

Abstract
Background
The short-term safety of and blood pressure changes after withdrawing hypertension treatment in older adults in preparation for clinical trials have not been well established.
Methods
Participants were enrolled in a clinical trial and antihypertensive medications were tapered over 3 weeks (week 1: reduction by 25%–50%; week 2: 50%–75%, week 3: off). Blood pressure was measured at the initial visit and after stopping all antihypertensive therapy (personnel) and twice a day during the taper phase (provided monitor). Trend analyses and linear models were used to assess changes in blood pressure.
Results
All participants (n = 53, mean age = 71 years, total of 1158 readings) successfully tapered their medications with no symptoms. Only 2% of the readings exceeded 180/100 mm Hg, but none were consecutive. Blood pressure gradually increased with an overall increase of 12/6 mm Hg, 95% confidence interval (4/1, 21/11). The daily increase in blood pressure was 0.2 mm Hg (standard error = 0.1) in both the systolic and diastolic blood pressure. Increases in systolic and diastolic blood pressure were comparable for all antihypertensive classes (P > .05 for all).
Conclusion
Short-term (<3-4 weeks) withdrawal of antihypertensive therapy in older adults with hypertension is safe and is associated with mild increases in blood pressure.
Keywords: Antihypertensive withdrawal, trajectory, older adults
Introduction
The prevalence of hypertension and the use of antihypertensive medications have been progressively increasing over the last few decades, especially in older adults.1 It is estimated that close to 84% of all hypertensive older adults were receiving antihypertensive medication in 2009 to 2010.1 The high number of treated hypertensive individuals makes it difficult to conduct clinical trials of hypertension therapy, as it is prudent to stop treatment prior to enrollment in such studies. Although such a practice has been commonly used in hypertension clinical trials, there is no evidence on its safety in older adults. Blood pressure fluctuation and variability increases with aging.2 Therefore, the safety of this practice in hypertension clinical trials in older adults may pose a limitation to the successful recruitment and enrollment in clinical trials. Older adults are already underrepresented in clinical research, which poses significant limitation to the appropriate management of older adults in clinical practice.3
Except for clonidine,4,5 studies have suggested that the blood pressure change after withdrawing antihypertensive therapy is variable and tends to be small.6 In fact, some patients do not experience any increase in blood pressure after stopping their antihypertensive medications. For example, in the second Australian National Blood Pressure study, 18% of patients attending a family practice remained normotensive after withdrawing medication for up to 76 weeks (median, 4).7 The trajectory of blood pressure change during and after withdrawal of blood pressure treatment in older adults is not known.
We therefore aimed at assessing the safety of withdrawing antihypertensive therapy in a sample of older adults being considered for enrollment in a clinical trial and studying the trajectory of blood pressure change over the withdrawal period.
Methods
Participants for this study were being enrolled in a hypertension cognitive clinical trial (The Antihypertensives and Vascular, Endothelial and Cognitive Function Trial or AVEC). The overall experimental design of this trial is described elsewhere.8 Participants were recruited from the greater Boston area and evaluated at the cardiovascular research laboratory at the Institute for Aging Research at Hebrew SeniorLife and Harvard Medical School. The Institutional Review Board at Hebrew SeniorLife approved the study, and all participants provided written informed consent. Patients were screened for eligibility (initial visit) and were asked to withdraw their antihypertensive medications under supervision (taper phase), and then asked to return for randomization into the study (pre-randomization visit). Blood pressure was measured using the American Heart Association guidelines by trained personnel during the initial and the pre-randomization visits where two readings were obtained in the sitting position.
