

Abstract
Objective
African Americans have the highest rates of obesity in the United States. Engaging in recommended levels of physical activity (PA) reduces risk for obesity. Social and environmental supports for PA may be important to increase PA. This study hypothesized that PA would mediate the effects of neighborhood and social supports for PA on body mass index (BMI).
Method
Baseline data were collected from 434 underserved African American adults in the Positive Action for Today’s Health (PATH) trial. Features of the neighborhood environment (i.e., infrastructure for walking, access to services, and crime) and peer social support were measured with validated surveys. Moderate-to-vigorous PA (MVPA) was assessed based on 7-day accelerometry estimates (in minutes per day), and self-reported walking and exercise were obtained using the Four-Week Physical Activity History questionnaire.
Results
The sample was predominantly female (63%) and obese (MBMI = 30.88 kg/m2, SD = 8.43). Neither crime nor social support was significantly associated with either PA or BMI; thus, they were excluded from the final models. Infrastructure for walking predicted MVPA (B = 4.06, p = .01) and self-reported walking (B = 7.39, p = .03). A positive association between access to services and MVPA approached significance (B = 2.27, p = .06). MVPA (B = −0.07, p < .001) and self-reported walking (B = −0.02, p = .01) predicted BMI, but only MVPA mediated the effect of infrastructure for walking on BMI (B = −0.03, p = .04). No significant direct or indirect effects of predictors were found for self-reported exercise.
Conclusion
Findings suggest that MVPA is a mediator linking infrastructure for walking and BMI in underserved communities.
Keywords: social environment, physical activity, obesity, neighborhood walkability, African American
Obesity is a leading cause of morbidity and mortality in the United States. More than 30% of adults are obese, with African Americans disproportionately represented (Flegal, Carroll, Kit, & Ogden, 2012). Despite evidence that regular engagement in physical activity (PA) may prevent the development of overweight and obesity (Brock et al., 2009), most adults in the United States do not meet national recommendations for PA (Troiano et al., 2008). Lack of regular PA is particularly evident among African American adults (Prus, 2007). To address disparities in obesity, it is a public health priority to identify factors that promote higher levels of engagement in PA in African Americans.
In the present study, a bioecological framework was used to identify factors that are associated with positive health behaviors. This approach posits that health behaviors are influenced by conditions in the social and physical environment, in addition to individual factors (Bronfenbrenner, 1979; Bronfenbrenner & Ceci, 1994; McLeroy, Bibeau, Steckler, & Glanz, 1988; Spence & Lee, 2003). Indeed, accumulating evidence has indicated that environmental and social factors are important for promoting PA (Sallis et al., 2009; Trost, Owen, Bauman, Sallis, & Brown, 2002). These factors may be particularly important in underserved African American adults who experience limited access to health-promoting contexts and services (Gordon-Larsen, Nelson, Page, & Popkin, 2006). Further, similar environments may have different health impacts for African Americans than for other racial and ethnic groups (Hooker, Wilson, Griffin, & Ainsworth, 2005). The present study expands on a limited literature that examines the association of environmental and social factors with PA in under-served African American adults, and tests whether PA is a potential mechanism linking these factors with obesity.
One aspect of the environment that has received increased attention over the past decade is neighborhood walkability. Two features related to neighborhood walkability that have been shown to be consistently associated with PA in predominantly nonminority samples are infrastructure for walking (e.g., sidewalks, trails) and access to services within walking distance (Owen, Humpel, Leslie, Bauman, & Sallis, 2004; Sallis et al., 2009). Studies with ethnically diverse samples have also found associations between these neighborhood features and PA (Addy et al., 2004; King et al., 2005; Parks, Housemann, & Brownson, 2003). A limited number of studies have examined associations between the neighborhood environment and PA in African American adults, yielding inconsistent findings, but providing some support for the importance of neighborhood walkability for PA in this population (Casagrande, Whitt-Glover, Lancaster, Odoms-Young, & Gary, 2009). For example, some studies have found associations between features of neighborhood walkability (such as infrastructure for walking) and PA in African Americans, including engaging in recommended levels of PA and leisure-time PA (Ainsworth, Wilcox, Thompson, Richter, & Henderson, 2003; Heinrich et al., 2007); however, other studies have not (King et al., 2000; Rohm Young & Voorhees, 2003; Sanderson et al., 2003).
Another neighborhood feature—crime—has been frequently cited as a barrier to PA in qualitative studies (Eyler et al., 1998; Holman, Donovan, & Corti, 1996). However, quantitative evidence of this association has been mixed in both predominantly nonminority samples (Foster & Giles-Corti, 2008) and African American adults (Casagrande et al., 2009). Whereas some studies have found an association between crime and PA in minority samples, including African Americans (Addy et al., 2004; Eyler et al., 2003; Hannon, Sawyer, & Allman, 2012; Wilbur, Chandler, Dancy, & Lee, 2003), other studies have not (Bennett et al., 2007; Hooker et al., 2005; King et al., 2000; Rohm Young & Voorhees, 2003; Sanderson et al., 2003). Nonetheless, because safety concerns have been identified as a barrier to PA in qualitative studies, crime warrants further investigation, particularly in underserved African Americans.
Social support, defined broadly as resources and encouragement provided by others, has also been identified as an important correlate of PA (Trost et al., 2002). Social support can come from different sources, including family and friends, and can take various forms, including instrumental and tangible (e.g., direct assistance), informational (e.g., PA suggestions), and emotional (e.g., encouragement) support (Harley et al., 2009). The few studies that have examined associations between social support and PA in African Americans have suggested the importance of social support for PA, but findings have been inconsistent. For example, although there is some evidence that family support is particularly important for PA in African Americans (Komar-Samardzija, Braun, Keithley, & Quinn, 2012), other studies have found support provided by friends, not family, to be associated with PA in this population (Peterson & Cheng, 2011; Sharma, Sargent, & Stacy, 2005). Moreover, some previous studies have shown that social support provided by either family or friends is associated with PA in African American men (Hooker, Harmon, Burroughs, Rheaume, & Wilcox, 2011) and women (Eyler et al., 1999). Other studies, however, have not found support provided by both friends and family combined to be associated with PA (Bopp et al., 2006; Li et al., 2012). Thus, an understanding of the association between social support and PA remains limited in African American adults.
