated knee in patients undergoing elective unilateral total knee replacement; (2) quantify the degree to which variation in patient-reported postoperative physical function is associated with this preoperative pain; and (3) illustrate the need for a musculoskeletal comorbidity index to summarize the total burden of arthritic and musculoskeletal pain in other joints to evaluate functional improvement after total knee replacement.
Materials and Methods
Data were obtained from a sample of patients having total knee replacement who, following institutional review board approval, were enrolled in a prospective randomized trial. The methods for the trial have been previously published7.
We collected patient-reported function data and a broad array of patient and clinical characteristics within three months before surgery and at six months following surgery from 180 patients undergoing primary, elective unilateral total knee replacement at one high-volume academic total joint replacement center.
Data collected included the following patient characteristics: age, sex, race and ethnicity, and BMI as well as patient-reported preoperative and postoperative emotional health and physical function (Short Form-36 [SF-36] mental component summary [MCS] score and physical component summary [PCS] score, respectively). The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire assessed osteoarthritis symptoms with twenty-two questions measuring pain, stiffness, and function in the operatively treated knee. The WOMAC pain questions were repeated for the nonoperatively treated knee, ipsilateral hip, and contralateral hip to quantify the pain in each lower extremity joint. Musculoskeletal comorbidity was defined as the presence of moderate or severe hip or knee pain (a WOMAC pain score of 4 to 7 or >7, respectively) in the nonoperatively treated joints. The pain items from the Oswestry Disability Index assessed pain in the lumbar spine and a response of moderate or severe was categorized as clinically important lumbar spine pain8. The modified Charlson Comorbidity Index quantified medical comorbidities9.
Analysis
Descriptive statistics for patient characteristics (sex, age, BMI, preoperative MCS score, preoperative PCS score, and medical and musculoskeletal comorbidities) include means, standard deviations, minimums, medians, maximums, and relevant quintiles for continuous variables, frequencies, and rates or proportions for categorical variables. We used descriptive statistics, scatter plots, and box plots to examine the variation in outcomes of interest. Chi-square tests and rank-sum tests were performed to compare differences in musculoskeletal pain and other outcomes among patient subgroups. Mixed models were used to determine associations of six-month PCS scores with preoperative musculoskeletal pain and other predictor variables. In all analyses, a p value of <0.05 was considered significant.
Source of Funding
This study was funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (1RO1AR054479); Joint Action study (P.D.F., principal investigator). The funds supported patient enrollment, data collection, and data analyses.
Results
A total of 180 patients participated in the study; 61% were women, the mean age was 65.1 years, the mean BMI was 32.5 kg/m2, the mean preoperative MCS score was 51.8 points, and the mean preoperative PCS score was 33.1 points. The most common comorbidities were cardiac disease (8.8%), pulmonary disease (6.3%), and renal disease (3.1%). No sex differences were detected with regard to age, BMI, baseline MCS score, or medical comorbidities.
Approximately one-half of the patients (54.4%) reported that moderate or severe pain was present only in the operatively treated knee. Women and men had no difference with regard to rates of moderate to severe pain in the operatively treated knee (76.3% versus 71.0%; p = 0.45). Among all participants before total knee replacement, 56.1% reported no or mild pain in the nonoperatively treated knee, hips, and low back; 22.2% had moderate to severe pain in one location, 12.8% in two locations, and 8.9% in three or four locations. When musculoskeletal pain was tallied by sex, a greater percentage of women than men reported moderate to severe pain in one or more nonoperatively treated joints or the lumbar spine (52.7% versus 30%; p < 0.003) (Fig. 1). Women reported more moderate to severe pain than men did in the nonoperatively treated knee (30% versus 11%; p < 0.004) and ipsilateral hip (26% versus 11%; p < 0.02) (Table I).
Fig. 1.
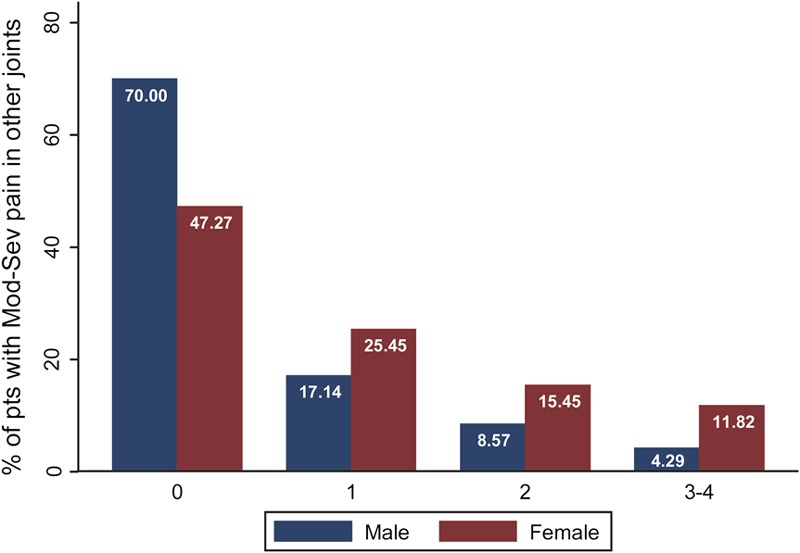
Percentage of male and female patients having total knee replacement by the total number of nonoperatively treated weight-bearing locations (contralateral knee, hips, and low back) with moderate (Mod) to severe (Sev) pain before total knee replacement.