Antihypertensive Medication Withdrawal
Individuals who were currently receiving antihypertensive medications were eligible to participate if the participant and the primary care provider were willing to taper their medications. Participants were provided with a portable automated blood pressure monitor. Study personnel trained each participant on the use of the blood pressure monitor: Participants were asked to measure their blood pressure in front of the study personnel and to repeat the process until they successfully and accurately performed the blood pressure measurements. The median difference between the personnel and the participant measurement after training was 2 mm Hg higher for systolic blood pressure (SBP; mean, 1 mm Hg; standard error [SE], 4 mm Hg) and 3 mm Hg higher for diastolic blood pressure (DBP; mean, 2 mm Hg, SE = 4 mm Hg). All participants received written instructions on tapering and discontinuation of antihypertensive medications, description of symptoms associated with possible adverse events, and familiarization with the study protocol. They were instructed to share this information with their spouses or other members of their households. They were asked to measure blood pressure two times a day (morning and before sleep) and record them into a diary. The subjects were asked to call the investigators (by phone or pager) anytime that they had two consecutive readings exceeding 180 mm hg SBP and/or 100 mm Hg DBP or had any unexpected discomfort, dizziness, or headaches. Contact by the study personnel was twice weekly for review of blood pressures. The timeline for medication was a decrease by 25% to 50% during week 1, 50% to 75% during week 2, and 100% for week 3. Subjects with significant blood pressure elevations (SBP >180/100 mm Hg) for at least two consecutive times or who developed hypertension-related symptoms were excluded (failed taper), asked to resume their usual dose of antihypertensive medications, and were referred back to their primary care physician for chronic blood pressure management as usual.
Statistical Analysis
Participants’ blood pressures were averaged over the initial visit, pre-randomization visit, and daily or weekly over the tapering phase. Trend analysis was conducted using analysis of variance and generalized linear models. Weekly blood pressure averages were compared with initial blood pressure, and significance was Bonferroni-adjusted for multiple comparisons. Daily blood pressure trajectories were also calculated, and a fitted linear model was used to calculate a daily increase in blood pressure with a 95% confidence interval (CI). Finally, mixed models for repeated correlated measures were used to compare if the pre-study class of antihypertensive medication has a relation with the blood pressure trajectory. Using the mixed model, we tested the hypothesis that there is a significant increase in blood pressure in each subgroup of antihypertensive classes. We adjusted this analysis to age, gender, and race. All analyses were conducted using SAS (v.9.2; Cary, NC) statistical package.
Results
Of the 63 eligible participants, 53 agreed to participate and taper their antihypertensive medications. Reasons for not enrolling were not related to the medication taper (severe elevation in blood pressure during screening [>180/100], new onset back pain, time constraints, and personal reasons) except in one potential subject whose primary care provider refused the tapering plans for undisclosed reasons. Basic characteristics of the enrolled sample are shown in Table 1. The mean number of antihypertensive medications was 1.5 (median, 1; standard deviation, 0.6). The majority of the patients were receiving a diuretic (43%) or angiotensin-converting enzyme inhibitor (45%).
Table 1.
Socio-demographic, clinical, and blood pressure characteristics of the study sample
| Measure | Mean (Standard Deviation) or % |
|---|---|
| N | 53 |
| Age, years | 1 (7) |
| Women, % | 64% |
| African American, % | 26% |
| High school education or lower, % | 20% |
| Less than 12 years of education, % | 17% |
| Body mass index, Kg/m2 | 19.3 (6.2) |
| Blood pressure and heart rate sitting | |
| Systolic blood pressure, mm Hg | 152 (16) |
| Diastolic blood pressure, mm Hg | 83 (9) |
| Heart rate, beats per minute | 66 (11) |
| Medical diagnosis | |
| Coronary heart disease, % | 49% |
| Past cancer, % | 19% |
| Osteoarthritis, % | 34% |
| Pre-study antihypertensive class | |
| Diuretics,% | 43% |
| Angiotensin-converting enzyme inhibitor, % |
45% |
| Angiotensin receptor blockers, % | 15% |
| Calcium channel blockers, % | 13% |
| Beta blockers, % | 34% |
During the taper process, all participants successfully measured their blood pressure and provided the information to the study personnel. A total of 1158 readings were obtained and analyzed. The mean number of reading per participant was 31 over 3 weeks (expected number was 42; one participant reported 56 readings), with a completion rate of the blood pressure diary of 74%. In all the home measurements, only 2% of the readings exceeded the 180 mm Hg for SBP or 100 mm Hg for DBP, as shown in Figure 1, and none reported two consecutive readings above these thresholds. None of the participants reported headaches, dizziness, visual changes, or focal weakness during the tapering phase.
