

Abstract
We assessed if the Revised Child Anxiety and Depression Scale (RCADS) measures anxiety symptoms similarly across age groups within adolescence. This is crucial for valid comparison of anxiety levels between different age groups. Anxiety symptoms were assessed biennially in a representative population sample (n = 2226) at three time points (age range 10–17 years) using the RCADS anxiety subscales (generalized anxiety disorder [GAD], obsessive‐compulsive disorder [OCD], panic disorder [PD], separation anxiety [SA], social phobia [SP]). We examined longitudinal measurement invariance of the RCADS, using longitudinal confirmatory factor analysis, by examining the factor structure (configural invariance), factor loadings (metric invariance) and thresholds (strong invariance). We found that all anxiety subtypes were configural invariant. Metric invariance held for items on the GAD, OCD, PD and SA subscales; yet, for the SP subscale three items showed modest longitudinal variation at age 10–12. Model fit decreased modestly when enforcing additional constraints across time; however, model fit for these models was still adequate to excellent. We conclude that the RCADS measures anxiety symptoms similarly across time in a general population sample of adolescents; hence, measured changes in anxiety symptoms very likely reflect true changes in anxiety levels. We consider the instrument suitable to assess anxiety levels across adolescence. Copyright © 2013 John Wiley & Sons, Ltd.
Keywords: measurement invariance, longitudinal research, psychometrics, adolescents, anxiety
Introduction
The longitudinal course of anxiety is important to monitor since there is evidence that individuals with an earlier onset and more severe anxiety symptoms are at higher risk for anxiety disorders in childhood, adolescence and adulthood, as well as other mental disorders and impairments in adolescence and adulthood (Rueter et al., 1999; ter Wolbeek et al., 2011). For valid comparisons of anxiety symptom levels over time, in longitudinal studies, it is imperative to have questionnaires that measure anxiety subtypes similarly across time. Previous studies have acknowledged this relevance and have examined the longitudinal measurement stability (measurement invariance) of instruments assessing concepts such as borderline personality features (de Moor et al., 2009), late‐life functioning (Szabo et al., 2011) and body image (Rusticus et al., 2008). In the current study, we examined longitudinal measurement invariance of an instrument assessing anxiety symptoms from pre‐/early‐ through middle‐adolescence.
A variety of assessment methods for anxiety symptoms and disorders are available. In large, general population studies, self‐report questionnaires are an attractive alternative to clinical interviews. Furthermore, in a population sample, they are valid and relatively easy and time‐efficient to employ (Hale et al., 2005, 2008). Several standardized questionnaires with adequate psychometric properties are available that assess child and adolescent anxiety symptoms. The Revised Child Anxiety and Depression Scale (RCADS) (Chorpita et al., 2000) is a revision of the Spence Children's Anxiety Scale (SCAS) (Spence, 1997, 1998), adapted to more closely correspond with the DMS‐IV anxiety disorder classification (Chorpita et al., 2000, 2005). It is a self‐report questionnaire for children and adolescents between seven and 18 years, that consists of 47 items that cover five anxiety subscales, corresponding with the DSM‐IV categories of generalized anxiety disorder (GAD), obsessive‐compulsive disorder (OCD), panic disorder (PD), separation anxiety (SA) disorder and social phobia (SP), as well as major depression. Good reliability and validity has been established in community and clinical samples (Chorpita et al., 2000; de Ross and Gullone, 2002; Ferdinand et al., 2006).
Whereas the previous studies on the RCADS have focused on cross‐sectional structure and validity, the question remains whether the instrument measures symptoms of anxiety consistently over youth development. This question is addressed by examining longitudinal measurement invariance of the RCADS. With this procedure we examine if, given a certain level of anxiety, all individuals have the same probability of endorsing a certain answer on a certain item, irrespective of their age (de Moor et al., 2009). Examination of longitudinal measurement invariance is necessary for understanding whether observed changes in anxiety symptom scores across ages reflect true changes in symptoms or are due to changes in measurement properties of the instrument. Consistency in measurement properties is referred to as measurement invariance and supports that the individual items reflect the same psychometric information across longitudinal assessments, as investigated here, or across subgroups (e.g. gender, racial groups). A questionnaire that is not measurement invariant across age can provide invalid conclusions regarding continuity in measurement. A lack of longitudinal measurement invariance may indicate that the interpretation or relevance of the questionnaire items changes across time. As a consequence, differences in RCADS subscale scores between age groups would not automatically reflect a true change in anxiety symptom severity between these groups. However, if longitudinal measurement invariance is established, this suggests that a change in measured anxiety symptoms reflects a true change in the anxiety level across time.
