

Abstract
Purpose
Systematic educational programs and genetic counseling certification courses for hereditary breast/ovarian cancer (HBOC) have not yet been introduced in Korea. We provided and evaluated the effects of genetic counseling education on Korean healthcare providers' knowledge, awareness, and counseling skills for patients at high risk of HBOC.
Methods
A 3-day educational program was conducted for healthcare providers who were interested in genetic counseling for patients at high risk of HBOC. Participants who completed a knowledge test and satisfaction questionnaire were included in the present sample. Pre-post comparisons were conducted to determine the effects of the intervention.
Results
Significant differences between preprogram and postprogram knowledge scores were observed (p=0.002). Awareness (p<0.001) and confidence (p<0.001) regarding genetic counseling significantly increased after the training. Doctors and participants with fewer years of work experience performed well on the knowledge test. Previous educational experience was correlated with increased confidence in knowledge and counseling skills.
Conclusion
Genetic counseling education regarding HBOC improved knowledge and awareness of HBOC and enhanced confidence in the counseling process. The effects varied according to occupation and participants' previous education. The implementation of systematic educational programs that consider participant characteristics may improve the effects of such interventions.
Keywords: Breast neoplasms, Education, Genetic counseling, Hereditary neoplastic syndromes
INTRODUCTION
Approximately 7% of breast cancer patients are considered to have genetic predispositions for cancer [1]. The incidence of breast cancer is increasing in Korea, with an age-standardized incidence rate of 27.1% in 2009. The proportion of breast cancer patients with family histories of breast cancer is currently estimated to be 7.5% [2]. In some countries, individuals can consult with certified genetic counselors. In the United States and Canada, the National Society of Genetic Counselors provides genetic counseling information, guidelines and policies regarding genetic counseling, genetic testing services, and education of genetic counselors [3-6]. Although genetic counseling educational programs for patients with hereditary breast/ovarian cancer (HBOC) have been introduced in Korea, they are not widely available. The lack of awareness of genetic counseling as well as a shortage of qualified genetic counselors are impediments to effective education of individuals at high risk of HBOC [7,8].
There is a growing demand for genetic counseling worldwide, which has led to shortages of genetic counselors and delays in timely, qualified counseling. Researchers have examined educational strategies such as videoconference-based genetic counseling, training nurses as counselors, interactive computer educational programs, group counseling, and dissemination of information booklets to help patients make informed decisions about treatments [9-13]. As there is no certified genetic counselor training program in Korea, typically doctors and research nurses, rather than certified counselors, offer genetic counseling to patients with HBOC. The Korean Hereditary Breast Cancer (KOHBRA) Study Group, which investigates HBOC and BRCA mutations in Koreans, has initiated educational programs for genetic counselors to meet patient needs and provided counseling scripts and educational leaflets for patients.
The aim of the present study is to determine the effects of educational programs on healthcare providers' knowledge of, awareness of, and confidence in genetic counseling of individuals at high risk of HBOC.
METHODS
The KOHBRA Study Group was organized in 2007 by the Korean Breast Cancer Society and is supported by the National Research and Development Program for Cancer Control of Korea. The KOHBRA Study Group has been investigating BRCA mutations in families with high risk of HBOC, developing a nationwide network of genetic counselors and providing genetic counseling services to families at high risk of HBOC.
A 3-day educational program on genetic counseling for patients at high risk of HBOC was conducted on June 24-26, 2011. The program included lectures (520 minutes) and hands-on practice sessions (400 minutes). The instructors were professionals in genetics, ethics, and psychiatry and expert clinicians in the management of hereditary breast cancer. The curriculum is described in Table 1. Hands-on practice sessions were held in a small-group discussion format to encourage the participation of all attendees. In risk assessment and pedigree drawing practice sessions, participants worked in pairs and performed the roles of counselee or counselor. A video of a mock genetic counseling session was shown before counseling practice sessions, and a counseling script was provided to each participant for practice.
Table 1.