Figure 1.
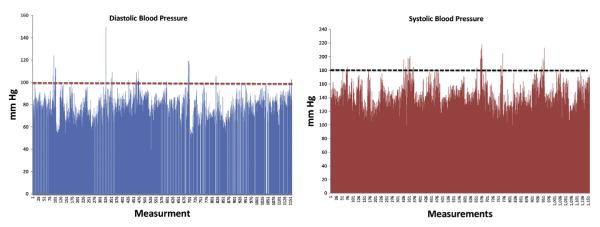
Blood pressure dispersion during the taper phase, measured twice daily in those enrolled in the study who underwent the gradual taper of antihypertensive medications.
Over the taper period, blood pressure gradually increased as the antihypertensive load decreased. As shown in Table 2, the weekly increase in blood pressure became statistically significant only when the load was 0 (off antihypertensive therapy). The overall increase in SBP was 12 mm Hg (95% CI [4,21]) and in DBP was 6 mm Hg (95% CI [1,11]). The daily increase in blood pressure was gradual with an average increase by 0.2 mm Hg (SE, 0.1) in both the SBP and DBP, as shown in Figure 2. We did not observe any differences by the antihypertensive class the participants were receiving prior to enrollment. As shown in Figure 3, increases in SBP and DBP were comparable for all classes.
Table 2.
Weekly blood pressure change from initial visit to pre-randomization visit
| Initial Visit∥ | Week 1¶ | Week 2¶ | Week 3¶ | Pre-randomization∥ | P Trend | |
|---|---|---|---|---|---|---|
| Antihypertensive load | 100% | 75%–50% | 25%–50% | 0% | 0% | |
| Systolic blood pressure (mean ± standard error) in mm Hg | 139 ± 2 | 142 ± 2 | 144 ± 2 | 151 ± 3* | 152 ± 2‡ | .004 |
| Diastolic blood pressure, (mean ± standard error) in mm Hg | 77 ±1 | 80± 2 | 80± 1 | 83± 2† | 83 ± 1§ | .0035 |
Blood pressure measurements that are significantly different from the baseline visit blood pressure measurement are marked in the table
P = .03.
P = .0005
P = .04
P = .004
Measured by study personnel.
Measured by subject using the provided blood pressure monitor.
Figure 2.
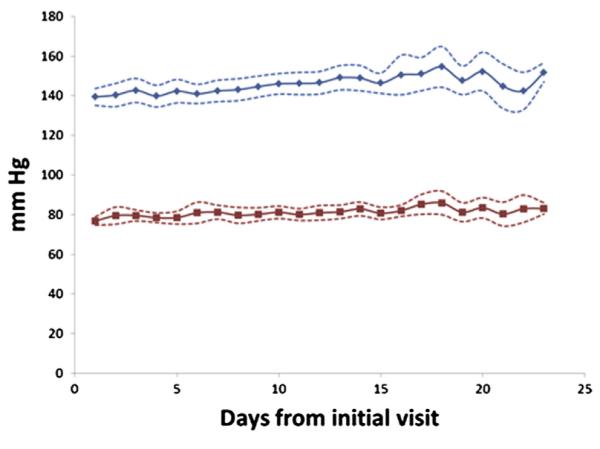
Trajectory of daily blood pressure over time in the study participants. Solid lines are the mean blood pressure at each day and dotted lines are the 95% confidence interval around the mean. Fitted linear regression showed overall increase in systolic blood pressure by 0.2 (SE, 0.1) mm Hg per day (P = .06) and 0.2 (SE, 0.1) mm Hg per day (P = .02) in diastolic blood pressure.
Figure 3.