In this paper, we examined the longitudinal measure stability of the RCADS subscales from pre‐adolescence to late adolescence in a large, representative, longitudinal population study.
Method
Study design and population
Participants were part of the Tracking Adolescents’ Individual Lives Survey (TRAILS), a large Dutch population cohort study designed to examine the development and etiological mechanisms of psychopathology from pre‐adolescents into adulthood. Participants were representative of the general population. They were assessed biennially from age 10–12 years onwards. Data were used from the first three waves of TRAILS: T1 (2001–2002; age range 10–12), T2 (2003–2004; age range 12–15) and T3 (2005–2007; age range 14–18).
More details of TRAILS have been described elsewhere (de Winter et al., 2005; Huisman et al., 2008) and are available upon request. In short, participants were recruited from the general population in five municipalities in the northern part of the Netherlands, including both urban and rural areas. Exclusion criteria were non‐participation of the school and inability to participate in the study due to severe mental retardation, a severe physical illness, or language‐limitations. Extensive efforts were taken to minimize non‐response, including reminder letters and personal house visits. Of the initial 3483 pre‐selected children, 2935 proved eligible for the study, of which 2230 (76%, of which 51% girls) responded for the first wave. At T2, n = 2149 (96.4%, of which 51% girls) continued to participate. At T3, participation in the study was impossible for 42 subjects due to severe mental or physical health problems, death, detention, emigration or because they were untraceable. Of the remaining subjects, n = 1816 (83%, of which 53% girls) continued to participate.
The vast majority of the respondents provided complete RCADS information (missing not more than one item on one subscale at T1 = 99.6%, T2 = 99.9%, T3 = 98.8%). There was little unavailable RCADS data at T1, (n = 20), at T2, (n = 65), and at T3 (n = 156). Of our whole sample (n = 2230), n = 4 respondents did not provide any RCADS information at any time point; these respondents were excluded from the analyses. The remaining missing values were excluded pairwise and treated as MCAR, which is the default implementation for the WLSMV estimator in analyses without covariates. We have not used an algorithm to estimate missing values.
Non‐response bias of the TRAILS sample was analyzed based on information about mental health determinants and outcomes as reported by teachers of responders and non‐responders (de Winter et al., 2005). No difference in the prevalence of psychopathology was found at T1 or T2. Also, responders and non‐responders did not differ regarding their associations between socio‐demographic variables and mental health outcomes. Informed consent was obtained at each assessment wave from each participant and their parents. The study was approved by the Dutch Central Medical Ethics Committee (CCMO) and all participants were compensated for their involvement in this study.
Measures
Anxiety symptoms were assessed by the Dutch translation of the RCADS (Chorpita et al., 2000). The RCADS is a self‐report questionnaire, consisting of 47‐items measuring five anxiety subtypes and depression symptoms (Chorpita et al., 2000). Chorpita et al. (2000) showed good reliability and internal consistency (GAD = 0.79, α = 0.77; OCD = 0.65, α = 0.73; PD = 0.76, α = 0.79; SA = 0.75, α = 0.76; SP = 0.80, α = 0.82; MDD = 0.77, α = 0.76) as well as convergent and discriminant validity in a sample of n = 246 children and adolescents aged 8–18 years (Chorpita et al., 2000). It is scored on a four‐point Likert scale (0 = never, 1 = sometimes, 2 = often, 3 = always). Due to the infrequent endorsement of the answer category “always”, we merged answer categories “often” and “always”, rendering a three‐point Likert scale ranging from zero to two. Our analysis focused on the 37 items that assess five anxiety subscales: GAD (six items, ordinal coefficient α = 0.85/ 0.89/ 0.88 at the three waves), OCD (six items, ordinal coefficient α = 0.76/ 0.81/ 0.84), PD (nine items, ordinal coefficient α = 0.85/ 0.90/ 0.90), SA disorder (seven items, ordinal coefficient α = 0.78/ 0.83/ 0.83) and SP (nine items, ordinal coefficient α = 0.84/ 0.90/ 0.91). The factor structure as proposed by the RCADS was replicated in the TRAILS sample for data from the first assessment wave (Ferdinand et al., 2006).
The majority of the RCADS anxiety items were previously translated to Dutch as part of the SCAS (Scholing, 2000; Spence, 1997, 1998) items not included in the SCAS were translated to Dutch and back‐translated to English in a combined effort of a study PI and a bilingual employee of the University of Groningen language center.
