

Abstract
An important step in advancing global health through informatics is to understand how systems support health professionals to deliver improved services to patients. Studies in several countries have highlighted the potential for clinical information systems to change patterns of work and communication, and in particular have raised concerns that they reduce nurses’ time in direct care. However measuring the effects of systems on work is challenging and comparisons across studies have been hindered by a lack of standardised definitions and measurement tools. This paper describes the Work Observation Method by Activity Time (WOMBAT) technique version 1.0 and the ways in which the data generated can describe different aspects of health professionals’ work. In 2011 a revised WOMBAT version 2.0 was developed specifically to facilitate its use by research teams in different countries. The new features provide opportunities for international comparative studies of nurses’ work to be conducted.
Introduction
Clinical information system interventions, from electronic nurse documentation to computerised ordering and electronic medication management systems, are reported as influencing nurses’ patterns of work1–4. Attempts to understand and measure the nature of these changes and their subsequent impact on the work and care outcomes of nurses have used a variety of methods1–3.
Early work focused on the application of work sampling methods, but these have been shown to be limited in their ability to accurately quantify time spent on particular categories of nurses’ work5. Time and motion studies provide a more accurate estimate of time distribution. In essence this method requires development of a classification of categories of work tasks and through direct observation the amount of time spent on individual work tasks is recorded.
Practical challenges in recording work task times using paper and pencil methods prompted the design of electronic tools to capture data4,6,7. However a limitation of these tools was a failure to account for the collaborative and multi-dimensional nature of health professionals’ work.
Approach: Design of the Work Observation Method By Activity Timing (WOMBAT version 1.0)
In 2006 we developed the Work Observational Method by Activity Timing (WOMBAT)8,9 technique in order to measure not only what health professionals were doing, but how and with whom they completed tasks. Further, unlike previous methods, the data collection tool designed to support this method captured interruptions to work and multi-tasking. Previous methods had either not considered tasks conducted in parallel4 or selected to deal with this issue by asking observers to identify and record the ‘primary’ task7.
The WOMBAT method requires trained researchers to shadow individual clinicians and record four dimensions of their work: What task is underway, with whom the task is being completed, where is the clinician completing the task and what information resource, if any, is used. Mutually exclusive definitions of each work task have been prepared and those developed for nurses’10, doctors’11 and pharmacists’12 work have been detailed elsewhere.
Figure 1 presents a screenshot of the WOMBAT data collection tool. The left hand side lists 10 broad work tasks, some of which have drop down menus for greater detail. The right hand side allows observers to record who the task was completed with, whether the nurse was on the ward at the time and what type of information tool was involved in the task (e.g. permanent patient medical record; computer). When tasks are interrupted these are recorded using the ‘interrupt’ button and tasks being conducted in parallel “multi-tasking”, for example speaking with a colleague while dressing a wound, are also recorded. Interrupted tasks remain as tabs at the bottom of the screen and may be reactivated when the clinician returns to an interrupted task.
Figure 1.