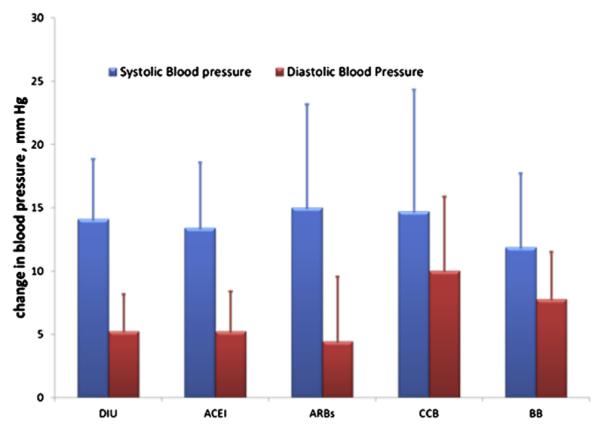
Demographic-based adjusted increase in blood pressure from initial visit (on antihypertensive medications) to pre-randomization visit (off antihypertensive medications). ACEI, Angiotensin converting enzyme inhibitors; ARB, Angiotensin receptor blockers; BB, beta blockers; CCB, calcium channel blockers; DIU, diuretics. Values are the least square means adjusted for age, gender, and race. P values are from comparing each class with the rest of the population of antihypertensive medications (DIU, SBP P value: .60/DBP P value: .30; ACE, 0.16/0.90; ARB, 0.19/0.74; CCB, 0.99/0.99; BB, 0.75/0.79).
Discussion
This study suggests that in older adults with hypertension, short-term withdrawal of antihypertensive medications is associated with small increases in SBP and DBP, and is generally safe, achievable, and well-tolerated. To our knowledge, this is the first study to show that withdrawing antihypertensive medications in preparation for a clinical trial in older adults is possible. A prior study in older adults (mean age, 75 years) with hypertension demonstrated no increase in cardiovascular events or mortality associated with antihypertensive withdrawal.9 Many factors may have increased the safety of our protocol: the use of gradual taper with safety triggers, the frequent home and office monitoring, and continuous contact with the study personnel are all good clinical and research practice. Following such a protocol may provide an important alternative to excluding treated older adults from future hypertension clinical trials.
Prior studies suggest that there is a period after stopping antihypertensive medication when blood pressure is mildly increased, but eventually, a significant number of patients with hypertension may relapse.10 Therefore, studies that use a withdrawal protocol should keep the period to a minimum. In our study, we used 3 weeks with 1 week off antihypertensive therapy. Beyond the 3- to 4-week period, it is not known if the blood pressure will abruptly increase or continue the mild gradual daily increase. We therefore cannot recommend a longer withdrawal period.
We did not observe differences by antihypertensive classes. Our sample size limits our subgroup analyses. It is possible that using a gradual taper has rendered the class differences, for example with the use of beta-blockers, less likely. We did not have any antihypertensive medication class that is known to be associated with an abrupt withdrawal syndrome.11 Extra caution should be exercised in these cases.
In a prior analysis, we found that after tapering antihypertensive medications, we were able to achieve blood pressure control with a lower antihypertensive load.12 We defined the antihypertensive load as the sum of the ratio of the current daily dosage divided by the maximum recommended daily dosage for each medication. The maximum daily dosage of each agent as indicated for hypertension was obtained from drug database. This may suggest that tapering antihypertensive medication may also provide an additional benefit of decreasing the antihypertensive load needed to achieve similar blood pressure control. Clinicians may consider reviewing antihypertensive therapy on a regular basis.
The main limitation to this study is the sample size. We, however, had an extensive number of blood pressure measurements (>1000). Despite this limitation, it is the first evidence suggesting that older adults on treatment can be included in hypertension clinical trials after undergoing a slow withdrawal protocol. Another limitation is that our sample has a relatively lower body mass index than the general older population, and many were receiving angiotensin-converting enzyme inhibitors and fewer receiving calcium channel blockers. This may limit generalizability to the clinical population.
Conclusion
A slow taper and short-term withdrawal of antihypertensive therapy in older adults with hypertension are possibly safe and are associated with mild increases in blood pressure. Larger studies are needed to confirm the safety of this withdrawal protocol.