Statistical analysis
To determine the level of longitudinal invariance, we examined whether the factor structure of the RCADS anxiety subscales remains invariant across age groups, adopting a confirmatory factor analysis (CFA) framework. Complete examination of measurement invariance involves a four‐step process where in each step, one additional restriction across age groups is imposed on the measurement model (Meredith, 1993; Widaman and Reise, 1997). Model fit of each of these nested models was compared with that of the less restricted model. Full invariance on each level is reached if the model fit itself is adequate, and if the model fit of the more restrictive model is not considerably less than that of the less restrictive model (Meredith, 1993; Widaman and Reise, 1997).
We examined longitudinal invariance on the first three levels by fitting a one‐factor model to the data including the three assessments over adolescence, for each RCADS anxiety subscale. The first level of longitudinal invariance is configural invariance, which imposes the same pattern of fixed and free factor loadings between age groups, while not making any equality constraints. We examined configural invariance by fitting the hypothesized RCADS factor structure (i.e. which items load on which anxiety subscale) to the data for all three age groups (see Figure 1a for illustration of this model). The second level is metric (or weak) invariance, which examines if factor loadings to each item are equal across age groups. Thus, metric invariance is examined by constraining the factor loadings across age groups (see Figure 1b). The third level is strong (or scalar) invariance, which examines if the means structure is longitudinally invariant. When observed indicators are continuous variables, examination of strong invariance involves testing whether the intercepts of the indicators differ across time. However, as the RCADS consists of ordinal categorical items, we examined strong invariance by restricting each threshold per item to be equal to its corresponding threshold across the measured time points. This procedure is based on the assumption that answer category endorsement for each item is driven by the underlying true anxiety level of the subject. The threshold parameter indicates the true (latent) anxiety level where half of the sample endorses the lower answer category (e.g. 0 “never”) and half endorses the next higher one (e.g. 1 “sometimes”). Hence, the number of thresholds per variable is equal to the number of answer categories minus one. When examining strong invariance by setting the threshold parameters of the items to be equal to each other, as described earlier, what is actually being estimated under the measurement invariance framework is the differences amongst the thresholds, not the absolute value of the threshold. This means that the pattern of all the thresholds together is fixed across the different time points, e.g. if one threshold of item a is lower that the corresponding threshold of item b, this has to be proportionally the same for all time points. Importantly, as a consequence of estimating the differences amongst thresholds and not their absolute value, the mean of the latent variable is not restricted and hence can vary over time. If strong invariance holds, the change in anxiety subscale scores reflects a change in true anxiety subtype levels. The fourth step is an examination of strict invariance, which measures whether the indicator residual variances are equal across age groups. The relevance of strict invariance examination has been generally disputed, as residual variance equality may have limited clinical and practical utility (Little et al., 2007).
Figure 1.
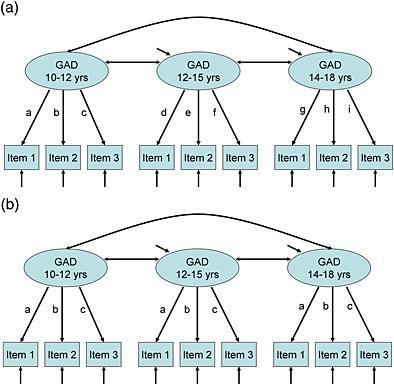
(a) A configural invariance model with factor loadings unrestrained. (b) A metric invariance model with factor loadings restrained across age groups.
Depending on the construct to be measured, different levels of invariance are realistic to expect. Few self‐report questionnaires pass strong or strict invariance examination, and a recommendation is to only consider configural and metric invariance, as developmental effects are expected that would render strong invariance unrealistic (Horn and McArdle, 1992).
We examined the model fit of all the invariance models and inspected the modification indices of each parameter in each specified model. The modification index is a post hoc indicator that indicates model fit improvement when a fixed parameter is freely estimated (Brown, 2006). Previous research with psychological constructs has shown that it is often necessary to allow for correlated errors between items with non‐random measurement error due to similar item formulation or narrowly associated item content (Byrne et al., 1989). Therefore, we allowed for residual error correlations of two or three items in each nested anxiety subscale, provided that the modification included items with similar content or phrasing (i.e. items had very similar formulation or measured one specific aspect within an anxiety subscale). The models with correlated residuals were used for evaluation of model fit to examine longitudinal invariance (items with correlated residual error terms are indicated later in Table 3). Model fit indices of the original, uncorrelated anxiety subscales are available upon request from the first author.