In summary, previous studies have shown that neighborhood walkability and social support are associated with higher levels of PA. However, less is known about these associations in under-served African American adults or about health behaviors, such as PA, as potential pathways through which environmental and social factors may be linked to obesity. Previous research with nonminority populations has provided mixed evidence that PA is a mediator of these associations. One study found that both objective and self-report measures of PA mediated linkages between neighborhood walkability and weight-related outcomes (Van Dyck et al., 2010). Other studies, however, have not found self-reported PA to be a mediator linking perceptions of the environment and social support with self-rated health (Poortinga, 2006a, 2006b). Additional research is needed to identify specific mechanisms that link environmental and social factors with obesity, particularly in underserved African American adults.
The purpose of the present study was to examine PA as a potential mediator of associations of neighborhood walkability and social support with obesity in African American adults as part of the Positive Action for Today’s Health (PATH) randomized trial (Coulon et al., 2012; Wilson et al., 2010). Three communities were identified and matched based on U.S. Census information (e.g., crime, PA, poverty, percent minority) and recruited to participate in the 24-month study. The primary aims of the trial were to compare a combined police-patrolled walking and social marketing intervention to a police-patrolled walking only or a walking-only intervention on increasing moderate-to-vigorous PA (MVPA) after 12 months and to examine the maintenance of effects over 24 months. Longitudinal data are not yet available; therefore, cross-sectional data were the focus of this study. Potential pathways through which environmental and social factors may influence obesity were examined by estimating the effects of neighborhood walkability, social support, and PA on body mass index (BMI) in the PATH sample at baseline. It was hypothesized that greater walkability and peer social support would be associated with increased time spent engaging in PA and lower BMI, and that greater PA would be associated with lower BMI. It was further hypothesized that PA would mediate associations of neighborhood walkability and social support with BMI. To better understand PA as a potential mechanism linking these factors with BMI, hypotheses were tested in a primary model, with accelerometry-assessed MVPA as a mediator, and, in secondary models, with self-reported walking and exercise as mediators.
Method
Study Design and Procedures
The PATH randomized trial is described in detail elsewhere (Coulon et al., 2012; Wilson et al., 2010). Assessments were conducted in each of the three communities at baseline as well as at 6, 12, 18, and 24 months. At baseline, each participant attended a 2-hr health screening during which height, weight, waist circumference, PA, and blood pressure were measured by trained research staff. Participants also completed survey assessments of psychosocial variables and provided demographic information, including age, sex, approximate annual income, education status, occupation status, and marital status. Participants signed informed consent and received a monetary incentive for their time.
Participants
Data were collected from a sample of 434 African American adults who resided in one of the three low-income communities identified and who were participating in the PATH trial. Two recruitment strategies were used. Participants were initially recruited from a random list of households in specified Census tracts in each targeted community via letters and telephone calls. Of the 1,986 households called, 770 did not answer. Of the 1,216 households reached, 581 persons declined and 635 persons were invited to participate. Of those who were invited to participate, 231 enrolled and provided baseline information. As a second recruitment method, volunteers were recruited using flyers, advertisements listed in local newspapers, and posters and banners placed in churches, schools, and at local businesses in each community (Wilson et al., 2010). Approximately 54% of the final sample was recruited using the random list of households and 46% was recruited through volunteer advertisements. Individuals were included in the PATH study sample if they met the following criteria: (a) African American (three of four grandparents of African heritage), (b) 18 years of age or older, (c) had no plans to move within 2 years, (d) had no medical condition that would limit participation in moderate intensity exercise, including life-threatening illness (e.g., immobile, severely disabled, bed-ridden), (e) were residing in specified Census areas within one of three identified communities, and (f) had controlled blood pressure (systolic < 180 mmHg systolic and diastolic < 110 mmHg) and blood sugar levels (nonfasting < 300 mg/dl and fasting ≤ 250 mg/dl). Participants were excluded if they answered affirmatively to any item on the Physical Activity and Readiness Questionnaire (Thomas, Reading, & Shephard, 1992), which indicated that they were unable to safely participate in moderate PA. The study was approved by the institutional review board at the University of South Carolina.
Measures of Environmental and Social Supports for PA
Neighborhood walkability
Items from three subscales of the Neighborhood Environment Walkability Survey (NEWS) were used to measure relevant aspects of neighborhood walkability (Saelens, Sallis, Black, & Chen, 2003). Scoring procedures, derived from a confirmatory factor analysis of the NEWS (Cerin, Saelens, Sallis, & Frank, 2006), provided the guiding framework for the construction of the subscales, which included infrastructure for walking (three items), land-use mix–access to services (five items), and crime (three items). The infrastructure for walking and access to services subscales were selected based on evidence that neighborhood features of walkability (e.g., sidewalks, trails) and access to destinations within walking distance are important for PA (Owen et al., 2004; Sallis et al., 2009). Because crime is often cited as a barrier to PA in underserved groups (Addy et al., 2004; Eyler et al., 1998), the crime subscale was also selected for investigation. Subscales elicited responses on a 4-point Likert scale. Example items for each subscale included: “There are sidewalks on most of the streets in my neighborhood” (infrastructure for walking), “There are many places to go within walking distance of my home” (access to services), and “There is a high crime rate in my neighborhood” (crime). Validity of the NEWS for measuring a number of neighborhood environment constructs has been established (Cerin, Conway, Saelens, Frank, & Sallis, 2009), with the survey correlated with geographic information systems (GIS) outcomes (Adams et al., 2009). Test–retest reliability is .58 (Saelens et al., 2003), with alpha reliabilities in the present study ranging from .67–.79.
Peer social support for PA
Items from the peer subscale of the Social Support for Exercise Habits Scale provided a measure of peer social support for PA (Sallis, Grossman, Pinski, Patterson, & Nader, 1987). The subscale elicited responses on a 5-point Likert scale to five items, such as “How often do your friends offer to exercise with you?” Criterion validity has been established with self-reported PA (Sallis et al., 1987). The scale has also been used in African American samples, with alpha reliability of .88 (Li et al., 2012). In the present study, alpha reliability was .84.
