

Abstract
Dentigerous cyst is a developmental odontogenic cyst, which develops by accumulation of fluid between reduced enamel epithelium and the tooth crown of an unerupted tooth. Dentigerous cysts are usually solitary, slow growing, asymptomatic lesions that are incidentally found during routine radiographs They most frequently involve the mandibular third molar followed in order of frequency by the maxillary canine, mandibular second pre-molar and maxillary third molar. Occasionally, these cysts become painful when infected causing swelling and erythema. The cyst is usually small, however, when large, results in the expansion and thinning of the cortex leading to pathological fracture. Radiographic features are specific to the lesion characterized by a well-defined radiolucency circumscribed by a sclerotic border, associated with the crown of an impacted or unerupted tooth. Dentigerous cysts are treated most commonly by enucleation, Marsupialization and decompression of cyst by fenestration. The criteria for selecting the treatment modality is based on the age, size, location, stage of root development, position of the involved tooth and relation of the lesion to the adjacent tooth and vital structure. The prognosis is an excellent when the cyst is enucleated and recurrence is rare. In this article, we present a case of a Dentigerous cyst in an 80-year-old man in the anterior aspect of the mandible enveloping an impacted canine and crossing the midline but with no clinical expansion or discomfort.
Keywords: Anterior mandible, crossing midline, dentigerous cyst
INTRODUCTION
The Dentigerous cyst is the most common type of noninflammatory odontogenic cyst and the most common cause of a pericoronal area of lucency associated with an impacted tooth.[1]
Dentigerous cyst was described by Paget in 1863.[1] The Dentigerous cyst develops around an unerupted tooth by accumulation of fluid between the reduced enamel epithelium and the enamel. It has been suggested that the pressure exerted by a potentially erupting tooth on an impacted follicle obstructs the venous outflow and there by induces rapid transudation of serum capillary walls. The increased hydrostatic pressure of this pooling fluid separates the follicle from the crown with or without reduced enamel epithelium.[2]
It may cause facial asymmetry if aggressive in nature.[1] Their association with supernumerary teeth was studied by Lustmann and Bodner in 1988.[3] Dentigerous cysts by far the most common lesion that often exhibits marked displacement of the unerupted tooth within the jaw. With the pressure of enlarging cyst, the unerupted tooth can be pushed away from its direction of eruption.[4]
Here, we present a rare case report of a Dentigerous cyst in an 80-year-old male in the anterior mandible crossing the midline. This rare case is reported because of its unusual presentation at such a location, its occurrence at this age and most importantly it is unique case because it is a single Dentigerous cyst crossing midline, which is not reported in any of the literature available.
CASE REPORT
An 80-year-old man, reported to the Department of Oral Medicine and Radiology with the chief complaint of pus discharge from the left lower front region of face since 2 years. Pus discharge was spontaneous, intermittent and started and stopped on its own. The pus discharge was not associated with any discomfort [Figure 1].
Figure 1.

Extra-oral view showing fibrosed sinus opening in the parasymphyseal region in the lower border of the mandible
On examination, extra-orally a fibrosed sinus opening was present on the left parasymphyseal region. The skin surrounding the sinus appeared normal in color with no secondary changes. On palpation, sinus opening was non-tender and fixed to the underlying bone with no frank discharge but a single, non-tender, movable left submandibular lymph node was palpable. Intra-orally generalized wasting disease of the teeth was present. Root stump in relation to 17, 21, 22, 27, 46 were present and 26, 34, 35, 43 were missing.
Radiographs
IOPA in relation to 35, 36, 37 revealed radiolucency in the periapical region of 36 not contacting the teeth.
Mandibular cross-sectional occlusal radiograph showed diffuse radiolucency extending from 34 to 44 region, latero-medially and from periapex to lower border of mandible superior-inferiorly. The cortical plates are not expanded [Figure 2].
Figure 2.