Table 3.
Standardized factor loading estimates of the configural (unrestricted) model across three age groups as well as the metric (restricted) model
| Factor | Item # | Item description | Factor loading | |||
|---|---|---|---|---|---|---|
| Configural | Metric | |||||
| T1 | T2 | T3 | ||||
| GAD | 1 | Worries about things | 0.55 | 0.64 | 0.67 | 0.60 |
| GAD | 13 | Worries something awful will happen to family | 0.70 | 0.75 | 0.70 | 0.69 |
| GAD | 22a | Worries bad things will happen to self | 0.82 | 0.88 | 0.83 | 0.81 |
| GAD | 27a | Worries something bad will happen to self | 0.80 | 0.85 | 0.84 | 0.80 |
| GAD | 35 | Worries about what will happen | 0.73 | 0.78 | 0.80 | 0.74 |
| GAD | 37 | Thinks about death | 0.59 | 0.60 | 0.55 | 0.56 |
| OCD | 10a | Has to do things just right to stop bad events | 0.53 | 0.61 | 0.57 | 0.52 |
| OCD | 16 | Bothered by bad or silly thoughts or images | 0.51 | 0.55 | 0.60 | 0.51 |
| OCD | 23a | Has to do things over and over again | 0.57 | 0.61 | 0.59 | 0.54 |
| OCD | 31 | Keeps checking if things done right | 0.65 | 0.75 | 0.75 | 0.65 |
| OCD | 42 | Can't get bad or silly thoughts out of head | 0.55 | 0.61 | 0.75 | 0.58 |
| OCD | 44 | Has to think special thoughts to stop bad events | 0.66 | 0.70 | 0.82 | 0.66 |
| PD | 3a | When has a problem, stomach feels funny | 0.43 | 0.51 | 0.54 | 0.46 |
| PD | 14 | Suddenly has trouble breathing for no reason | 0.63 | 0.76 | 0.67 | 0.64 |
| PD | 24a | When has a problem, heart beats really fast | 0.53 | 0.59 | 0.60 | 0.53 |
| PD | 26 | Suddenly trembles or shakes for no reason | 0.65 | 0.71 | 0.75 | 0.65 |
| PD | 28a | When has a problem, feels shaky | 0.54 | 0.65 | 0.69 | 0.57 |
| PD | 34 | Suddenly feels really scared for no reason | 0.68 | 0.77 | 0.82 | 0.69 |
| PD | 36 | Suddenly becomes dizzy of faint for no reason | 0.64 | 0.70 | 0.67 | 0.62 |
| PD | 39 | Heart suddenly beats too quickly for no reason | 0.76 | 0.79 | 0.79 | 0.72 |
| PD | 41 | Worries will suddenly get scared for no reason | 0.65 | 0.78 | 0.76 | 0.67 |
| SA | 5a | Fears being alone at home | 0.62 | 0.68 | 0.67 | 0.65 |
| SA | 9 | Fears being away from parents | 0.56 | 0.61 | 0.61 | 0.59 |
| SA | 17a | Scared to sleep alone | 0.71 | 0.73 | 0.69 | 0.71 |
| SA | 18 | Trouble going to school | 0.53 | 0.64 | 0.65 | 0.60 |
| SA | 33 | Afraid of being in crowded places | 0.50 | 0.60 | 0.59 | 0.56 |
| SA | 45 | Worries in bed at night | 0.52 | 0.53 | 0.51 | 0.52 |
| SA | 46 | Scared to sleep away from home | 0.62 | 0.69 | 0.75 | 0.67 |
| SP | 4 | Worries when does poorly at things | 0.57 | 0.71 | 0.73 | 0.68 |
| SP | 7a | Scared to take a test | 0.39 | 0.56 | 0.56 | 0.51 |
| SP | 8 | Feels worried when someone angry | 0.61 | 0.69 | 0.69 | 0.66 |
| SP | 12a | Worries will do badly at school work | 0.53 | 0.67 | 0.66 | 0.63 |
| SP | 20 | Worries might look foolish | 0.74 | 0.80 | 0.82 | 0.79 |
| SP | 30 | Worries about mistakes | 0.60 | 0.73 | 0.76 | 0.71 |
| SP | 32 | Worries what others think | 0.73 | 0.82 | 0.83 | 0.80 |
| SP | 38 | Afraid to talk in front of class | 0.49 | 0.57 | 0.56 | 0.54 |
| SP | 43 | Afraid of looking foolish in front of people | 0.76 | 0.80 | 0.85 | 0.81 |
Note: GAD, generalized anxiety disorder; OCD, obsessive‐compulsive disorder; PD, panic disorder; SA, separation anxiety disorder; SP, social phobia.