TABLE I.
Moderate to Severe Pain Before Total Knee Replacement in Nonoperatively Treated, Weight-Bearing Locations by Sex
| Location | Total No. (N = 180) | Women (N = 110) | Men (N = 70) | P Value for Sex Difference* |
| Nonoperatively treated knee | 41 (23%) | 33 (30%) | 8 (11%) | <0.004 |
| Ipsilateral hip | 36 (20%) | 28 (25%) | 8 (11%) | 0.02 |
| Contralateral hip | 16 (9%) | 11 (10%) | 5 (7%) | 0.599 |
| Low back | 46 (26%) | 33 (30%) | 13 (19%) | 0.114 |
Fisher exact test.
In unadjusted models, poorer function (SF-36 PCS score) before the total knee replacement was associated with moderate to severe pain in greater numbers of weight-bearing locations (operatively treated knee, nonoperatively treated knee, ipsilateral hip, and low back). Sex, baseline BMI, and medical comorbidities were not significantly correlated with baseline PCS score. After adjusting for patient age, sex, BMI, preoperative MCS score, and medical comorbidities, only greater pain in the surgically treated knee and the low back was significantly associated with poorer function before total knee replacement (adjusted r2 = 0.41).
As shown in Table II, the severity of preoperative pain in nonoperatively treated weight-bearing locations as well as the total number of painful locations were associated with poorer function (SF-36 PCS score) at six months after total knee replacement. Specifically, after adjusting for age, sex, BMI, and preoperative MCS score, poorer physical function at six months was associated with mild, moderate, and severe pain in the nonoperatively treated knee and moderate to severe pain in the ipsilateral and contralateral hips. Importantly, function at six months was inversely and directly correlated with the intensity of pain in the low back. As the severity of back pain increased from mild to moderate to severe, the mean PCS score declined by 3.7, 6.5, and 7.3 points, respectively, with any change of >3 points representing a clinically important difference10.
TABLE II.
Pain Before Total Knee Replacement Predicts Physical Function Score at Six Months Postoperatively After Adjusting for Age, Sex, Body Mass Index, and SF-36 Mental Component Summary Score Before Total Knee Replacement
| Predictor | No. of Patients | Coefficient (95% Confidence Interval) | Significance (p value) |
| Pain intensity in nonoperatively treated knee | |||
| None | 35 | Reference | |
| Mild | 104 | −4.62 (−7.77, −1.48) | 0.004 |
| Moderate to severe | 41 | −4.84 (−8.66, −1.04) | 0.013 |
| Pain intensity in ipsilateral hip | |||
| None | 86 | Reference | |
| Mild | 57 | −0.87 (−3.70, 1.97) | 0.547 |
| Moderate to severe | 37 | −4.15 (−7.44, −0.87) | 0.014 |
| Pain intensity in contralateral hip | |||
| None | 107 | Reference | |
| Mild | 57 | 1.64 (−4.40, 1.11) | 0.241 |
| Moderate to severe | 16 | −5.01 (−9.41, −0.60) | 0.026 |
| Pain intensity in low back (Oswestry) | |||
| None | 91 | Reference | |
| Mild | 43 | −3.68 (−6.60, −0.76) | 0.014 |
| Moderate | 32 | −6.52 (−9.80, −3.24) | <0.001 |
| Severe | 14 | −7.31 (−11.86, −2.76) | 0.002 |
| No. of locations with moderate to severe pain | |||
| 0 | 101 | Reference | |
| 1-2 | 63 | −4.12 (−6.72, −1.52) | 0.002 |
| 3-4 | 16 | −4.95 (−9.43, −0.48) | 0.030 |
Discussion
Our analyses provide evidence that musculoskeletal pain in the lumbar spine, hips, and the nonoperatively treated knee prior to total knee replacement is associated with poorer physical function at six months after total knee replacement. For the 42.5% of the patients with moderate or severe pain in the low back, hips, or contralateral knee, the functional gain after total knee replacement varies with the total burden of musculoskeletal pain.