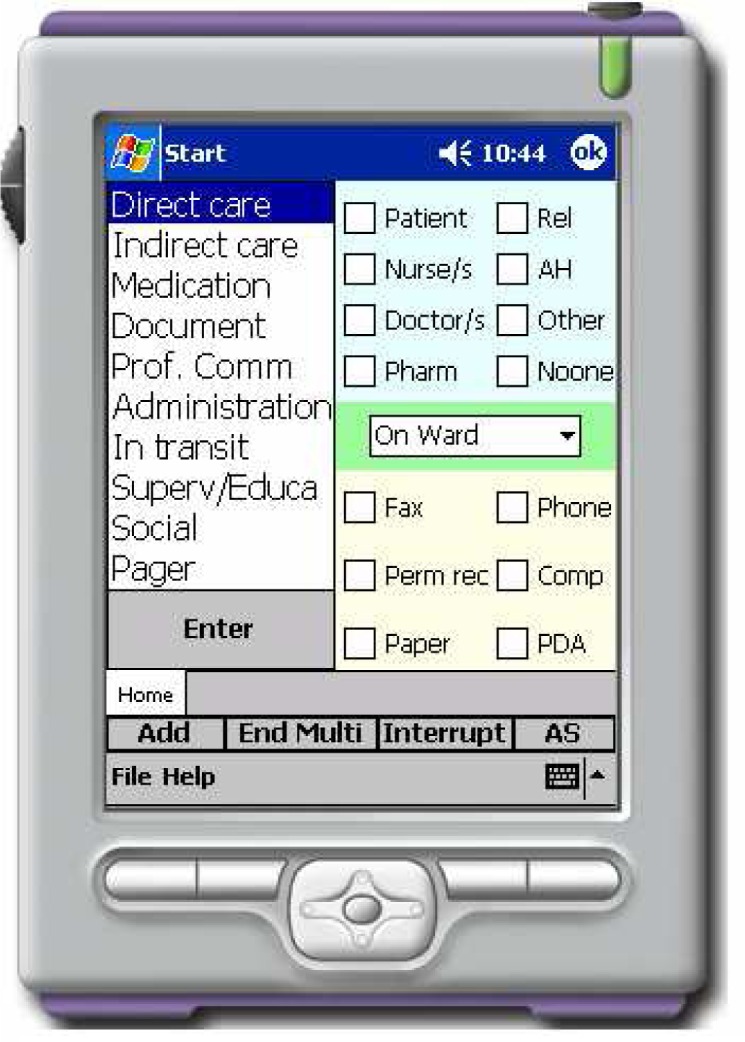
WOMBAT version 1.0 PDA data collection tool
The software was originally developed for an HP iPAQ rx3000 Pocket PC running Windows Mobile 2003 with an SD card expansion slot. The PDA program was developed in Visual C# using the .NET Compact Framework v1.0. Using ActiveSync enabled the use of SQL and the synchronization of multiple PDA databases with one central database on a PC.
Assessing changes to work and communication patterns
The WOMBAT technique has been applied in a range of studies to answer questions about health professionals’ work and communication patterns. These have included studies to quantify Australian physicians’11,13, nurses’10,14 and pharmacists’ 12 work patterns; and studies of Canadian health professionals 15–18. These studies have demonstrated the ways the data produced using the WOMBAT technique allows examination of multiple aspects of a clinician’s work as outlined in Table 1.
Table 1.
Measures which can be used to develop a profile of work and communication patterns pre and post an intervention
| Measures of work and communication which can be generated from WOMBAT datasets | Examples from published studies using WOMBAT | Examples of research questions which can be addressed |
|---|---|---|
| Proportion of total observation time spent in particular categories of tasks | Hospital physicians were found to spend the greatest proportion of their time (33%) in professional communication11. ICU nurses spent 39% in professional communication 15. Nurses spent an average of 16.9% of their time in medication tasks10. |
Provides an indication of whether clinicians shift to spend more or less time in particular broad categories of work following an intervention or between different groups. It can answer questions such as do nurses spend less time in direct care following an intervention compared to baseline. The proportion of time will be influenced by both frequency and length of task time. |
| The average or median length of time spent in an individual task | Pharmacists on wards with CPOE spent on average 43.7 seconds per task compared to 1 minute and 16 seconds for wards without CPOE12. When not interrupted emergency physicians spent an average of 3 minutes and 10 seconds on each direct care task13. |
This measure indicates whether particular types of tasks may have become more efficient, i.e. nurses spend less time per task following an intervention. It also provides a measure of the rapidity of task changing by clinicians. |