Physical Activity and BMI Measures
Actical accelerometer
Objective assessments of PA over 7 consecutive days were collected using Actical accelerometer devices (Mini-Mitter, Bend, OR). Actical accelerometers are small electronic devices that measure intensity and frequency of movement (i.e., PA) by detecting accelerations within spatial planes. Acticals detect movement omnidirectionally and provide a more sensitive accelerometry measure of PA when compared to accelerometers that detect motion on uni- or bidirectional planes (Esliger & Tremblay, 2006). Acticals have test–retest reliability coefficients for MVPA ranging from .85–.90 (Kayes et al., 2009). Participants wore an accelerometer on their right hip at all times for 1 week, with the exception of occasions when the device could get wet. Activity was categorized as MVPA if counts per minute were greater than or equal to 1,075, based on data from a calibration study conducted within a sample matched to the PATH sample (Trumpeter et al., 2012). MVPA was quantified as minutes per day. Given the challenges of collecting 7-day accelerometry data in low-resource communities, a compliance criterion of one or more 4-hr intervals was implemented and combined with full information maximum likelihood estimation (FIML), a robust technique for addressing missing data (Enders & Bandalos, 2001).
Four-Week Physical Activity History questionnaire
The Four-Week Physical Activity History questionnaire (FWH) was used as a measure of PA in secondary analyses to supplement accelerometry estimates of PA included in primary analyses. This measure was selected because it assesses PA for a longer period of time (i.e., 4 weeks) than is assessed by accelerometry in the present study. Further, the FWH provides information about participants’ self-reported frequency and duration of engagement in specific types of activities, including walking and exercise, over the previous 4 weeks. Thus, the supplemental PA data from the FWH permits a more complete examination of how PA may serve as a pathway linking environmental and social factors with BMI in underserved communities. Items on the walking subscale assessed activities such as walking for pleasure, to work, and up steps when an elevator was present. Items on the exercise subscale assessed participants’ conditioning exercises (e.g., jogging, running, weight lifting). Test–retest reliability is high (r = .60, p < .05; Ainsworth, Leon, Richardson, Jacobs, & Paffenbarger, 1993). Correlations for moderate intensity activities have been consistent with reliability studies of other PA questionnaires (Pereira et al., 1997).
Body mass index
BMI was calculated using height measured with a ShorrBoard and weight measured with a Seca 880 scale. Height and weight were measured twice to 0.1 cm and 0.5 kg, respectively, by certified staff. Weight (in kilograms) was divided by height (in square meters) to obtain BMI estimates, based on standard procedures (Flegal et al., 2012).
Data Analytic Plan
Direct and indirect effects of environmental and social factors were tested within a mediation framework using multiple linear regression. Accelerometry-estimated MVPA and self-reported PA data were positively skewed and log-transformed to obtain normal distributions. Both transformed and untransformed PA data were tested in the models, with similar results; therefore, untransformed data were included in the final models, given the benefits of retaining original metrics. Models were also tested with outliers and influential cases. These cases did not affect results and were included in final analyses. Variables that were not of theoretical interest but that demonstrated large correlations (r > .37) (Cohen, 1988) with the predictors, mediator, and/or outcome were entered as control variables. Data were clustered within three cities; however, implementation of a multilevel model was not feasible with a small cluster-level sample size of 3 and given that simulations have shown that a cluster-level sample size of 50 –100 is required for sufficient accuracy of multilevel model estimators (Hox, Maas, & Brinkhuis, 2010). Thus, community was a covariate in each model, as were age, sex, and education.
The product of coefficients method was applied using Mplus, Version 5.2 (Muthén & Muthén, Los Angeles, LA) and SAS, Version 9.2 (SAS Institute, Cary, NC) statistical software packages, and percentile bootstrapping was applied to adjust asymmetric confidence limits and biased standard errors (Fairchild, Mackinnon, Taborga, & Taylor, 2009; MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002). This approach supports the use of mediation in models for which there may not be strong predictor–outcome associations and provides a balance of power and Type I error (Fairchild & MacKinnon, 2009; Fairchild et al., 2009; MacKinnon, Fairchild, & Fritz, 2007; MacKinnon et al., 2002; MacKinnon & Luecken, 2008), which traditional mediation methods lack. The ratio of the mediated effect to the direct effect was calculated to indicate the size of the mediated effects of PA relative to the direct effect of environmental supports for PA on BMI (MacKinnon & Luecken, 2008). An additional measure calculated for the mediated effect was the proportion of the total effect that was mediated, or the product of a and b coefficients divided by the total effect of the model on BMI. Missing data were addressed using FIML estimation, resulting in more accurate Type I error rates than listwise or pairwise deletion and in a similar response pattern as multiple imputation (Enders & Bandalos, 2001). Less than 12% of data were missing for any given variable.
Results
Sample Characteristics
Demographic data are presented in Table 1. The sample represented both men (37%) and women (63%), with a mean age of 51 years (SD = 16). Participants were, on average, obese (MBMI = 30.88 kg/m2, SD = 8.43). Approximately half of the sample obtained no more than a high school diploma, and a majority reported making less than $24,000 (U.S. dollars) annually. Complete demographic and baseline characteristics of the sample are described in detail elsewhere (Wilson et al., 2010).
Table 1.
Sample Characteristics by Community and Total
| Characteristics | Community A | Community B | Community C | Total |
|---|---|---|---|---|
| Total | 133 (30) | 164 (38) | 137 (32) | 434 (100) |
| Sex | ||||
| Male | 44 (33) | 57 (35) | 61 (44) | 162 (37) |
| Female | 89 (67) | 107 (65) | 76 (56) | 272 (63) |
| Age (years)a | ||||
| Mean | 54.18 (15.58) | 48.14 (15.64) | 51.85 (15.39) | 51.19 (15.68) |
| 18–24 | 8 (6) | 15 (9) | 10 (7) | 33 (8) |
| 25–44 | 22 (17) | 52 (32) | 28 (20) | 102 (24) |
| 45–64 | 67 (50) | 70 (42) | 70 (51) | 207 (48) |
| 65+ | 36 (27) | 27 (17) | 29 (21) | 92 (21) |
| Employmenta | ||||
| Working | 38 (29) | 71 (43) | 60 (44) | 169 (39) |
| Unemployed | 29 (22) | 32 (20) | 24 (18) | 85 (20) |
| Retired | 39 (29) | 26 (16) | 29 (21) | 94 (22) |
| Disabled | 7 (5) | 19 (12) | 9 (7) | 36 (8) |
| Other | 19 (14) | 16 (10) | 14 (10) | 49 (11) |
| No response | 1 (.5) | 0 (0) | 1 (.5) | 2 (1) |
| Marital Status | ||||
| Married | 36 (27) | 32 (20) | 32 (23) | 100 (23) |
| Separated | 18 (14) | 20 (12) | 21 (15) | 59 (14) |
| Divorced | 16 (12) | 18 (11) | 15 (11) | 49 (11) |
| Widowed | 30 (23) | 27 (17) | 24 (18) | 81 (19) |
| Never married | 23 (17) | 54 (33) | 34 (25) | 111 (26) |
| Unmarried couple | 9 (7) | 13 (8) | 9 (7) | 31 (7) |
| No response | 1 (1) | 0 (0) | 2 (1) | 3 (1) |
| Education | ||||
| Less than high school degree | 36 (27) | 43 (26) | 39 (29) | 118 (27) |
| High school degree/GED | 49 (37) | 76 (46) | 49 (36) | 174 (40) |
| More than high school degree | 45 (34) | 43 (26) | 44 (32) | 132 (30) |
| No response | 3 (2) | 2 (1) | 5 (4) | 10 (2) |
| Income | ||||
| <$10,000 | 42 (32) | 42 (26) | 41 (30) | 125 (29) |
| $10,000–24,000 | 43 (32) | 61 (37) | 41 (30) | 145 (33) |
| $25,000–39,000 | 24 (18) | 24 (15) | 29 (21) | 77 (18) |
| >$40,000 | 20 (15) | 27 (17) | 16 (12) | 63 (15) |
| No response | 4 (3) | 10 (6) | 10 (7) | 24 (6) |
Note. Demographics reported as number (percentage); age reported as mean (standard deviation). GED = General Educational Development.