Topics and contents of education program
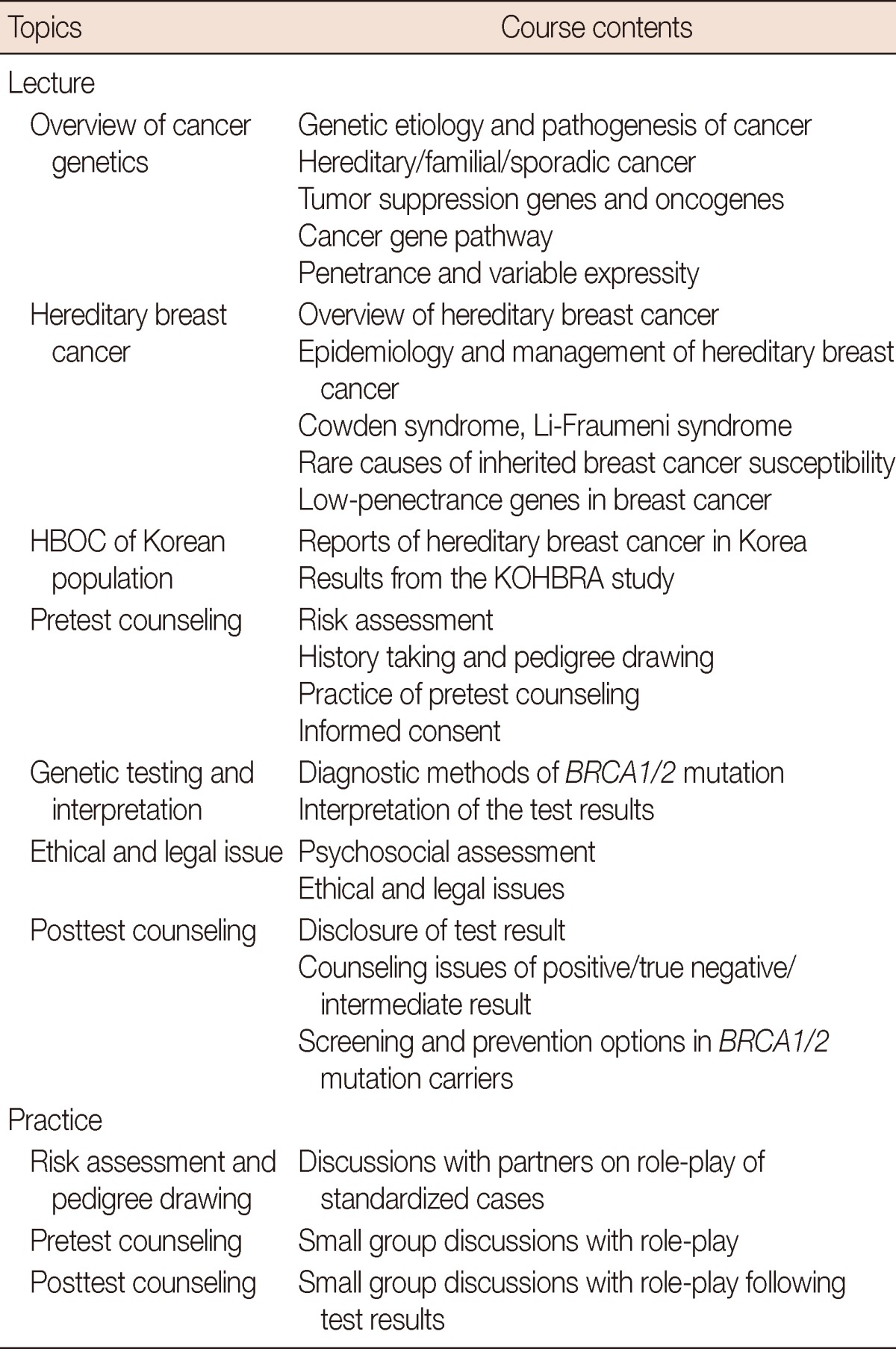
HBOC=hereditary breast and ovarian cancer; KOHBRA=Korean Hereditary Breast Cancer.
Healthcare providers willing to participate in the educational program were enrolled and provided with a questionnaire and a knowledge test. Self-reported questionnaires that assessed awareness of and confidence during genetic counseling, using a 5-point Likert scale (strongly agree, agree, neutral, disagree, strongly disagree), were completed before and after the educational program. The questionnaires consists of three subscales: awareness of genetic counseling education (AW); confidence in one's expertise to perform counseling (AK), including history taking, psychological assessment, risk assessment, genetic testing, hereditary breast cancer, individual screening and treatment plan, and psychological support, and confidence in the skill to perform the counseling process (AS), including skills to convey knowledge of hereditary cancer and the risks and benefits of testing, and to guarantee patient's confidentiality. Total scores ranging from 1 to 5 were calculated by summing the items and dividing by the number of total items to obtain a mean value. The questionnaires had good internal consistency (Cronbach's α=0.924 preprogram, 0.966 postprogram). In the postprogram questionnaire, participants were able to describe additional opinions regarding their overall perception of the educational program. Participants also completed a 49-item knowledge test designed to evaluate the effects of each lecture. The test consisted of true/false questions and was based on the curriculum. Each participant had 20 minutes to complete the knowledge test. Lack of response to any test item was regarded as an incorrect answer. To prevent memorization of answers from the preprogram test, some of the questions were re-worded and re-sequenced on the postprogram test.