| Number of tasks completed in specific time periods | 27% of all tasks completed by pharmacists on a hospital ward with an electronic medication system was medication chart review12. | This measure indicates how frequently specific tasks are conducted and should be considered in relation to the length of these individual tasks. For example, documentation tasks generally take longer per task than other tasks but occur less frequently. |
| Proportion of time spent undertaking specific types of tasks in specific locations | 75.1% of ward doctors’ work was spent on the ward11. | This answers questions about what work is done where. For example, the proportion of time spent in professional communication at the nurses’ work station. |
| Proportion of time spent with other health professionals, patients or alone | 8% of nurses’ time was spent in communication with a doctor9. 83% of hospital pharmacists’ time on a ward with CPOE was spent alone compared to 73% for pharmacists on wards without CPOE 12. |
This answers questions about how much collaborative work is undertaken, with whom and where. |
| Proportion of tasks completed using specific information tools | 6% of doctors’ tasks on a hospital ward involved the telephone11. | This answers questions about the role of specific information sources such as paper medical records, computers etc. in completing specific types of tasks. |
| Rate of interruptions to work per hour | Emergency physicians were interrupted on average 6.6 times per hour and 11% of all tasks were interrupted13. Physicians in an ICU were interrupted 3.8 times per hour while ICU nurses were interrupted 3.3 times per hour 15. The greatest proportion of all interruptions to nurses on wards occurred when they were undertaking medication tasks9. |
This measure assesses the interruptive nature of work and has important safety implications given the established relationship between errors and interruptions 19. Examination of the types of tasks being interrupted assists in determining the extent to which interruptions increase risk. |
| Proportion of tasks conducted in parallel | Hospital doctors spent 20% of their time multi-tasking11. | Addresses questions about the complexity of work and by examination of the types of tasks involved in multi-tasking can provide insights into whether this type of work pattern might introduce increased risk of error. |
Revised Work Observation Method by Activity Timing (Version 2.0)