Indicates correlated items within one anxiety subscale.
Model fit indices used were the comparative fit index (CFI), (Bentler, 1990; Hu and Bentler, 1998) the Tucker–Lewis Index (TLI) (Tucker and Lewis, 1973) and the root mean square error of approximation (RMSEA) (Steiger, 1990). We did not rely on the Chi Square test as a primary indicator of model fit due to concerns about sensitivity to large sample sizes (Schermelleh‐Engel et al., 2003). Good model fit is indicated by a CFI of 0.95 or higher (Hu and Bentler, 1998; Schermelleh‐Engel et al., 2003), a TLI of 0.97 or higher (Schermelleh‐Engel et al., 2003) and a RMSEA of 0.05 or lower (Schermelleh‐Engel et al., 2003). Acceptable model fit is indicated by a CFI greater than 0.90, a TLI greater than 0.95 and a RMSEA smaller than 0.08 (Schermelleh‐Engel et al., 2003).
Model fit of each individual model was evaluated with the CFI, TLI and RMSEA. Next, model fit of each nested, more restricted model was compared with that of the less restricted model using the CFI as indicator. For nested model comparison, we used the ΔCFI test. This test is more robust against large sample sizes than the Chi‐square difference test. A CFI decrease of more than 0.005 from the less restricted model to the more restricted model was used as indicator for worse model fit (Cheung and Rensvold, 2002). All examinations of measurement invariance were conducted using longitudinal confirmatory factor analysis with ordinal categorical data using the weighted least square mean and variance (WLSMV) adjusted estimator (Millsap and Yun‐Tein, 2004) in Mplus Version 5 (Múthen and Múthen, 1998–2007).
Results
Table 1 shows the mean anxiety subtype levels at each of the assessment waves of TRAILS. Table 2 shows the model fit of the models with configural invariance, metric invariance and strong invariance, by anxiety subscale. Table 3 gives the factor loadings of the models with configural invariance. In the configural models, items are forced to load on a specific factor, but the factor loadings of the items are estimated freely. All anxiety subscales show a good model fit on the configural level (all CFI > 0.95; TLI > 0.97; RMSEA < 0.05), indicating that the factor structure of the RCADS anxiety subscales fits each of the age groups across adolescence.
Table 1.
Demographic characteristics and anxiety subtype levels of the TRAILS sample at T1, T2 and T3
| Assessment wave | T1 (2001–2002) | T2 (2003–2004) | T3 (2005–2007) |
|---|---|---|---|
| Age, mean (SD); range | 11.1 (0.56); 10.1–12.6 years | 13.6 (0.53); 12.2–15.2 years | 16.3 (0.71); 14.7–18.7 years |
| Anxiety, mean (SD), range | |||
| GAD | 0.65 (0.42), 0–2.0 | 0.48 (0.40), 0–2.0 | 0.51 (0.40), 0–2.0 |
| OCD | 0.57 (0.40), 0–2.0 | 0.33 (0.33), 0–2.0 | 0.28 (0.33), 0–2.0 |
| PD | 0.41 (0.33), 0–2.0 | 0.29 (0.30), 0–2.0 | 0.28 (0.28), 0–2.0 |
| SA | 0.36 (0.32), 0–1.7 | 0.23 (0.27), 0–1.6 | 0.22 (0.25), 0–1.4 |
| SP | 0.75 (0.39), 0–2.0 | 0.66 (0.43), 0–2.0 | 0.70 (0.45), 0–2.0 |
Note: SD, standard deviation; GAD, generalized anxiety disorder; OCD, obsessive‐compulsive disorder; PD, panic disorder; SA, separation anxiety disorder; SP, social phobia.
Table 2.