Statistical analyses were performed using SPSS version 15.0 (SPSS Inc., Chicago, USA) to detect changes in knowledge, awareness, and confidence, and to analyze the influences of different demographic factors (gender, occupation, prior education, and occupational experiences). p-values less than 0.05 were considered statistically significant. A paired t-test was used to analyze the knowledge test and questionnaire results. To identify the effect of previous differences between groups, a t-test was first performed on the preprogram questionnaire and knowledge test results. If significant difference were found between groups in the analysis of the preprogram questionnaire, the authors used an analysis of covariance (ANCOVA) in the postprogram survey to control for the effects of covariates. Otherwise, t-tests were used to assess postprogram survey data.
RESULTS
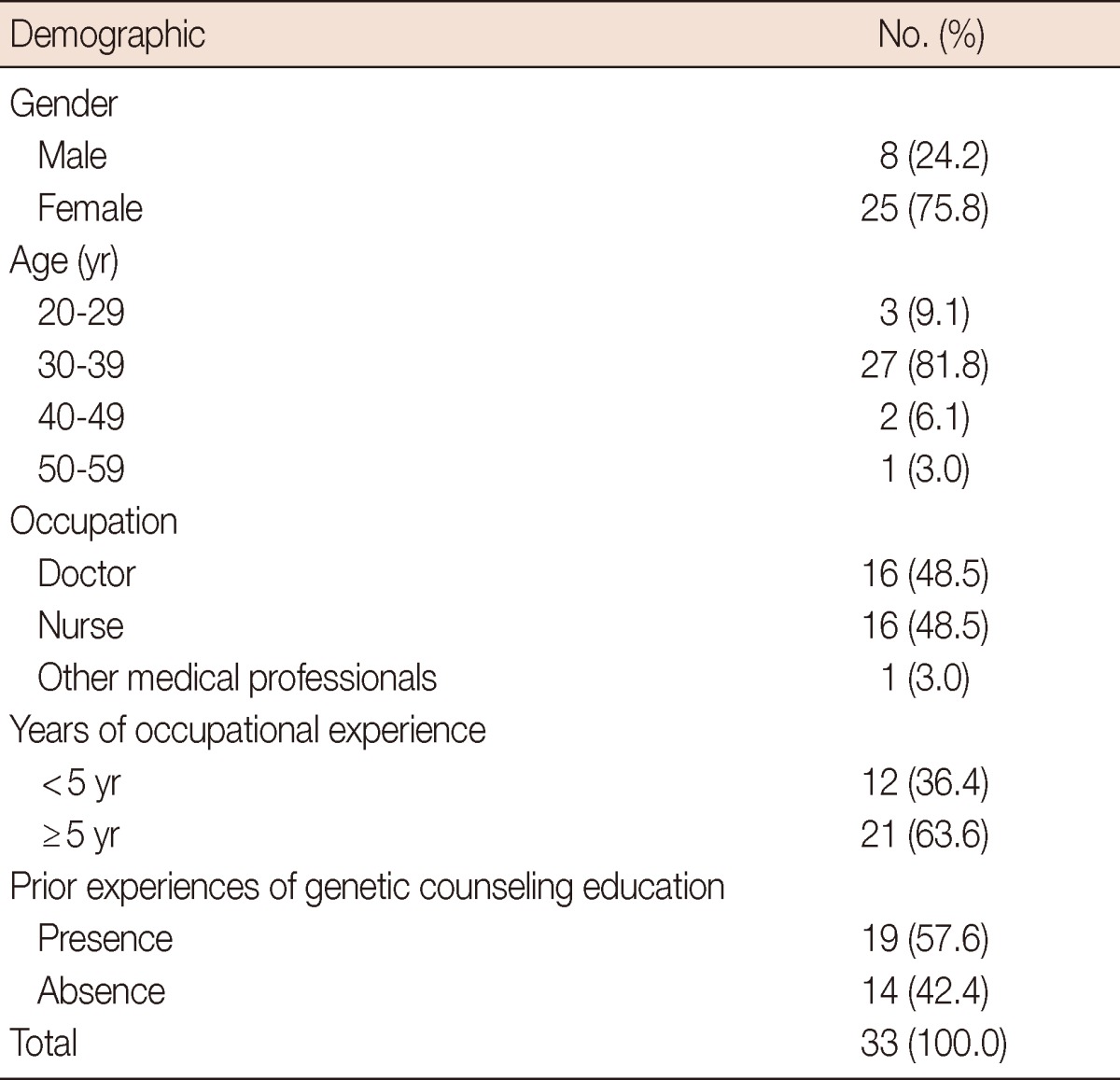
A total of 35 participants attended the genetic counseling educational program. Completed questionnaires assessing awareness and confidence (n=33) and paired knowledge tests (n=30) were analyzed. Table 2 describes the characteristics of the participants. Most were female (75.8%) and between the age of 30 and 39 years (81.8%). The percentages of doctors and nurses were similar (48.5%). Twenty-seven participants (81.8%) had more than 3 years of occupational experience. Nineteen participants (57.6%) had received prior genetic counseling education.