Several articles have described a correlation between patient attributes, such as age, sex, BMI, emotional status (SF-36 MCS score), and patient-reported physical function after total knee replacement11,12. However, the burden of musculoskeletal pain in weight-bearing joints has not been included in these statistical models. When we added preoperative pain in the lumbar spine, hips, and contralateral knee to multivariate models, and adjusted for demographic characteristics, we found that pain in the nonoperative locations was independently associated with poorer physical function after total knee replacement. Psychometric research has documented that a 3-point difference in the SF-36 PCS score represents a clinically important difference10. In these analyses, the mean PCS score after total knee replacement was >3 points lower for patients with moderate or severe pain in the lumbar spine, contralateral knee, and hips compared with patients with pain limited to the operatively treated knee. Conversely, medical comorbidities were not independently associated with poorer function at six months after total knee replacement, suggesting that musculoskeletal disease plays a greater role than medical comorbidities in explaining variation in physical function in patients after total knee replacement.
Our data also provide new insight into the influence of musculoskeletal pain on the variation in physical function with regard to sex differences and patient attributes.
Many authors have postulated that women wait longer than men do for total knee replacement and therefore have more advanced arthritis in the operatively treated knee and poorer physical function scores at the time of surgery13. However, women in our study did not report more severe pain in the involved knee before surgery than men did. At the time of surgery, a higher percentage of women than men reported moderate or severe pain in the nonoperatively treated knee and in the ipsilateral hip and low back. In addition, more women than men reported pain in a greater number of nonoperatively treated, weight-bearing locations. Our data suggest that the poorer physical function in women before surgery may be associated with a greater burden of nonoperative musculoskeletal pain. The coexistence of systemic joint pain might explain previously reported poorer physical function in women compared with men before, and after, surgery11,12.
Limitations to this study include the relatively small number of patients having primary total knee replacement in some subgroups and the fact that all patients were enrolled at one university setting. While the demographic profile of this sample parallels the U.S. national population, it is important to validate the prevalence of advanced pain in the nonoperatively treated joints in the lower extremity and lumbar spine in a larger, national sample. Despite the limited sample size, clinically important, and significant, differences in the burden of musculoskeletal pain in nonoperatively treated locations were detected as well as a significant association with poorer function at six months after total knee replacement. These preliminary data suggest that surgeons may counsel patients that, while they are likely to experience pain relief in the operatively treated knee after total knee replacement, gains in physical function may be reduced by pain in nonoperatively treated weight-bearing locations. As policy analysts and insurers implement standardized patient-reported measures of physical function to assess outcomes after total knee replacement, they should be aware that postoperative function may vary with overall joint pain burden. Unfortunately, current administrative data sets do not include measures of total joint pain burden in the lumbar spine, hips, and both knees at the time of total knee replacement. This is, in part, due to the lack of a musculoskeletal comorbidity index that would facilitate the measurement of total joint pain burden.
The need for such a system was recognized as early as 1972 by Charnley, who proposed that arthritis in nonoperatively treated joints may influence patient function despite successful joint replacement surgery14 and introduced the Charnley classification system. Charnley recommended classifying patients into one of three categories before hip arthroplasty to summarize the cause of impaired function. These categories were (A) one hip involved, (B) both hips involved, or (C) conditions extending beyond the hips that limit locomotion. This concept can be extrapolated to quantify knee, hip, and low back conditions that limit physical function. While important, the Charnley system is a crude classification that has not been improved since its introduction.
Katz et al. recently proposed a musculoskeletal functional limitations index15. Patients answered the question: “In the past four weeks, how much have problems in any of the following areas limited your activities?” The items assessed problems in the knees, hips, ankles and feet, back, neck, and upper extremities. In contrast to our research, this six-item self-reported musculoskeletal index was tested in a sample of Medicare patients who had undergone primary total knee replacement two years earlier without assessment prior to total knee replacement.
Beyond clinical care, a musculoskeletal burden or severity index may benefit health-care policy makers. Current administrative data do not include measures to summarize the total joint pain burden; this is an important limitation to the interpretation of patient-reported function in the current health-care system. As the United Kingdom and other countries introduce reimbursement for total joint replacement that varies on the basis of patient-reported functional outcomes, greater attention to preexisting pain in other joints is warranted.
In summary, these data suggest that clinicians, policy makers, and researchers may choose to quantify the total burden of musculoskeletal pain in the knees, hips, and low back as they evaluate the likely impact of total knee replacement on postoperative physical function. Data on the total burden of musculoskeletal pain in other joints and the spine are not currently available in billing data or administrative comorbidity codes. However, the Function and Outcomes Research for Comparative Effectiveness in Total Joint Replacement (FORCE-TJR) national U.S. cohort includes measures of pain in the nonoperative locations16. Parallel analyses in this national sample could clarify the potential role for a clinically meaningful measure of musculoskeletal pain burden, a musculoskeletal comorbidity index, to ensure optimal interpretation of research evaluating functional outcome after total knee replacement.