Significant differences (p < .05) between community demographics were found for age and employment status.
Descriptive data for the predictors, mediators, and outcomes of substantive interest in the present study are presented in Table 2. Mean scores for social and environmental measures typically fell within the mid range of the 4- or 5-point response scales. Based on accelerometry assessment, participants generally engaged in 22 min of daily MVPA (SD = 28.79), although the distribution of MVPA was skewed and the median was 13 min. Participants reported engaging in an average of 37 min of walking and 19 min of exercise daily. Self-reported walking and exercise differed significantly by community (p ≤ .01), with Community B differing from both the full intervention and the general health communities on each of those measures.
Table 2.
Descriptive Statistics With Means (Standard Deviations) by Community and Total for Model Variables (n = 403)
| Measure | Community
|
Total | ||
|---|---|---|---|---|
| A | B | C | ||
| Infrastructure for walking | 2.54 (0.71) | 2.59 (0.65) | 2.55 (0.77) | 2.56 (0.71) |
| Access to services* | 3.04 (0.88)c | 3.22 (0.73)c | 2.83 (0.79)d | 3.04 (0.81) |
| Crime* | 2.69 (0.87)c | 2.76 (0.77)c | 2.12 (0.89)d | 2.54 (0.89) |
| Social Support | 2.35 (0.96) | 2.52 (1.03) | 2.61 (1.06) | 2.50 (1.03) |
| MVPA/daya | 19.67 (30.36) | 23.01 (31.77) | 19.73 (22.58) | 22.06 (28.79) |
| Walking/dayb* | 32.94 (41.41)c | 28.37 (57.13)d | 49.02 (71.55)c | 36.96 (58.25) |
| Exercise/dayb* | 18.17 (29.88)c | 15.81 (27.30)d | 20.19 (38.90)c | 19.03 (32.38) |
| BMI | 31.05 (7.93) | 30.26 (8.34) | 31.40 (9.03) | 30.88 (8.43) |
Note. MVPA = moderate-to-vigorous physical activity; BMI = body mass index.
Assessed by accelerometry.
Self-reported.
Denotes significant differences by community at p ≤ .01, with shared superscripts (c, d) indicating no significant differences at p ≤ .01 by a Bonferroni test.
Correlation Analyses
Correlations were significant and in the expected directions for the association of infrastructure for walking (r = .24, p < .01) and access to services (r = .22, p < .01) with MVPA. Infrastructure for walking also correlated with self-reported walking (r = .15, p < .01). Both MVPA (r = −.31, p < .01) and self-reported walking (r = −.14, p < .01) correlated with BMI. Control variables were consistently significantly associated with the variables of primary interest, with higher MVPA associated with younger age (r = −.34, p < .01) and being male (r = −.39, p < .01), and higher BMI associated with being female (r = −.32, p < .01).
Mediation Analyses
Separate mediation models tested each of the three PA variables as a mediator of associations between environmental and social supports for PA and BMI. Initial models included covariates (i.e., age, sex, education, and community), infrastructure for walking, access to services, crime, peer social support, BMI, and the relevant measure of PA. However, because neither crime nor peer social support was significantly associated with target study variables, they were excluded from the final models reported in the results.
Predictors in the primary model, which included accelerometry-assessed MVPA as mediator, collectively accounted for 15% of the total variance in the BMI outcome and 27% of the total variance in the MVPA mediator. The secondary models, which included self-reported PA as mediators, accounted for 14 and 12% of the total variance in the BMI outcome and 4 and 3% of the total variance in the self-reported walking and exercise mediators, respectively.
Direct Effects
Primary model with accelerometry-assessed MVPA
Demographic variables were significantly associated with BMI and MVPA. Specifically, sex was significantly associated with BMI (B = 4.25, SE = 0.89, p < .001) and with MVPA (B = −19.51, SE = 3.26, p < .001). Compared to men, women had a greater BMI and fewer minutes of daily MVPA. Age was also significantly associated with MVPA (B = −0.46, SE = 0.08, p < .001) such that, with increasing age, participants engaged in fewer minutes of daily MVPA. No other demographic variables in the model were significantly associated with either BMI or MVPA. Infrastructure for walking predicted MVPA (B = 4.06, SE = 1.58, p = .01), indicating that for every 1-unit increase in this feature of the neighborhood environment, daily MVPA increased by approximately 4 min (see Figure 1). Although access to services was positively related to MVPA, this association was not statistically significant (B = 2.27, SE = 1.22, p = .06). This model further revealed that MVPA was significantly associated with BMI (B = 0.07, SE = 0.02, p < .001). Neither infrastructure for walking (B = −0.09, SE = 0.42, p = .82) nor access to services (B = 0.05, SE = 0.39, p = .91) directly predicted BMI.
Figure 1.