Model fitting results for measurement invariance examined across three age groups
| χ 2 | df | #par | CFI | TLI | RMSEA | |
|---|---|---|---|---|---|---|
| GAD | ||||||
| Configural | 226.647 | 63 | 78 | 0.987 | 0.992 | 0.034 |
| Metric | 222.639 | 66 | 68 | 0.988a | 0.993 | 0.033 |
| Strong | 433.841 | 80 | 46 | 0.972 | 0.987 | 0.045 |
| OCD | ||||||
| Configural | 221.430 | 80 | 78 | 0.974 | 0.979 | 0.028 |
| Metric | 210.414 | 80 | 68 | 0.976a | 0.981 | 0.027 |
| Strong | 395.729 | 96 | 46 | 0.944 | 0.963 | 0.037 |
| PD | ||||||
| Configural | 424.750 | 149 | 120 | 0.958 | 0.981 | 0.029 |
| Metric | 366.538 | 139 | 104 | 0.965a | 0.983 | 0.027 |
| Strong | 506.312 | 156 | 70 | 0.947 | 0.976 | 0.032 |
| SA | ||||||
| Configural | 292.202 | 107 | 90 | 0.963 | 0.974 | 0.028 |
| Metric | 260.875 | 98 | 76 | 0.967a | 0.975 | 0.027 |
| Strong | 511.463 | 112 | 50 | 0.920 | 0.947 | 0.040 |
| SP | ||||||
| Configural | 627.470 | 155 | 114 | 0.964 | 0.986 | 0.037 |
| Metric | 929.248 | 128 | 96 | 0.939 | 0.971 | 0.053 |
| Strong | 1273.453 | 143 | 62 | 0.914 | 0.963 | 0.060 |
Note: GAD, generalized anxiety disorder; OCD, obsessive‐compulsive disorder; PD, panic disorder; SA, separation anxiety disorder; SP, social phobia; df, degrees of freedom; #par, number of parameters; CFI, comparative fit index; TLI, Tucker–Lewis Index; RMSEA, root mean square error of approximation.
CFI decrease smaller than 0.005.
The model fit of the metric model was good for GAD, OCD, PD and SA, and acceptable for SP. The last column of Table 3 shows the metric invariance factor loading of the models where items were forced to load on a specific factor and to have the same factor loadings at the three age groups. The difference in CFI compared with the configural model exceeded 0.005 for SP only. Hence, on the metric invariance level, the subscales for GAD, OCD, PD and SA were fully longitudinal invariant, but the subscale for SP was not. For SP, we inspected the modification indices of the metric model to find out which items had factor loadings that differed across assessment wave. For three items, modification indices were above 100 (item 4 “Worries when does poorly at things”, 7 “Scared to take a test”, and 30 “Worries about mistakes”), all at age 10–12. These items loaded lower on the SP factor at age 10–12 (T1) than at ages 12–18 (T2 and T3; see Table 3). After allowing age‐specific factor loadings for these three items, the CFI difference with the configural model did not exceed 0.005 and the model fit of the SP subscale improved from acceptable to good (CFI = 0.959, TLI = 0.981, RMSEA = 0.043).
For the strong invariance examination, we constrained the thresholds of each item to be equal across age groups. With this procedure we examine whether the likelihood of response endorsement is driven by the underlying true anxiety level of the subject. The model fit was good for the GAD subscale, acceptable to good for OCD, PD and SA, and acceptable for SP. When comparing this strong invariance model with the metric model, however, the difference in CFI exceeded the 0.005 criteria for all anxiety subscales, indicating a deterioration in model fit.
Discussion
Measurement stability is critically important for longitudinal studies, yet few investigations have examined this issue in anxiety assessment instruments. The present study examined the longitudinal measurement stability in youth across three waves including pre‐ through late‐adolescence in the general population using a CFA framework.
In the RCADS, each of the anxiety subscales had the same factor patterns across age groups and the GAD, OCD, PD and SA subscales demonstrated similar factor loadings across age as well. This work suggests that each of the items comprising these specific subscales contribute equally to these domains across development. The SP subscale, however, included three items (out of nine) that had different factor loadings across time, in particular items of anxiety about self‐evaluated poor performance. These items had stronger loadings from the SP latent factor for the latter two assessments (ages 12–18) than at the first assessment (ages 10–12). The SP scale includes symptoms related to social interaction as well as symptoms of performance anxiety. These symptoms often co‐occur, yet evidently describe different aspects of social phobia (Heimberg et al., 1993; Knappe et al., 2011). Our data show that their relative importance is not stable over time, but that performance anxiety becomes more important in the context of social phobia symptoms across adolescent development. We can only speculate on the reasons why performance anxiety becomes more important. It is possible that the increased importance of performance anxiety is caused by increased levels of depression symptoms over adolescence, such as feelings of worthlessness or incompetence, or by increased academic pressure.
The model fit of the strong invariance models decreased significantly; however, on an absolute level, they were still acceptable to good for all anxiety subscales. This indicates only small deviations from strong longitudinal invariance. We did not expect to find full strong longitudinal invariance. Indeed, as a consequence of children's development, the expression of anxiety subtypes changes across developmental stages, which can be expected to be reflected in different item endorsement (Dadds and Barrett, 2001).