Table 2.
Demographics of respondents
Knowledge test
The mean score before the educational program was 37.4 out of 49. After the completion of the educational program, the mean score increased to 40.2 (Table 3), a statistically significant change (p=0.002). Scores for topical information, such as Korean epidemiological data regarding HBOC and the ethical and legal issues related to pretest counseling, tended to improve. However, scores decreased after education for some topics, such as cancer genetics, informed consent for pretest counseling, and posttest counseling.
Table 3.
Effect of education: influence on knowledge

Data are presented as mean±SD.
HBOC=hereditary breast and ovarian cancer; NS=not significant.
*Subdivisions of each topic.
Improvements of over 30% were achieved for the 8 questions that assessed knowledge about differences between hereditary, familial, and sporadic breast cancers; breast cancer risk reduction after risk-reducing salpingo-oophorectomy (RRSO); ovarian cancer surveillance protocols; mutations associated with hereditary breast cancer; elevated risk of endometrial carcinoma in Cowden syndrome; indications of the BRCA gene test; definition of "proband"; large genomic rearrangement; and genetic testing of carrier families. Three questions regarding missense mutations, the two-hit hypothesis, breast cancer surveillance of BRCA carriers, and confidentiality issues associated with genetic test results were repeated in preprogram and postprogram tests but the correct answer rates for these questions decreased by 30%.
The mean scores on the preprogram knowledge test were 37.9 for nurses and 36.7 for doctors; this difference was not significant (p=0.652). After education, the mean score increased to 41.3 for nurses and 39.3 for doctors. Both doctors and respondents with less occupational experience demonstrated significant improvements after receiving training (p=0.036 and p=0.028, respectively). Prior education experience and gender had no influence on achievement (p=0.628).
Awareness and confidence regarding genetic counseling
Thirty-three respondents completed the questionnaire, which was analyzed on three main subscales: AW, AK, and AS. Awareness of counseling and genetic counseling were included in the AW subscale. Essential knowledge about genetic counseling processes such as history taking, risk assessment and genetic testing was included in the AK subscale. Genetic counseling skills that convey knowledge to and reassure counselees were included in the AS subscale. Significant improvements were achieved in all three categories after the educational program (Table 4).
Table 4.
Participant's perception regarding performing genetic counseling
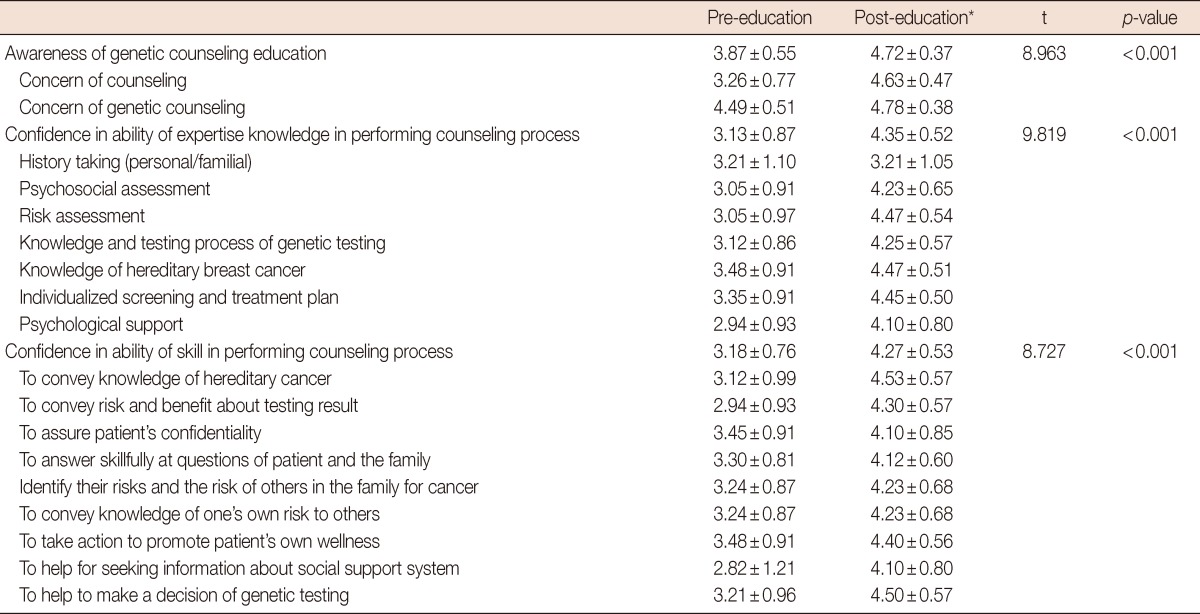
Data are presented as mean±SD.