In 2011 we re-designed the WOMBAT data collection tool software and created new functionality with the specific aim of allowing the tool to be readily shared by research teams across the world. These features include the ability to configure observational studies using different dimensions and variables, and enhanced functionality to examine interruptions and multi-tasking in more detail. In particular, attention was paid to health informatics researchers’ calls for improved standardisation in the methods used to conduct time and motion studies20. Zheng et al20 reviewed previous time and motion studies and developed a Suggested Time and Motion Procedures (STAMP) checklist to guide future researchers. The new version of the WOMBAT tool was designed to create the capacity to collect all the suggested data elements while allowing research teams the flexibility to address a range of research questions about work and communication patterns.
Figure 2 shows the new WOMBAT interface design. In this example, four dimensions (what task, with whom, how and where the task is being completed) have been configured, but new users can input different dimensions as well as different variable names. On the right hand side Figure 2 shows a multi-task underway and also shows the previously completed ‘medication task’. Figure 3 shows two tasks which have been interrupted (social task and direct care) and one active task (professional communication with a doctor on the ward). When the nurse being observed returns to the interrupted task the researcher touches the relevant interrupted task in order for it to be resumed. For each task the original starting time is listed on the screen and this assists the observer to keep track of the sequence of tasks.
Figure 2.
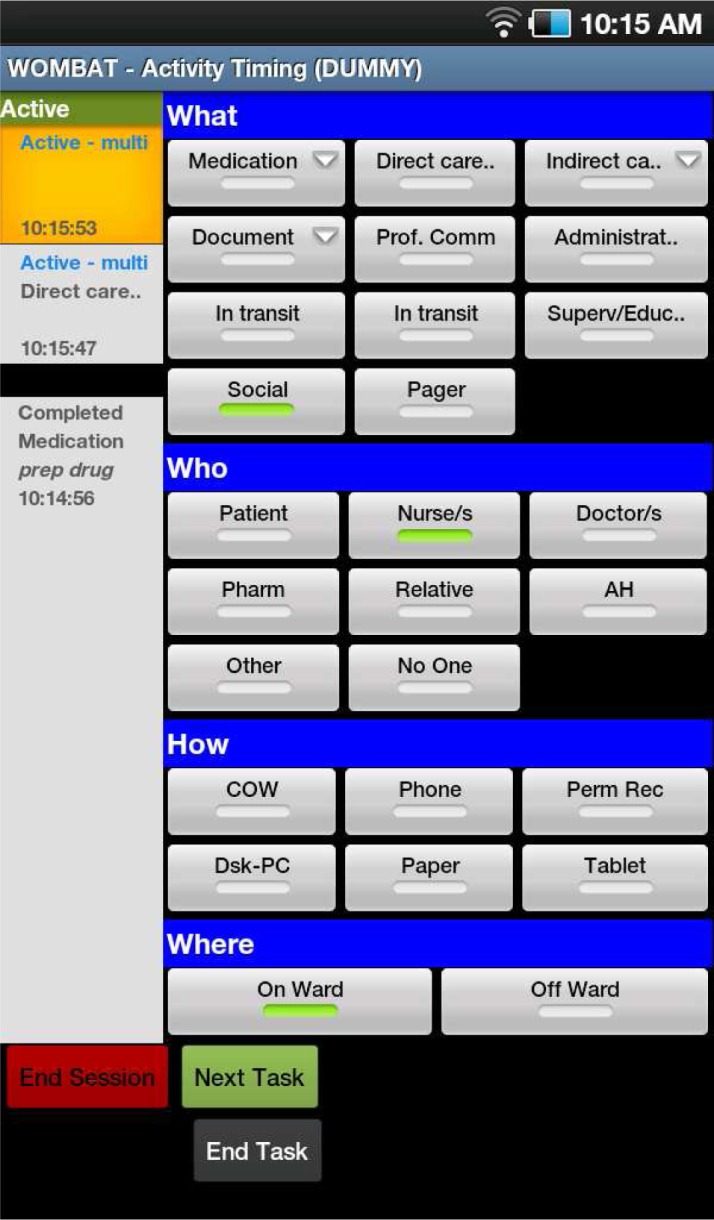
WOMBAT version 2.0 showing multi-tasking
Figure 3.
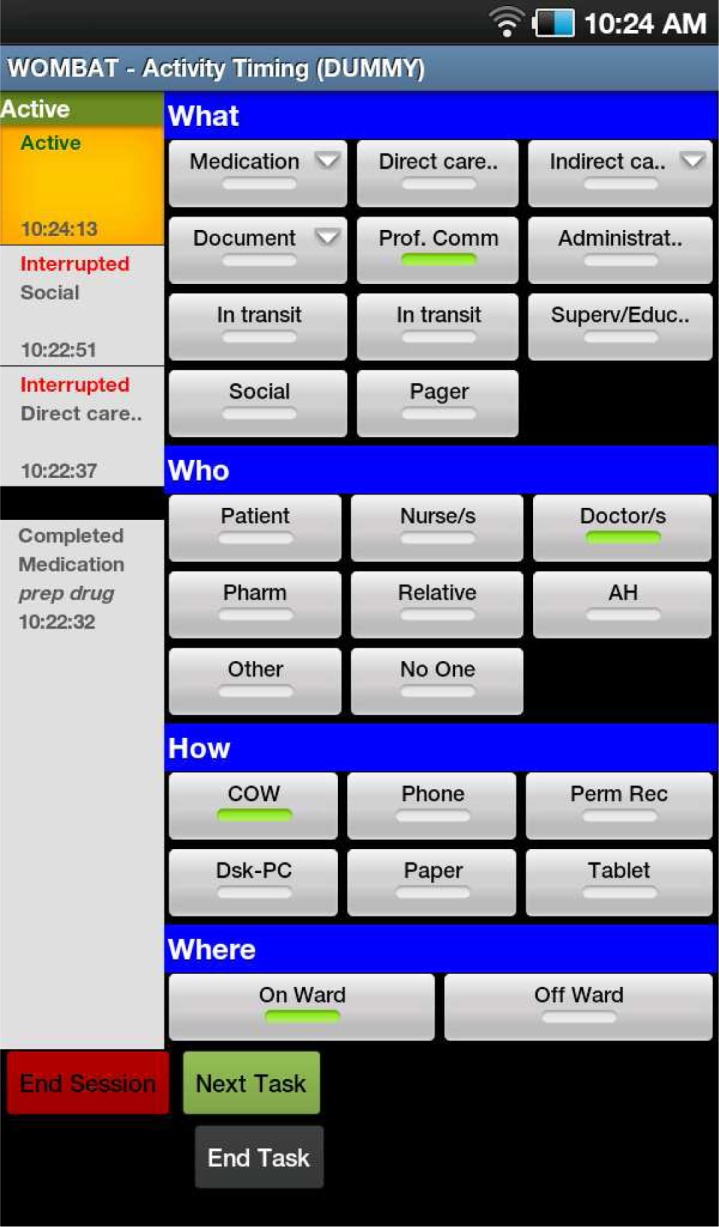
WOMBAT version 2.0 showing two interrupted tasks
Version 2.0 has been developed for a tablet with the Android operating system running the WOMBAT application. Currently we are using Samsung Galaxy Tab 7” devices. A web application server running the Apache Web Server and a Ruby on Rails application on a Linux Operating System has been used. Observers record sessions using the tablet and then, using the tablet's built in wireless connectivity to connect to an Internet service, transmit the recorded session data via a secure HTTP connection to the WOMBAT web application server. The web server accepts (authenticated) connections from the tablets, processes the incoming data and stores it in the local database. When this process completes successfully the web server responds with a message that indicates that the tablet application can clear the session records it currently has stored on the device.