Acknowledgments
This work (Dr. Hajjar and the AVEC trial) was supported by grant1 K23 AG030057 from the National Institute on Aging and a generous donation from Hinda Marcus to the Cardiovascular Research Laboratory at Hebrew SeniorLife and Harvard Medical School. The study was also registered in ClinicalTrials.gov (NCT00605072).
Footnotes
Conflict of interest: None.
References
- 1.Gu Q, Burt VL, Dillon CF, Yoon S. Trends in antihypertensive medication use and blood pressure control among United States adults with hypertension: the National Health and Nutrition Examination Survey, 2001 to 2010. Circulation. 2012;126:2105–14. doi: 10.1161/CIRCULATIONAHA.112.096156. [DOI] [PubMed] [Google Scholar]
- 2.Veerman DP, Imholz BP, Wieling W, Karemaker JM, van Montfrans GA. Effects of aging on blood pressure variability in resting conditions. Hypertension. 1994;24:120–30. doi: 10.1161/01.hyp.24.1.120. [DOI] [PubMed] [Google Scholar]
- 3.Herrera AP, Snipes SA, King DW, Torres-Vigil I, Goldberg DS, Weinberg AD. Disparate inclusion of older adults in clinical trials: priorities and opportunities for policy and practice change. Am J Public Health. 2010;100(Suppl 1):S105–12. doi: 10.2105/AJPH.2009.162982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Clonidine withdrawal and hypertension. Drug Ther Bull. 1977;15:99–100. [PubMed] [Google Scholar]
- 5.Goldberg AD, Wilkinson PR, Raftery EB. The overshoot phenomenon on withdrawal of clonidine therapy. Postgrad Med J. 1976;52(Suppl 7):128–36. [PubMed] [Google Scholar]
- 6.Nelson M, Reid C, Krum H, McNeil J. A systematic review of predictors of maintenance of normotension after withdrawal of antihypertensive drugs. Am J Hypertens. 2001;14:98–105. doi: 10.1016/s0895-7061(00)01246-2. [DOI] [PubMed] [Google Scholar]
- 7.Nelson MR, Reid CM, Krum H, Ryan P, Wing LM, McNeil JJ. Short-term predictors of maintenance of normotension after withdrawal of antihypertensive drugs in the second Australian National Blood Pressure Study (ANBP2) Am J Hypertens. 2003;16:39–45. doi: 10.1016/s0895-7061(02)03143-6. [DOI] [PubMed] [Google Scholar]
- 8.Hajjar I, Hart M, Milberg W, Novak V, Lipsitz L. The rationale and design of the Antihypertensives and Vascular, Endothelial, and Cognitive function (AVEC) trial in elderly hypertensives with early cognitive impairment: role of the renin angiotensin system inhibition. BMC Geriatr. 2009;9:48. doi: 10.1186/1471-2318-9-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ekbom T, Lindholm LH, Oden A, Dahlof B, Hansson L, Wester PO, et al. A 5-year prospective, observational study of the withdrawal of antihypertensive treatment in elderly people. J Intern Med. 1994;235:581–8. doi: 10.1111/j.1365-2796.1994.tb01265.x. [DOI] [PubMed] [Google Scholar]
- 10.Dannenberg AL, Kannel WB. Remission of hypertension. The ‘natural’ history of blood pressure treatment in the Framingham Study. JAMA. 1987;257:1477–83. doi: 10.1001/jama.257.11.1477. [DOI] [PubMed] [Google Scholar]
- 11.Peters RW, Hamilton BP, Hamilton J, Kuzbida G, Pavlis R. Cardiac arrhythmias after abrupt clonidine withdrawal. Clin Pharmacol Ther. 1983;34:435–9. doi: 10.1038/clpt.1983.194. [DOI] [PubMed] [Google Scholar]
- 12.Wan SH, Hart M, Hajjar I. A novel measurement index for antihypertensive medication burden and its use. Hypertension. 2009;54:e135–6. doi: 10.1161/HYPERTENSIONAHA.109.140681. [DOI] [PubMed] [Google Scholar]