*Data do not add up in analysis of change after the education on account of missing data.
Subgroup analyses of AW, AK, and AS are described in Tables 5 and 6. On the preprogram AW questionnaire, the perceived importance of genetic counseling was higher in men (p=0.010) and in participants who had prior educational experience (p=0.001). No differences were observed regarding occupation or length of occupational experience (p=0.374). After the educational program, male participants were strongly convinced of the importance of education (p=0.019). Confidence regarding knowledge required for genetic counseling (AK) was higher in men (p=0.023) and in doctors (p=0.002) before education. An increase in confidence after education was associated with male sex, being a doctor, and having prior educational experience (p=0.001, p=0.003, and p=0.023, respectively). Length of occupational experience was not associated with confidence in knowledge (p=0.665). Doctors showed increased confidence regarding genetic counseling skills (AS) after education (p=0.044). Doctors and those with prior education showed confident attitudes toward genetic counseling after education (p=0.032).
Table 5.
Subgroup analysis of knowledge score
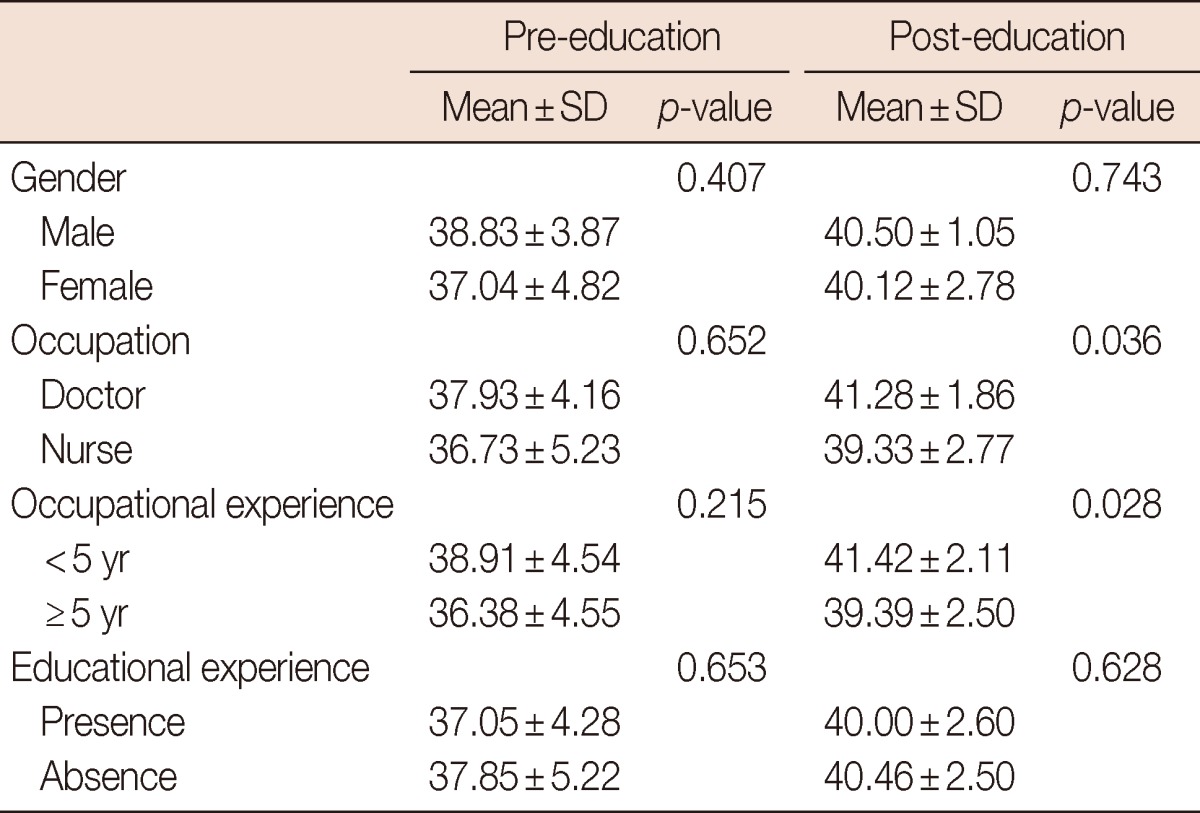
Table 6.