Mandibular cross-sectional radiograph revealing radiolucent area from 34 to 44 region latero-medially and from periapex to lower border of mandible superior-inferiorly
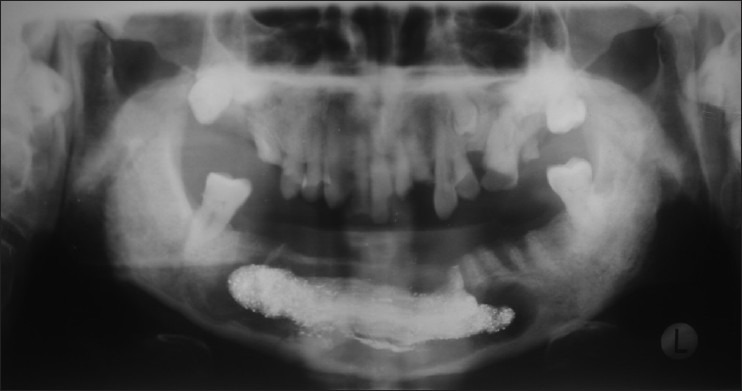
OPG showed a unilocular well-defined radiolucency extending lateromedially from the distal root of 36 to the mesial root of 47 and superior-inferiorly from the furcation area of the teeth to the lower border of the mandible. The periphery of the radiolucency is scalloped with sclerotic border. A well-defined radio-opacity is seen at the lower border of the mandible on the right side in the periapex of 44, which was identified as impacted canine (43) [Figure 3].
Figure 3.

OPG showing a unilocular well defined radiolucency with scalloped margins associated with impacted canine
On the basis of history, clinical and radiological examination, a provisional diagnosis of Odontogenic keratocyst was given.
Treatment
Enucleation of the cyst with chemical cauterization was done conserving the impacted canine to avoid fracture of lower border of the mandible. The teeth involved in the cystic lining were extracted. The surgery was done using local anesthesia and under antibiotic cover.
The cystic lining was sent for further histopathological examination. Histopathological examination revealed cystic epithelium comprising of 2-3 layers of non-keratinized stratified squamous epithelium. Fibrous connective tissue and slight inflammatory cell infiltrate was observed in connective tissue stroma. Hence, the diagnosis of Dentigerous cyst was confirmed [Figure 4].
Figure 4.
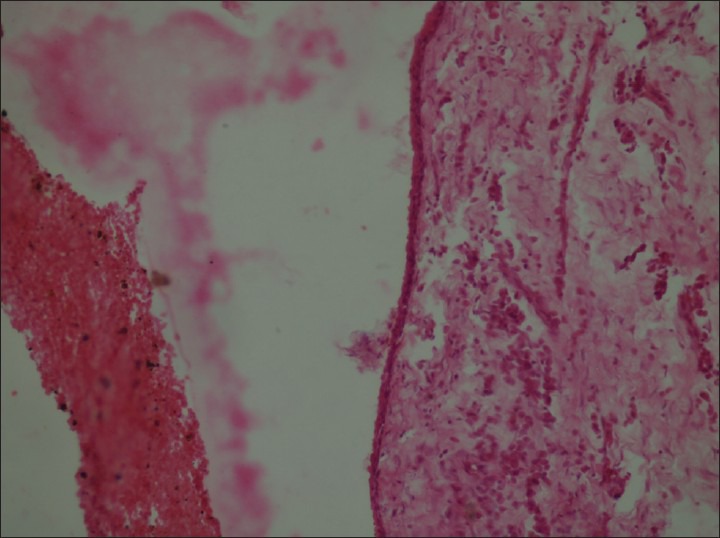
Photomicrograph revealed-3 layers of non-keratinized stratified squamous epithelium with fibrous connective tissue and inflammatory cell infiltrate
Healing was uneventful and 1 week after the surgery, the surgical site showed good healing and the sutures were removed. The patient was recalled for follow-up every week and Iodoform dressing was given. The post-operative OPG taken after 2 weeks revealed healing by secondary intention [Figure 5]. Patient was lost to follow-up.
Figure 5.
Post-op OPG revealing Iodoform dresssing and showing healing by secondary intention
DISCUSSION
Dentigerous cyst accounts for more than 24% of jaw cysts and it is the most common developmental cyst of oral region. The Dentigerous cyst occurs most commonly in second and third decade.[5] Koseoglu et al. in their study, stated that Dentigerous cysts occur over a wide age range age from 15 years to 65 years.[6] As evident from literature Dentigerous cyst is twice as often in males than females and is 10 times more likely to occur in the lower-jaw than in the upper-jaw. The present case seems to support the age and sex pre-dilection given by other authors.[7] A study reported by Mourshed state that 1.44 per cent of impacted teeth may undergo Dentigerous cyst transformation.[8] as was found in our case report.