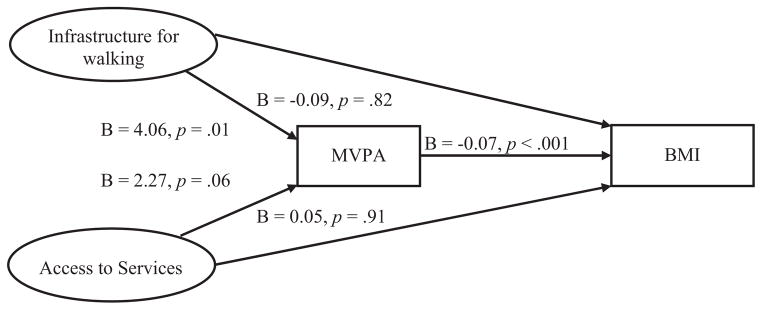
Results of primary model for testing direct relations. MVPA = moderate-to-vigorous physical activity; BMI = body mass index.
Secondary model with self-reported walking
This model revealed a significant association between infrastructure for walking and self-reported walking (B = 7.39, SE = 3.42, p = .03), indicating that for every 1-unit increase in this feature of the neighborhood environment, daily walking increased by approximately 7 min. Access to services was not significantly associated with self-reported walking (B = 1.75, SE = 2.84, p = .54). Self-reported walking was significantly associated with BMI (B = −0.02, SE = 0.01, p = .01). Neither infrastructure for walking (B = −0.16, SE = 0.44, p = .72) nor access to services (B = −0.06, SE = 0.39, p = .89) directly predicted BMI.
Secondary model with self-reported exercise
Neither infrastructure for walking (B = 1.31, SE = 2.04, p = .52) nor access to services (B = −0.20, SE = 1.74, p = .91) was associated with self-reported exercise. Self-reported exercise was not significantly associated with BMI (B = 0.00, SE = 0.01, p = .97), and neither infrastructure for walking (B = −0.30, SE = 0.43, p = .49) nor access to services (B = −0.09, SE = 0.39, p = .81) was significantly associated with BMI.
Indirect Effects
The primary model revealed that accelerometry-assessed MVPA was a significant mediator linking infrastructure for walking and BMI (B = −0.03, SE = 0.02, p = .04). A ratio of the mediated effect to the total effect (i.e., the amount of variance in BMI accounted for through the mediated effect vs. the independent effect of infrastructure for walking on BMI) indicated that the mediated effect of MVPA on BMI was 2.85 times larger than the direct effect of infrastructure for walking on BMI. The proportion of the absolute total effect that was mediated by MVPA indicated that 74% of the relation or shared variance of infrastructure for walking and BMI was attributable to the presence of MVPA. Secondary models revealed no statistically significant mediation effects for either self-reported walking or exercise.
Discussion
This study examined PA as a potential mediator of associations between features of the neighborhood environment and peer social support with BMI in African American men and women residing in underserved communities. Tests of indirect relations indicated that accelerometry-assessed MVPA mediated the association of infrastructure for walking (e.g., sidewalks, trails), but not access to services, and BMI. Direct effects of infrastructure for walking on MVPA and self-reported walking were observed. Access to services was also associated with MVPA; however, that association was only marginally significant. Further, self-reported walking and MVPA were significantly associated with BMI. These effects demonstrate the importance of neighborhood supports for PA, particularly infrastructure for walking, in influencing MVPA and BMI in low-income African American adults.
Findings in the present study expand on a growing literature that has suggested neighborhood walkability is a consistent predictor of walking and PA (Ainsworth et al., 2003; Kaczynski & Glover, 2012; Owen et al., 2004; Sallis et al., 2009; Wendel-Vos, Droomers, Kremers, Brug, & van Lenthe, 2007). These findings contribute to a limited number of studies that have examined this association in African American men and women (Ainsworth et al., 2003; Rohm Young & Voorhees, 2003; Sanderson et al., 2003). The present study further contributes to the literature by examining different measures of PA to better understand how PA may link the neighborhood environment and BMI in underserved African American communities. In this study, accelerometry-assessed MVPA, but not self-reported PA, mediated the effect of the neighborhood environment on BMI. Previous research, however, has found the relation of neighborhood walkability and BMI to be mediated by both accelerometry-assessed MVPA and self-reported walking for recreation and transportation in Belgian adults (Van Dyck et al., 2010). The present findings highlight the importance of examining PA at different levels of intensity and using both objective and self-report measures to better understand the specific types of PA that characterize potential pathways through which environmental factors influence obesity.
Although the present study found that infrastructure for walking was associated with PA and BMI in underserved African American adults, neither neighborhood crime nor social support was significantly associated with any of the measures of PA or BMI. The absence of a significant effect of crime may indicate that the perception of neighborhood crime may not influence PA, unless it is accompanied by an emotional reaction. That is, neighborhood crime may only impact PA if it is viewed as a threat to the individual during PA engagement that occurs within that context. Additionally, some individuals residing in underserved communities may habituate to the presence of crime, such that it does not largely impact their daily lives or PA activities.
The absence of a significant association between social support and PA in the present study contrasts with some previous investigations (Orsega-Smith, Payne, Mowen, Ho, & Godbey, 2007; Peterson & Cheng, 2011; Sharma et al., 2005). Social support may serve as an important motivating factor and resource for influencing attitudes about PA (Fleury & Lee, 2006). However, African Americans in underserved communities may benefit more from tangible types of support, which were not specifically measured in this study. For example, adults might benefit from supports that would reduce time constraints imposed by social roles, such as assistance with caregiving responsibilities. Consistent with this hypothesis, one study found that having fewer social roles (e.g., household tasks, childcare responsibilities) was associated with being more likely to meet PA recommendations in African American women (Rohm Young & Voorhees, 2003). Another study showed that having practical or tangible social support from a close significant other predicted engaging in and maintaining an active lifestyle (Kouvonen et al., 2012). Future research should examine the association of tangible supports that reduce burdens, such as those imposed by social roles, with PA in African American adults.
Overall, this study demonstrated that neighborhood walkability is indirectly related to obesity through PA in African American adults residing in low-income communities. Neighborhood infrastructure for walking may be especially important in underserved groups for whom other PA resources (e.g., exercise facilities) may be limited. There was also some evidence in this study that having access to services within walking distance may be associated with PA. Together, these findings may suggest that tangible supports for PA are especially important in underserved African American adults because they confer opportunities to engage in PA that are not afforded by other forms of support, such as encouragement to be active.