Subgroup analysis of awareness and confidence
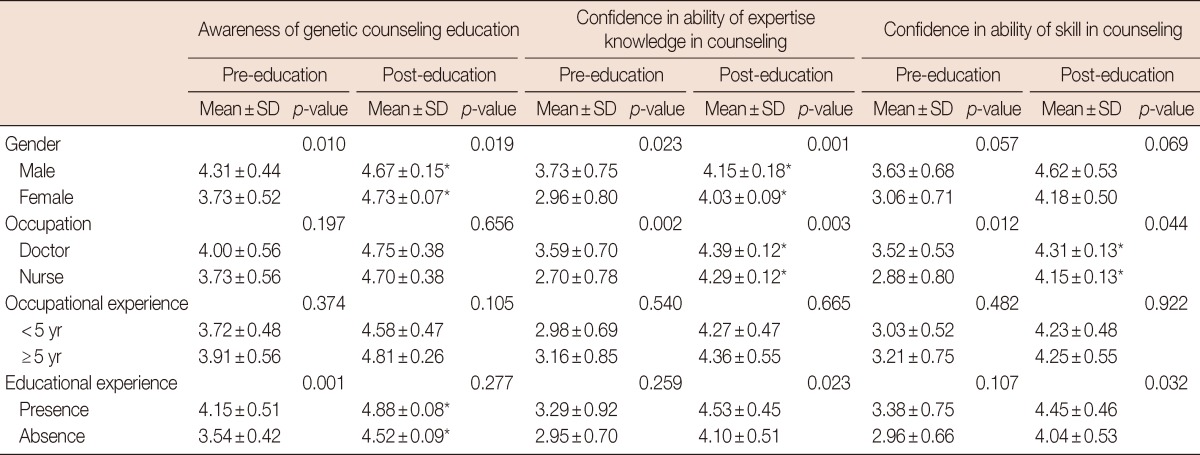
*Adjusted mean score using ANCOVA analysis.
Regarding the overall perceptions about the educational program, 6 out of 12 respondents emphasized the importance of communication skills. Most respondents requested more comprehensive educational programs about counseling practice.
DISCUSSION
We conducted an organized genetic counseling educational program for HBOC in Korea and evaluated its effects by assessing participant knowledge and perceptions. The program resulted in significant improvements in knowledge, awareness, and confidence regarding genetic counseling. We introduced two specific concepts of educational science to measure the effect of the educational program. The first one was changing the structure and/or words of a question to prevent memorization of its answer. The other was related to statistics. If there were no difference in the preprogram knowledge score, the effects of the educational program can be evaluated by a between-groups comparison of the scores on the postprogram knowledge test, using a t-test. Otherwise, if significant differences were shown, the two groups were compared using analysis of covariance (ANCOVA), taking preprogram differences into consideration.
Although, overall participants showed increased knowledge after education, there were neither significant changes nor achievements in some subsections. Therefore, gradual education should be planned using itemized subsections of genetic counseling topics. A systematized core curriculum for genetic counseling is also required.
Male participants showed increased awareness and confidence after completing the program compared to female participants. Although significant differences were found in knowledge scores, occupational experience showed no influence on AW, AK, and AS. Attainment of knowledge is an important outcome of educational programs, because conveying knowledge about genetics is a critical skill in genetic counseling. However, achievement of confidence is also important from a "counseling" perspective, because confidence can influence the quality of counseling.
Prior experience with genetic counseling education was associated with elevated awareness before education and with increased confidence on the AK and AS scales. Repeated educational experiences may be essential for developing qualified genetic counselors. To maximize the efficacy of genetic counseling education, systematic education is required through learner analysis that considers participant gender, occupation, and knowledge status. Further evaluations of participants by using different analytical tools may be useful for learner analysis and instruction design [14].
The majority of participants in the educational program desired access to more-advanced programs regarding practice and counseling skills. In the educational program that was provided, participants performed mock genetic counseling through role-play. Although role-play has been shown to be effective for medical education and genetic counseling education, the lack of realism may be a barrier to improving communication skills [15,16]. Supervised genetic counseling practice would be helpful to enhance counseling skills. Lindh et al. [17] emphasized the importance, methods, and barriers of clinical supervision in genetic counseling training. Trial and error, student feedback, consultations with colleagues, and using methods employed by one's own supervisors were major resources. Supervised education by genetic counselors should also be planned in Korea.
The basic concepts of genetics are included in the curriculum of medical schools, but healthcare providers remain unfamiliar with the genetic counseling process [18]. Doctors and nurses who staff breast clinics are a well-prepared student group for genetic counseling education, because they already have knowledge of basic genetics and breast cancer. Effective organization of educational content can promote genetic counseling knowledge and skills. Organized instruction that considers specific areas of knowledge and counseling skills is also required to implement advanced educational plans and improve patient satisfaction [19].