Rohilla et al. stated that Dentigerous cysts are frequently associated with impacted teeth and its occurrence in association with canines is frequent as the canines are the commonly impacted anterior teeth[9] as was found in our case report.
There is no evidence of Dentigerous cyst crossing the midline in the literature in various search engines like Medline, Cochrane and PubMed apart from a case report by Gonzalez et al. (2011) who reported a Dentigerous cyst encompassing the right and left impacted mandibular canines and crossing the midline. Hence, we are reporting this case, which is unique in its own kind as Dentigerous cyst has never been found to cross midline. This will be a great break-through in the classification of midline crossing cysts. The authors also stated that as Dentigerous cyst enlarges, it displaces the affected tooth or teeth apically, which was found in accordance to our case report.[10]
CONCLUSION
This new case presentation shows that a Dentigerous cyst might also cross the midline.[10] As Dentigerous cysts are asymptomatic, they can attain considerable size without the notice of the patient and this warrants an early clinical and radiographic detection of the cyst so that early treatment strategies will prevent or decrease the morbidity associated with the same.[11]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Scholl RJ, Kellett HM, Neumann DP, Lurie AG. Cysts and cystic lesions of the mandible: Clinical and radiologic-histopathologic review. Radiographics. 1999;19:1107–24. doi: 10.1148/radiographics.19.5.g99se021107. [DOI] [PubMed] [Google Scholar]
- 2.Desai RS, Vanaki SS, Puranik RS, Tegginamani AS. Dentigerous cyst associated with permanent central incisor: A rare entity. J Indian Soc Pedod Prev Dent. 2005;23:49–50. doi: 10.4103/0970-4388.16030. [DOI] [PubMed] [Google Scholar]
- 3.Kumar RV, Gunashekhar M. Dentigerous cyst in 8-year-old child–A case report. SRM Univ J Dent Sci. 2010;1:190–193. [Google Scholar]
- 4.Neyaz Z, Gadodia A, Gamanagatti S, Mukhopadhyay S. Radiographical approach to jaw lesions. Singapore Med J. 2008;49:165–76. [PubMed] [Google Scholar]
- 5.Shear M, Speight P. Cysts of the Oral and Maxillofacial Regions. 4th ed. Blackwell Publishing; 2007. Dentigerous cyst; p. 59. [Google Scholar]
- 6.Koseoglu BG, Atalay B, Erdem MA. Odontogenic cysts: A clinical study of 90 cases. J Oral Sci. 2004;46:253–7. doi: 10.2334/josnusd.46.253. [DOI] [PubMed] [Google Scholar]
- 7.Singh S, Singh M, Chhabra N, Nagar Y. Dentigerous cyst: A case report. J Indian Soc Pedod Prev Dent. 2001;19:123–6. [PubMed] [Google Scholar]
- 8.Mourshed F. A roentgenographic study of dentigerous cysts. II. Role of roentgenograms in detecting dentigerous cyst in the early stages. Oral Surg Oral Med Oral Pathol. 1964;18:54–61. doi: 10.1016/0030-4220(64)90256-7. [DOI] [PubMed] [Google Scholar]
- 9.Rohilla M, Namdev R, Dutta S. Dentigerous cyst containing multiple impacted teeth: A rare case report. J Indian Soc Pedod Prev Dent. 2011;29:244–7. doi: 10.4103/0970-4388.85834. [DOI] [PubMed] [Google Scholar]
- 10.Gonzalez SM, Spalding PM, Payne JB, Giannini PJ. A dentigerous cyst associated with bilaterally impacted mandibular canines in a girl: A case report. J Med Case Rep. 2011;5:230. doi: 10.1186/1752-1947-5-230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bhayya DP, Shyagali TR. Dentigerous cysts of inflammatory origin: A case report. Internet J Dent Sci. 2009;7:2. [Google Scholar]