Study Limitations
There were several limitations to the current study. Given the cross-sectional design, our results do not provide strong support for potential causal pathways that were hypothesized to affect BMI in low-income African American adults. Although there are reasons to believe that environmental and social factors affect PA, which would in turn affect BMI, it is possible that the associations found in the present study are bidirectional. That is, characteristics of the individual may influence the types of environments adults select for their residence, and neighborhood PA may affect the physical environments of the neighborhood. Thus, the potential causal pathways examined and theorized to influence obesity in low-income African American adults should be the focus of future investigations. Specifically, further studies should examine the relations investigated in this study using longitudinal and experimental approaches.
Conclusion
The present study contributes to an understanding of MVPA as a potential mediator linking neighborhood walkability and BMI in African American adults. Although neighborhood infrastructure for walking accounted for a relatively small amount of variance in the present study, its contribution has the potential to impact public health at the community level. These findings may aid in the development of effective programs that aim to address health disparities because they imply that the presence of tangible supports for PA that afford opportunities for being active, such as neighborhood infrastructure for walking, may contribute to PA and help to reduce obesity in African American adults residing in underserved communities.
Acknowledgments
This research was supported by grants funded by National Institutes of Diabetes and Digestive and Kidney Diseases (R01 DK067615) and of Child Health and Human Development (HD 072153) to Dawn K. Wilson, PhD, and in part by training grants from the National Institute on Aging (F31 AG039930) and of General Medical Sciences (T32 GM081740) to Sandra M. Coulon, M.A.
References
- Adams MA, Ryan S, Kerr J, Sallis JF, Patrick K, Frank LD, Norman GJ. Validation of the Neighborhood Environment Walkability Scale (NEWS) items using geographic information systems. Journal of Physical Activity & Health. 2009;6(Supp 1):S113–S123. doi: 10.1123/jpah.6.s1.s113. [DOI] [PubMed] [Google Scholar]
- Addy CL, Wilson DK, Kirtland KA, Ainsworth BE, Sharpe P, Kimsey D. Associations of perceived social and physical environmental supports with physical activity and walking behavior. American Journal of Public Health. 2004;94:440–443. doi: 10.2105/AJPH.94.3.440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ainsworth BE, Leon AS, Richardson MT, Jacobs DR, Paffenbarger RS. Accuracy of the college alumnus physical activity questionnaire. Journal of Clinical Epidemiology. 1993;46:1403–1411. doi: 10.1016/0895-4356(93)90140-V. [DOI] [PubMed] [Google Scholar]
- Ainsworth BE, Wilcox S, Thompson WW, Richter DL, Henderson KA. Personal, social, and physical environmental correlates of physical activity in African-American women in South Carolina. American Journal of Preventive Medicine. 2003;25(3 Supp 1):23–29. doi: 10.1016/S0749-3797(03)00161-2. [DOI] [PubMed] [Google Scholar]
- Bennett GG, McNeill LH, Wolin KY, Duncan DT, Puleo E, Emmons KM. Safe to walk? Neighborhood safety and physical activity among public housing residents. PLoS Medicine. 2007;4:1599–1606. doi: 10.1371/journal.pmed.0040306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bopp M, Wilcox S, Laken M, Butler K, Carter RE, McClorin L, Yancey A. Factors associated with physical activity among African-American men and women. American Journal of Preventive Medicine. 2006;30:340–346. doi: 10.1016/j.amepre.2005.11.007. [DOI] [PubMed] [Google Scholar]
- Brock DW, Thomas O, Cowan CD, Allison DB, Gaesser GA, Hunter GR. Association between insufficiently physically active and the prevalence of obesity in the United States. Journal of Physical Activity & Health. 2009;6:1–5. doi: 10.1123/jpah.6.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bronfenbrenner U. The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press; 1979. [Google Scholar]
- Bronfenbrenner U, Ceci SJ. Nature-nurture reconceptualized in developmental perspective: A bioecological model. Psychological Review. 1994;101:568–586. doi: 10.1037/0033-295X.101.4.568. [DOI] [PubMed] [Google Scholar]
- Casagrande SS, Whitt-Glover MC, Lancaster KJ, Odoms-Young AM, Gary TL. Built environment and health behaviors among African Americans: A systematic review. American Journal of Preventive Medicine. 2009;36:174–181. doi: 10.1016/j.amepre.2008.09.037. [DOI] [PubMed] [Google Scholar]
- Cerin E, Conway TL, Saelens BE, Frank LD, Sallis JF. Cross-validation of the factorial structure of the Neighborhood Environment Walkability Scale (NEWS) and its abbreviated form (NEWS-A) The International Journal of Behavioral Nutrition and Physical Activity. 2009;6:32. doi: 10.1186/1479-5868-6-32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cerin E, Saelens BE, Sallis JF, Frank LD. Neighborhood Environment Walkability Scale: Validity and development of a short form. Medicine and Science in Sports and Exercise. 2006;38:1682–1691. doi: 10.1249/01.mss.0000227639.83607.4d. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2. Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- Coulon SM, Wilson DK, Griffin S, StGeorge SM, Alia KA, Trumpeter NN, Gadson B. Formative process evaluation for implementing a social marketing intervention to increase walking in African Americans in the Positive Action for Today’s Health trial. American Journal of Public Health. 2012;102:2315–2321. doi: 10.2105/AJPH.2012.300758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK, Bandalos DL. The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling. 2001;8:430–457. doi: 10.1207/S15328007SEM0803_5. [DOI] [Google Scholar]
- Esliger DW, Tremblay MS. Technical reliability assessment of three accelerometer models in a mechanical setup. Medicine & Science in Sports & Exercise. 2006;38:2173–2181. doi: 10.1249/01.mss.0000239394.55461.08. [DOI] [PubMed] [Google Scholar]