The limitation of this study is that we have too few participants for sufficiently high statistical power. The educational program was advertised via e-mail, as well as made available to the members of The KOHBRA Study Group and the Korean Breast Cancer Society. Participation was voluntary, making it hard to control the number of subjects and related variables for the study. While the questionnaire's internal consistency was assessed, preprogram and postprogram knowledge tests were conducted differently to prevent the memorization of answers; therefore, this practice might have affected the level of difficulty. Although the knowledge test was devised to reflect the content of the educational program, we found decreased knowledge in some subsections.
Genetic counseling may be provided by not only clinical geneticists and certified genetic counselors but also nurses and other trained health care professionals. Having the latter conduct genetic counseling might be cost-effective, particularly in Korea, where fees for genetic counseling are not currently reimbursed by the nationwide universal insurance system. Systematized core curricula of genetic counseling for nurses and other primary care providers assisting clinical geneticists is in the process of being implemented in Korea [20-22]. These professionals could provide genetic counseling for HBOC in the future. In the present study, a genetic counseling educational program was shown to be useful to improve participant knowledge as well as enhance awareness and confidence. It was particularly beneficial for doctors. Collaboration between doctors and nurses is necessary to provide high-quality genetic counseling. Structured educational training programs regarding genetic counseling of patients at high risk of HBOC are needed to meet public demand in Korea.
ACKNOWLEDGEMENTS
We would particularly like to thank all of the participants who completed questionnaires and joined in nationwide network of genetic counseling of hereditary breast-ovarian cancer. We also thank Eunyoung Kang, Sung-Won Kim, Cha Kyong Yom, Byung Ho Son, Sei-Hyun Ahn, Jong-Han Yu, Jong Won Lee, Dong-Young Noh, Hyeong-Gon Moon, Sue K. Park, Wonshik Han, Min Hyuk Lee, Sung Yong Kim, Young-Ik Hong, Lee Su Kim, Ki-Tae Hwang, Sei Joong Kim, Young Up Cho, Myung Chul Chang, Young Tae Bae, Yoon Joo Jung, Tae Woo Kang, Young Jin Suh, Sung Hoo Jung, Hyde Lee, Joon Jeong, Seok-Jin Nam, Jeong Eon Lee, Doo Ho Choi, Dae Sung Yoon, Il-Kyun Lee, Chang Hyun Lee, Byung-In Moon, Nam Sun Paik, Ku Sang Kim, Yongsik Jung, Sung Soo Kang, Seung Sang Ko, Chan Seok Yoon, Hae Kyung Lee, Min Hee Hur, Hai-Lin Park, Eundeok Chang, Sang Seol Jung, Keumhee Kwak, Sehwan Han, Yong Lai Park, Chan Heun Park, Eun-Kyu Kim, Hyun-Ah Kim, Woo-Chul Noh, Su Yun Choi, Sang Uk Woo, Se Jeong Oh, Tae Hyun Kim, Beom Seok Kwak, Jung-Hyun Yang, Young Bum Yoo, Byeong-Woo Park, Soo-Jung Lee, Sang Ah Han for participating the Korean Hereditary Breast Cancer Study.
This study was supported by a grant from the National R&D Program for Cancer Control, Ministry for Health, Welfare and Family Affairs, Republic of Korea (1020350).
Footnotes
This study was supported by a grant from the National R&D Program for Cancer Control, Ministry for Health, Welfare and Family Affairs, Republic of Korea (1020350).
The authors declare that they have no competing interests.
References
- 1.Claus EB, Schildkraut JM, Thompson WD, Risch NJ. The genetic attributable risk of breast and ovarian cancer. Cancer. 1996;77:2318–2324. doi: 10.1002/(SICI)1097-0142(19960601)77:11<2318::AID-CNCR21>3.0.CO;2-Z. [DOI] [PubMed] [Google Scholar]
- 2.The Korean Breast Cancer Society. Nationwide Korean breast cancer data of 2004 using breast cancer registration program. J Breast Cancer. 2006;9:151–161. [Google Scholar]
- 3.Robson ME, Storm CD, Weitzel J, Wollins DS, Offit K American Society of Clinical Oncology. American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol. 2010;28:893–901. doi: 10.1200/JCO.2009.27.0660. [DOI] [PubMed] [Google Scholar]
- 4.Berliner JL, Fay AM Practice Issues Subcommittee of the National Society of Genetic Counselors' Familial Cancer Risk Counseling Special Interest Group. Risk assessment and genetic counseling for hereditary breast and ovarian cancer: recommendations of the National Society of Genetic Counselors. J Genet Couns. 2007;16:241–260. doi: 10.1007/s10897-007-9090-7. [DOI] [PubMed] [Google Scholar]