A redesign of the WOMBAT database has increased the capacity to undertake more sophisticated analyses and to examine new measures. These include examining the sequence of tasks in order to assess changes in work flow rather than viewing tasks in isolation. Automatic calculation of the fragments of time for interrupted tasks assists researchers to examine the impact that interruptions have on, for example, task completion times13. Additional work is underway to develop an online statistical processing module which will further enhance consistency of analysis approaches which can be complex (see for example13), and also to allow real-time data analysis following completion of the observational sessions.
Conclusion
There is much still to learn about the complex ways in which the introduction of health informatics interventions may impact on the work and communication patterns of nurses and other health professionals. The availability of standardised research methods and tools provides opportunities to make substantial advances in our knowledge by allowing comparisons across studies. Early comparison studies using the WOMBAT in Australia and Canada15 have shown that this is possible and increases our ability to draw robust conclusions. The revised WOMBAT allows for multiple measures of work and communication patterns to be measured and creates valuable datasets against which to test more complex hypothesises about how interventions affect the work of different professional groups in different ways. Sharing this tool with international research teams provides an avenue for large comparative studies which have not previously been possible.
Acknowledgments
Thanks to Raul Carrizo, Georgina Edwards, Shuqian Hon, Sean McCarthy, Spencer Wu, and Veronica Luke who made important contributions to the design of WOMBAT version 2.0. This work was supported by an Australian Research Council Discovery Grant DP110100090.
References
- 1.Kossman S, Scheidenyhelm S. Nurses' perceptions of the impact of electronic health records on work and patient outcomes. CIN: Computers Informatics Nursing. 2008;26(2):69–77. doi: 10.1097/01.NCN.0000304775.40531.67. [DOI] [PubMed] [Google Scholar]
- 2.Poissant L, Pereira J, Tamblyn R, Kawasumi Y. The impact of electronic health records on time efficiency of physicians and nurses: A systematic review. J Am Med Inform Assoc. 2005;12(5):505–516. doi: 10.1197/jamia.M1700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Breslin S, Greskovich W, Turisco F. Wireless technology improves nursing workflow and communications. Computers, Informatics, Nursing. 2004;22(5):275–281. doi: 10.1097/00024665-200409000-00007. [DOI] [PubMed] [Google Scholar]
- 4.Tang Z, Weavind L, Mazabob J, Thomas E, Chu-Weininger M, Johnson TR. Workflow in intensive care unit remote monitoring: A time-and-motion study. Crit Care Med. 2007;35(9):2057–2063. doi: 10.1097/01.ccm.0000281516.84767.96. [DOI] [PubMed] [Google Scholar]
- 5.Ampt A, Westbrook J, Creswick N, Mallock N. Comparison of self-reported and observational work sampling techniques to measure nurses' work. J Health Serv Res Policy. 2007;12(1):18–24. doi: 10.1258/135581907779497576. [DOI] [PubMed] [Google Scholar]
- 6.Lo H, Newmark L, RYoon C, et al. Electronic health records in specialty care: A time-motion study. J Am Med Inform Assoc. 2007;14(5):609–615. doi: 10.1197/jamia.M2318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pizziferri L, Kittler A, LA V, et al. Primary care physician time utilization before and after implementation of an electronic health record: A time-motion study. J Biomed Informatics. 2005;38:176–188. doi: 10.1016/j.jbi.2004.11.009. [DOI] [PubMed] [Google Scholar]