- Eyler AA, Baker E, Cromer LC, King AC, Brownson RC, Donatelle RJ. Physical activity and minority women: A qualitative study. Health Education & Behavior. 1998;25:640–652. doi: 10.1177/109019819802500510. [DOI] [PubMed] [Google Scholar]
- Eyler AA, Brownson RC, Donatelle RJ, King AC, Brown D, Sallis JF. Physical activity social support and middle-and older-aged minority women: Results from a US survey. Social Science and Medicine. 1999;49:781–789. doi: 10.1016/S0277-9536(99)00137-9. [DOI] [PubMed] [Google Scholar]
- Eyler AA, Matson-Koffman D, Young DR, Wilcox S, Wilbur J, Thompson JL, Evenson KR. Quantitative study of correlates of physical activity in women from diverse racial/ethnic groups: The Women’s Cardiovascular Health Network Project summary and conclusions. American Journal of Preventive Medicine. 2003;25(3 Supp 1):93–103. doi: 10.1016/s0749-3797(03)00170-3. [DOI] [PubMed] [Google Scholar]
- Fairchild AJ, MacKinnon DP. A general model for testing mediation and moderation effects. Prevention Science. 2009;10:87–99. doi: 10.1007/s11121-008-0109-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fairchild AJ, Mackinnon DP, Taborga MP, Taylor AB. R2 effect-size measures for mediation analysis. Behavior Research Methods. 2009;41:486–498. doi: 10.3758/BRM.41.2.486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flegal KM, Carroll MD, Kit BK, Ogden CL. Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999 –2010. JAMA: Journal of the American Medical Association. 2012;307:491–497. doi: 10.1001/jama.2012.39. [DOI] [PubMed] [Google Scholar]
- Fleury J, Lee SM. The social ecological model and physical activity in African American women. American Journal of Community Psychology. 2006;37:129–140. doi: 10.1007/s10464-005-9002-7. [DOI] [PubMed] [Google Scholar]
- Foster S, Giles-Corti B. The built environment, neighborhood crime and constrained physical activity: An exploration of inconsistent findings. Preventive Medicine: An International Journal Devoted to Practice and Theory. 2008;47:241–251. doi: 10.1016/j.ypmed.2008.03.017. [DOI] [PubMed] [Google Scholar]
- Gordon-Larsen P, Nelson MC, Page P, Popkin BM. Inequality in the built environment underlies key health disparities in physical activity and obesity. Pediatrics. 2006;117:417–424. doi: 10.1542/peds.2005-0058. [DOI] [PubMed] [Google Scholar]
- Hannon L, Sawyer P, Allman RM. The influence of community and the built environment on physical activity. Journal of Aging and Health. 2012;24:384–406. doi: 10.1177/0898264311424430. [DOI] [PubMed] [Google Scholar]
- Harley AE, Katz ML, Heaney CA, Duncan DT, Buckworth J, Odoms-Young A, Willis SK. Social support and companionship among active African American women. American Journal of Health Behavior. 2009;33:673–685. doi: 10.5993/AJHB.33.6.5. [DOI] [PubMed] [Google Scholar]
- Heinrich KM, Lee RE, Suminski RR, Regan GR, Reese-Smith JY, Howard HH, Ahluwalia JS. Associations between the built environment and physical activity in public housing residents. International Journal of Behavioral Nutrition and Physical Activity. 2007;4:56. doi: 10.1186/1479-5868-4-56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holman C, Donovan RJ, Corti B. Factors influencing the use of physical activity facilities: Results from qualitative research. Health Promotion Journal of Australia. 1996;6:16–21. [Google Scholar]
- Hooker SP, Harmon B, Burroughs EL, Rheaume CE, Wilcox S. Exploring the feasibility of a physical activity intervention for midlife African American men. Health Education Research. 2011;26:732–738. doi: 10.1093/her/cyr034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hooker SP, Wilson DK, Griffin SF, Ainsworth BE. Perceptions of environmental supports for physical activity in African American and white adults in a rural county in South Carolina. Preventing Chronic Disease. 2005;2:1–10. [PMC free article] [PubMed] [Google Scholar]
- Hox JJ, Maas CJM, Brinkhuis MJS. The effect of estimation method and sample size in multilevel structural equation modeling. Statistica Neerlandica. 2010;64:157–170. doi: 10.1111/j.1467-9574.2009.00445.x. [DOI] [Google Scholar]
- Kaczynski AT, Glover TD. Talking the talk, walking the walk: Examining the effect of neighbourhood walkability and social connectedness on physical activity. Journal of Public Health. 2012;34:382–389. doi: 10.1093/pubmed/fds011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kayes NM, Schluter PJ, McPherson KM, Leete M, Mawston G, Taylor D. Exploring actical accelerometers as an objective measure of physical activity in people with multiple sclerosis. Archives of Physical Medicine and Rehabilitation. 2009;90:594–601. doi: 10.1016/j.apmr.2008.10.012. [DOI] [PubMed] [Google Scholar]
- King AC, Castro C, Wilcox S, Eyler AA, Sallis JF, Brownson RC. Personal and environmental factors associated with physical inactivity among different racial-ethnic groups of U.S. middle-aged and older-aged women. Health Psychology. 2000;19:354–364. doi: 10.1037/0278-6133.19.4.354. [DOI] [PubMed] [Google Scholar]
- King WC, Belle SH, Brach JS, Simkin-Silverman LR, Soska T, Kriska AM. Objective measures of neighborhood environment and physical activity in older women. American Journal of Preventive Medicine. 2005;28:461. doi: 10.1016/j.amepre.2005.02.001. [DOI] [PubMed] [Google Scholar]
- Komar-Samardzija M, Braun LT, Keithley JK, Quinn LT. Factors associated with physical activity levels in African-American women with type 2 diabetes. Journal of the American Academy of Nurse Practitioners. 2012;24:209–217. doi: 10.1111/j.1745-7599.2011.00674.x. [DOI] [PubMed] [Google Scholar]
- Kouvonen A, De Vogli R, Stafford M, Shipley MJ, Marmot MG, Cox T, Kivimäki M. Social support and the likelihood of maintaining and improving levels of physical activity: The Whitehall II Study. The European Journal of Public Health. 2012;22:514–518. doi: 10.1093/eurpub/ckr091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li K, Seo DC, Torabi MR, Peng CYJ, Kay NS, Kolbe LJ. Social-ecological factors of leisure-time physical activity in Black adults. American Journal of Health Behavior. 2012;36:797–810. doi: 10.5993/AJHB.36.6.7. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP, Fairchild AJ, Fritz MS. Mediation analysis. Annual Review of Psychology. 2007;58:593–614. doi: 10.1146/annurev.psych.58.110405.085542. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7:83–104. doi: 10.1037/1082-989X.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Luecken LJ. How and for whom? Mediation and moderation in health psychology. Health Psychology. 2008;27(2 Supp):S99–S100. doi: 10.1037/0278-6133.27.2(Suppl).S99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Education Quarterly. 1988;15:351–377. doi: 10.1177/109019818801500401. [DOI] [PubMed] [Google Scholar]