To our knowledge, the only other youth anxiety assessing instrument that has been examined for longitudinal measurement invariance is the SCAS (Spence, 1997). Spence (1997) examined measurement invariance of the SCAS across two age groups (younger than 11 years versus 11 years and older) and found the instrument to be configural invariant. However, metric invariance already proved to be suboptimal and the strong invariance examination did not hold. Hence, the RCADS has more favourable longitudinal measurement invariance properties than the SCAS.
The current study has several strengths and limitations. The main strength is that we used a large adolescent sample representative of the general population of adolescents in the Netherlands, assessed with a high response at three time points, describing the age range from 10 to 18 years. Each assessment point covers a narrow age range of two to four years, which minimizes the risk of making unjustified assumptions about invariance within one time point. However, this study was limited to this age range and does not guarantee longitudinal invariance for younger ages. Due to low endorsement of the answer category “always”, we had to combine answer categories “often” and “always” to obtain reliable results from our analyses. It could be important for future work to examine similar issues with an enriched sample of anxious youth to examine the full set of response options. Lastly, we did not include any infrequency scales in the TRAILS study to detect (pseudo)random answering patterns; however, the RCADS is a questionnaire with low risk for typical (pseudo)random answering. Future longitudinal studies of anxiety symptoms in the general population will give more insight in the factors that contribute to continuity and discontinuity of anxiety, and identify youth requiring early interventions and possible prevention of anxiety disorders.
Conclusion
The RCADS measures anxiety subtypes similarly across time in a general population sample of adolescents; that is, the measured changes in anxiety subscales very likely reflect true changes in anxiety levels as opposed to measurement artefacts. Some caution should be exercised due to the minor adjustments made to improve the model fits, especially for the SP subscale, where additional adjustments were needed for adequate metric invariance model fit. Nonetheless, this research suggests that the RCADS is very likely suitable to compare anxiety levels in longitudinal, population based studies of adolescents.
Declaration of interest statement
The authors have no competing interests.
Acknowledgments
This research is part of the TRacking Adolescents’ Individual Lives Survey (TRAILS). Participating centers of TRAILS include various departments of the University Medical Center and University of Groningen, the Erasmus University Medical Center Rotterdam, the University of Utrecht, the Radboud Medical Center Nijmegen, and the Parnassia Bavo group, all in the Netherlands. TRAILS has been financially supported by various grants from the Netherlands Organization for Scientific Research NWO (Medical Research Council program grant GB‐MW 940‐38‐011; ZonMW Brainpower grant 100‐001‐004; ZonMw Risk Behavior and Dependence grants 60‐60600‐98‐018 and 60‐60600‐97‐118; ZonMw Culture and Health grant 261‐98‐710; Social Sciences Council medium‐sized investment grants GB‐MaGW 480‐01‐006 and GB‐MaGW 480‐07‐001; Social Sciences Council project grants GB‐MaGW 457‐03‐018, GB‐MaGW 452‐04‐314, and GB‐MaGW 452‐06‐004; NWO large‐sized investment grant 175.010.2003.005; NWO Longitudinal Survey and Panel Funding 481‐08‐013); the Sophia Foundation for Medical Research (projects 301 and 393), the Dutch Ministry of Justice (WODC), the European Science Foundation (EuroSTRESS project FP‐006), and the participating universities. The authors are grateful to all adolescents, their parents and teachers who participated in this research and to everyone who worked on this project and made it possible.