- 8.Westbrook J, Ampt A. Design, application and testing of the Work Observation Method by Activity Timing (WOMBAT) to measure clinicians’ patterns of work and communication. Int J Med Inform. 2009;78S:S25–S33. doi: 10.1016/j.ijmedinf.2008.09.003. [DOI] [PubMed] [Google Scholar]
- 9.Westbrook JI, Ampt A, Williamson M, Nguyen K, Kearney L. Methods for measuring the impact of health information technologies on clinicians' patterns of work and communication. In: Kuhn KA WJ, Leong T, editors. Medinfo 2007. Vol. 2. Amsterdam: IOS Press; 2007. pp. 1083–1087. [PubMed] [Google Scholar]
- 10.Ampt A, Westbrook J. Measuring nurses' time in medication related tasks prior to the implementation of an electronic medication management system. In: Westbrook J, Coiera E, Callen J, Aarts J, editors. Information Technology in Health Care 2007. Vol. 130. Amsterdam: IOS Press; 2007. pp. 157–168. [PubMed] [Google Scholar]
- 11.Westbrook JI, Ampt A, Kearney L, Rob MI. All in a day's work: an observational study to quantify how and with whom doctors on hospital wards spend their time. Med J Aust. 2008;188(9):506–509. doi: 10.5694/j.1326-5377.2008.tb01762.x. [DOI] [PubMed] [Google Scholar]
- 12.Lo C, Burke R, Westbrook J. Comparison of pharmacists’ work patterns on hospital wards with and without an electronic medication management system (eMMS) J Pharm Pract Res. 2010;40(2):108–112. [Google Scholar]
- 13.Westbrook J, Coiera E, Dunsmuir WTM, et al. The impact of interruptions on clinical task completion. Quality and Safety in Health Care. 2010;19:284–289. doi: 10.1136/qshc.2009.039255. [DOI] [PubMed] [Google Scholar]
- 14.Westbrook JI, Braithwaite J, Georgiou A, et al. Multimethod evaluation of information and communication technologies in health in the context of wicked problems and sociotechnical theory. J Am Med Inform Assoc. 2007;14(6):746–755. doi: 10.1197/jamia.M2462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ballerman M, Shaw N, Mayes D, Gibney R, Westbrook J. Validation of the Work Observational Method By Activity Timing (WOMBAT) method of conducting time-motion observations in critical care settings: an observational study. BMC Med Inform Dec Mak. 2011;11 doi: 10.1186/1472-6947-11-32. 32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shaw N, Mador R, Ho s, et al. Understanding the impact of intensive care staff workflow due to the introduction of a critical care information system: a mixed methods research methodology. Studies in Health Technology & Informatics. 2009;143(186–191) [PubMed] [Google Scholar]
- 17.Ballerman M, Shaw N, Mayes D, Gibney R. Intensive care unit health care providers spend less time multitasking after the introduction of a critical care information system. 18th Annual Health Informations Conference 2010; Melbourne. pp. 6–10. [Google Scholar]
- 18.Shaw N, Ballerman MH, R, Ho S, Mayes D, Gibney N. Intensive care unit nurse workflow during shift change prior to the introduction of a critical care clinical information system. Electronic Journal of Health Informatics. 2011;6(1) http://www.ejhi.net/ojs/index.php/ejhi/article/view/119. [Google Scholar]
- 19.Westbrook J, Woods A, Rob MI, Dunsmuir WTM, Day R. Association of interruptions with increased risk and severity of medication administration errors. Arch Intern Med. 2010;170(8):683–690. doi: 10.1001/archinternmed.2010.65. [DOI] [PubMed] [Google Scholar]
- 20.Zheng K, Guo M, Hanauer D. Using the time and motion method to study clinical work processes and workflow: methodological inconsistencies and a call for standardized research. J Am Med Inform Assoc. 2011;18:704–710. doi: 10.1136/amiajnl-2011-000083. [DOI] [PMC free article] [PubMed] [Google Scholar]