- Orsega-Smith EM, Payne LL, Mowen AJ, Ho C, Godbey GC. The role of social support and self-efficacy in shaping the leisure time physical activity of older adults. Journal of Leisure Research. 2007;39:70, 5–727. [Google Scholar]
- Owen N, Humpel N, Leslie E, Bauman A, Sallis JF. Understanding environmental influences on walking: Review and research agenda. American Journal of Preventive Medicine. 2004;27:67–76. doi: 10.1016/j.amepre.2004.03.006. [DOI] [PubMed] [Google Scholar]
- Parks SE, Housemann RA, Brownson RC. Differential correlates of physical activity in urban and rural adults of various socioeconomic backgrounds in the United States. Journal of Epidemiology and Community Health. 2003;57:29–35. doi: 10.1136/jech.57.1.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pereira MA, FitzerGerald SJ, Gregg EW, Joswiak ML, Ryan WJ, Suminski RR, Zmuda JM. A collection of Physical Activity Questionnaires for health-related research. Medicine and Science in Sports and Exercise. 1997;29(6 Supp):S1–S205. [PubMed] [Google Scholar]
- Peterson JA, Cheng AL. Heart and soul physical activity program for African American women. Western Journal of Nursing Research. 2011;33:652–670. doi: 10.1177/0193945910383706. [DOI] [PubMed] [Google Scholar]
- Poortinga W. Do health behaviors mediate the association between social capital and health? Preventive Medicine: An International Journal Devoted to Practice and Theory. 2006a;43:488–493. doi: 10.1016/j.ypmed.2006.06.004. [DOI] [PubMed] [Google Scholar]
- Poortinga W. Perceptions of the environment, physical activity, and obesity. Social Science & Medicine. 2006b;63:2835–2846. doi: 10.1016/j.socscimed.2006.07.018. [DOI] [PubMed] [Google Scholar]
- Prus SG. Age, SES, and health: A population level analysis of health inequalities over the lifecourse. Sociology of Health & Illness. 2007;29:275–296. doi: 10.1111/j.1467-9566.2007.00547.x. [DOI] [PubMed] [Google Scholar]
- Rohm Young D, Voorhees CC. Personal, social, and environmental correlates of physical activity in urban African-American women. American Journal of Preventive Medicine. 2003;25(3 Supp 1):38–44. doi: 10.1016/S0749-3797(03)00163-6. [DOI] [PubMed] [Google Scholar]
- Saelens BE, Sallis JF, Black JB, Chen D. Neighborhood-based differences in physical activity: An environment scale evaluation. American Journal of Public Health. 2003;93:1552–1558. doi: 10.2105/AJPH.93.9.1552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sallis JF, Bowles HR, Bauman A, Ainsworth BE, Bull FC, Craig CL, Bergman P. Neighborhood environments and physical activity among adults in 11 countries. American Journal of Preventive Medicine. 2009;36:484–490. doi: 10.1016/j.amepre.2009.01.031. [DOI] [PubMed] [Google Scholar]
- Sallis JF, Grossman RM, Pinski RB, Patterson TL, Nader PR. The development of scales to measure social support for diet and exercise behaviors. Preventive Medicine: An International Journal Devoted to Practice and Theory. 1987;16:825–836. doi: 10.1016/0091-7435(87)90022-3. [DOI] [PubMed] [Google Scholar]
- Sanderson BK, Foushee HR, Bittner V, Cornell CE, Stalker V, Shelton S, Pulley L. Personal, social, and physical environmental correlates of physical activity in rural African-American women in Alabama. American Journal of Preventive Medicine. 2003;25(3 Supp 1):30–37. doi: 10.1016/S0749-3797(03)00162-4. [DOI] [PubMed] [Google Scholar]
- Sharma M, Sargent L, Stacy R. Predictors of leisure-time physical activity among African American women. American Journal of Health Behavior. 2005;29:352–359. doi: 10.5993/AJHB.29.4.7. [DOI] [PubMed] [Google Scholar]
- Spence JC, Lee RE. Toward a comprehensive model of physical activity. Psychology of Sport and Exercise. 2003;4:7–24. doi: 10.1016/S1469-0292(02)00014-6. [DOI] [Google Scholar]
- Thomas S, Reading J, Shephard RJ. Revision of the Physical Activity Readiness Questionnaire (PAR-Q) Canadian Journal of Sport Sciences. 1992;17:338–345. [PubMed] [Google Scholar]
- Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Medicine and Science in Sports and Exercise. 2008;40:181–188. doi: 10.1249/mss.0b013e31815a51b3. [DOI] [PubMed] [Google Scholar]
- Trost SG, Owen N, Bauman AE, Sallis JF, Brown W. Correlates of adults’ participation in physical activity: Review and update. Medicine and Science in Sports and Exercise. 2002;34:1996–2001. doi: 10.1097/00005768-200212000-00020. [DOI] [PubMed] [Google Scholar]
- Trumpeter NN, Lawman HG, Wilson DK, Pate RR, Van Horn ML, Tate AK. Accelerometry cut points for physical activity in underserved African Americans. The International Journal of Behavioral Nutrition and Physical Activity. 2012;9:73. doi: 10.1186/1479-5868-9-73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Dyck D, Cerin E, Cardon G, Deforche B, Sallis JF, Owen N, de Bourdeaudhuij I. Physical activity as a mediator of the associations between neighborhood walkability and adiposity in Belgian adults. Health & Place. 2010;16:952–960. doi: 10.1016/j.healthplace.2010.05.011. [DOI] [PubMed] [Google Scholar]
- Wendel-Vos W, Droomers M, Kremers S, Brug J, van Lenthe F. Potential environmental determinants of physical activity in adults: A systematic review. Obesity Reviews. 2007;8:425–440. doi: 10.1111/j.1467-789X.2007.00370.x. [DOI] [PubMed] [Google Scholar]
- Wilbur J, Chandler PJ, Dancy B, Lee H. Correlates of physical activity in urban Midwestern African-American women. American Journal of Preventive Medicine. 2003;25(3 Supp 1):45–52. doi: 10.1016/S0749-3797(03)00164-8. [DOI] [PubMed] [Google Scholar]
- Wilson DK, Trumpeter NN, St George SM, Coulon SM, Griffin S, Lee Van Horn M, Gadson B. An overview of the “Positive Action for Today’s Health” (PATH) trial for increasing walking in low income, ethnic minority communities. Contemporary Clinical Trials. 2010;31:624–633. doi: 10.1016/j.cct.2010.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]