- 5.American Society of Clinical Oncology. Resource document for curriculum development in cancer genetics education. J Clin Oncol. 1997;15:2157–2169. doi: 10.1200/JCO.1997.15.5.2157. [DOI] [PubMed] [Google Scholar]
- 6.Genetic/familial high-risk assessment: breast and ovarian - v.1. 2011. National Comprehensive Cancer Network; [Accessed April 13th, 2013]. http://www.nccn.org/professionals/physician_gls/pdf/genetics_screening.pdf. [Google Scholar]
- 7.Choi KS, Jun MH, Anderson G. The first Korean cancer genetic counseling program for nurses. J Korean Acad Soc Nurs Educ. 2006;12:104–114. [Google Scholar]
- 8.Choi KS, Jun MH, Ahn SH, Anderson G. Implementing and evaluating a nurse led hereditary cancer genetics educational program in a Korean breast cancer surgery clinic. J Korean Acad Adult Nurs. 2008;20:815–828. [Google Scholar]
- 9.Coelho JJ, Arnold A, Nayler J, Tischkowitz M, MacKay J. An assessment of the efficacy of cancer genetic counselling using real-time videoconferencing technology (telemedicine) compared to face-to-face consultations. Eur J Cancer. 2005;41:2257–2261. doi: 10.1016/j.ejca.2005.06.020. [DOI] [PubMed] [Google Scholar]
- 10.Hooker GW, Leventhal KG, Demarco T, Peshkin BN, Finch C, Wahl E, et al. Longitudinal changes in patient distress following interactive decision aid use among BRCA1/2 carriers: a randomized trial. Med Decis Making. 2011;31:412–421. doi: 10.1177/0272989X10381283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ridge Y, Panabaker K, McCullum M, Portigal-Todd C, Scott J, McGillivray B. Evaluation of group genetic counseling for hereditary breast and ovarian cancer. J Genet Couns. 2009;18:87–100. doi: 10.1007/s10897-008-9189-5. [DOI] [PubMed] [Google Scholar]
- 12.Mancini J, Noguès C, Adenis C, Berthet P, Bonadona V, Chompret A, et al. Impact of an information booklet on satisfaction and decision-making about BRCA genetic testing. Eur J Cancer. 2006;42:871–881. doi: 10.1016/j.ejca.2005.10.029. [DOI] [PubMed] [Google Scholar]
- 13.Masny A, Ropka ME, Peterson C, Fetzer D, Daly MB. Mentoring nurses in familial cancer risk assessment and counseling: lessons learned from a formative evaluation. J Genet Couns. 2008;17:196–207. doi: 10.1007/s10897-007-9140-1. [DOI] [PubMed] [Google Scholar]
- 14.Schwen TM. Learner analysis: some process and contents concerns. Av Commun Rev. 1973;21:44–72. [Google Scholar]
- 15.Nestel D, Tierney T. Role-play for medical students learning about communication: guidelines for maximising benefits. BMC Med Educ. 2007;7:3. doi: 10.1186/1472-6920-7-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.McIlvried DE, Prucka SK, Herbst M, Barger C, Robin NH. The use of role-play to enhance medical student understanding of genetic counseling. Genet Med. 2008;10:739–744. doi: 10.1097/GIM.0b013e318187762e. [DOI] [PubMed] [Google Scholar]
- 17.Lindh HL, Veach PM, Cikanek K, LeRoy BS. A survey of clinical supervision in genetic counseling. J Genet Couns. 2003;12:23–41. doi: 10.1023/A:1021443100901. [DOI] [PubMed] [Google Scholar]
- 18.Korf BR. Genetics and genomics education: the next generation. Genet Med. 2011;13:201–202. doi: 10.1097/GIM.0b013e31820986cd. [DOI] [PubMed] [Google Scholar]
- 19.Arranz P, Ulla SM, Ramos JL, Del Rincon C, Lopez-Fando T. Evaluation of a counseling training program for nursing staff. Patient Educ Couns. 2005;56:233–239. doi: 10.1016/j.pec.2004.02.017. [DOI] [PubMed] [Google Scholar]
- 20.Prows CA, Glass M, Nicol MJ, Skirton H, Williams J. Genomics in nursing education. J Nurs Scholarsh. 2005;37:196–202. doi: 10.1111/j.1547-5069.2005.00035.x. [DOI] [PubMed] [Google Scholar]
- 21.Carroll JC, Rideout AL, Wilson BJ, Allanson JM, Blaine SM, Esplen MJ, et al. Genetic education for primary care providers: improving attitudes, knowledge, and confidence. Can Fam Physician. 2009;55:e92–e99. [PMC free article] [PubMed] [Google Scholar]
- 22.Sussner KM, Jandorf L, Valdimarsdottir HB. Educational needs about cancer family history and genetic counseling for cancer risk among frontline healthcare clinicians in New York City. Genet Med. 2011;13:785–793. doi: 10.1097/GIM.0b013e31821afc8e. [DOI] [PMC free article] [PubMed] [Google Scholar]