Supplementary Material
Disclosure of Potential Conflicts of Interest
Footnotes
Disclosure: One or more of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support of an aspect of this work. In addition, one or more of the authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to submission of this work, with an entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. No author has had any other relationships, or has engaged in any other activities, that could be perceived to influence or have the potential to influence what is written in this work. The complete Disclosures of Potential Conflicts of Interest submitted by authors are always provided with the online version of the article.
References
- 1.Rankin EA, Alarcon GS, Chang RW, Cooney JLM, Costley LS, Delitto A, et al. ; NIH Consensus Panel NIH Consensus Statement on total knee replacement December 8-10, 2003. J Bone Joint Surg Am. 2004 Jun;86(6):1328-35 [DOI] [PubMed] [Google Scholar]
- 2.Fried LP, Bandeen-Roche K, Kasper JD, Guralnik JM. Association of comorbidity with disability in older women: the Women’s Health and Aging Study. J Clin Epidemiol. 1999 Jan;52(1):27-37 [DOI] [PubMed] [Google Scholar]
- 3.Ayers DC, Franklin PD, Ploutz-Snyder R, Boisvert CB. Total knee replacement outcome and coexisting physical and emotional illness. Clin Orthop Relat Res. 2005 Nov;(440):157-61 [DOI] [PubMed] [Google Scholar]
- 4.Farquhar S, Snyder-Mackler L. The Chitranjan Ranawat Award: The nonoperated knee predicts function 3 years after unilateral total knee arthroplasty. Clin Orthop Relat Res. 2010 Jan;468(1):37-44 Epub 2009 May 27 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Escobar A, Quintana JM, Bilbao A, Azkárate J, Güenaga JI, Arenaza JC, Gutierrez LF. Effect of patient characteristics on reported outcomes after total knee replacement. Rheumatology (Oxford). 2007 Jan;46(1):112-9 Epub 2006 May 30 [DOI] [PubMed] [Google Scholar]
- 6.Novicoff WM, Rion D, Mihalko WM, Saleh KJ. Does concomitant low back pain affect revision total knee arthroplasty outcomes? Clin Orthop Relat Res. 2009 Oct;467(10):2623-9 Epub 2009 May 12 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rosal MC, Ayers D, Li W, Oatis C, Borg A, Zheng H, Franklin PD. A randomized clinical trial of a peri-operative behavioral intervention to improve physical activity adherence and functional outcomes following total knee replacement. BMC Musculoskelet Disord. 2011;12(1):226 Epub 2011 Oct 07 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Daltroy LH, Cats-Baril WL, Katz JN, Fossel AH, Liang MH. The North American spine society lumbar spine outcome assessment instrument: reliability and validity tests. Spine (Phila Pa 1976). 1996 Mar 15;21(6):741-9 [DOI] [PubMed] [Google Scholar]
- 9.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-83 [DOI] [PubMed] [Google Scholar]
- 10.Ware JE, Kosinski M, Bjorner JB, Turner-Bowker DM, Gandek B, Maruish ME. User’s manual for the SF 36v2® health survey. 2nd ed. Lincoln: QualityMetric Inc; 2007 [Google Scholar]
- 11.Franklin PD, Li W, Ayers DC. The Chitranjan Ranawat Award: functional outcome after total knee replacement varies with patient attributes. Clin Orthop Relat Res. 2008 Nov;466(11):2597-604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lingard EA, Riddle DL. Impact of psychological distress on pain and function following knee arthroplasty. J Bone Joint Surg Am. 2007 Jun;89(6):1161-9 [DOI] [PubMed] [Google Scholar]
- 13.Hawker GA, Wright JG, Coyte PC, Williams JI, Harvey B, Glazier R, Badley EM. Differences between men and women in the rate of use of hip and knee arthroplasty. N Engl J Med. 2000 Apr 6;342(14):1016-22 [DOI] [PubMed] [Google Scholar]
- 14.Charnley J. The long-term results of low-friction arthroplasty of the hip performed as a primary intervention. 1972. Clin Orthop Relat Res. 1995 Oct;(319):4-15 [PubMed] [Google Scholar]
- 15.Katz JN, Wright EA, Baron JA, Losina E. Development and validation of an index of musculoskeletal functional limitations. BMC Musculoskelet Disord. 2009;10:62 Epub 2009 Jun 06 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Franklin PD, Allison JJ, Ayers DC. Beyond joint implant registries: a patient-centered research consortium for comparative effectiveness in total joint replacement. JAMA. 2012 Sep 26;308(12):1217-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Disclosure of Potential Conflicts of Interest