References
- Bentler P.M. (1990) Comparative fit indexes in structural models. Psychological Bulletin, 107(2), 238–246, DOI: 10.1037/0033-2909.107.2.238 [DOI] [PubMed] [Google Scholar]
- Brown T.A. (2006) Confirmatory Factor Analysis for Applied Research. New York: The Guilford Press. [Google Scholar]
- Byrne B.M., Shavelson R.J., Muthen B. (1989) Testing for the equivalence of factor covariance and mean structures – the issue of partial measurement invariance. Psychological Bulletin, 105(3), 456–466, DOI: 10.1037/0033-2909.105.3.456 [DOI] [Google Scholar]
- Cheung G.W., Rensvold R.B. (2002) Evaluating goodness‐of‐fit indexes for testing measurement invariance. Structural Equation Modeling, 9(2), 233–255, DOI: 10.1207/s15328007sem0902_5 [DOI] [Google Scholar]
- Chorpita B.F., Moffitt C.E., Gray J. (2005) Psychometric properties of the Revised Child Anxiety and Depression Scale in a clinical sample. Behaviour Research and Therapy, 43(3), 309–322, DOI: 10.1016/j.brat.2004.02.004 [DOI] [PubMed] [Google Scholar]
- Chorpita B.F., Yim L., Moffitt C., Umemoto L.A., Francis S.E. (2000) Assessment of symptoms of DSM‐IV anxiety and depression in children: a Revised Child Anxiety and Depression Scale. Behaviour Research and Therapy, 38(8), 835–855, DOI: 10.1016/s0005-7967(99)00130-8 [DOI] [PubMed] [Google Scholar]
- Dadds M.R., Barrett P.M. (2001) Practitioner review: psychological management of anxiety disorders in childhood. Journal of Child Psychology and Psychiatry and Allied Discipline, 42(8), 999–1011, DOI: 10.1111/1469-7610.00798 [DOI] [PubMed] [Google Scholar]
- Ferdinand R.F., van Lang N.D., Ormel J., Verhulst F.C. (2006) No distinctions between different types of anxiety symptoms in pre‐adolescents from the general population. Journal of Anxiety Disorders, 20(2), 207–221, DOI: 10.1016/j.janxdis.2004.12.003 [DOI] [PubMed] [Google Scholar]
- Hale W.W., Raaijmakers Q., Muris P., Meeus W. (2005) Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED) in the general adolescent population. Journal of the American Academy of Child and Adolescent Psychiatry, 44(3), 283–290, DOI: 10.1097/00004583-200503000-00013 [DOI] [PubMed] [Google Scholar]
- Hale W.W., Raaijmakers Q., Muris P., van Hoof A., Meeus W. (2008) Developmental trajectories of adolescent anxiety disorder symptoms: a 5‐year prospective community study. Journal of the American Academy of Child and Adolescent Psychiatry, 47(5), 556–564, DOI: 10.1097/CHI.0b013e3181676583 [DOI] [PubMed] [Google Scholar]
- Heimberg R.G., Holt C.S., Schneier F.R., Spitzer R.L., Liebowitz M.R. (1993) The issue of subtypes in the diagnosis of social phobia. Journal of Anxiety Disorders, 7(3), 249–269, DOI: 10.1016/0887-6185(93)90006-7 [DOI] [Google Scholar]
- Horn J.L., McArdle J.J. (1992) A practical and theoretical guide to measurement invariance in aging research. Experimental Aging Research, 18(3–4), 117–144. [DOI] [PubMed] [Google Scholar]
- Hu L.T., Bentler P.M. (1998) Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods, 3(4), 424–453, DOI: 10.1037/1082-989x.3.4.424 [DOI] [Google Scholar]
- Huisman M., Oldehinkel A.J., de Winter A., Minderaa R.B., de Bildt A., Huizink A.C., Verhulst F.C., Ormel J. (2008) Cohort profile: the Dutch ‘TRacking Adolescents' Individual Lives' Survey’; TRAILS. International Journal of Epidemiology, 37(6), 1227–1235, DOI: 10.1093/ije/dym273 [DOI] [PubMed] [Google Scholar]
- Knappe S., Beesdo‐Baum K., Fehm L., Stein M.B., Lieb R., Wittchen H.U. (2011) Social fear and social phobia types among community youth: differential clinical features and vulnerability factors. Journal of Psychiatric Research, 45(1), 111–120, DOI: 10.1016/j.jpsychires.2010.05.002 [DOI] [PubMed] [Google Scholar]
- Little T.D., Card N.A., Slegers D.W., Ledford E.C. (2007) Representing contextual effects in multi‐group MACS models In Little T.D. (ed.) Longitudinal structural equation modeling; New York: Guilford: press. [Google Scholar]
- Meredith W. (1993) Measurement invariance, factor analysis and factorial invariance. Psychometrika, 58(4), 525–543, DOI: 10.1007/bf02294825 [DOI] [Google Scholar]
- Millsap R.E., Yun‐Tein J. (2004) Assessing factorial invariance in ordered‐categorical measures. Multivariate Behavioral Research, 39(3), 479–515, DOI: 10.1207/s15327906mbr3903_4 [DOI] [Google Scholar]
- de Moor M.H.M., Distel M.A., Trull T.J., Boomsma D.I. (2009) Assessment of borderline personality features in population samples: is the Personality Assessment Inventory‐Borderline Features scale measurement invariant across sex and age? Psychological Assessment, 21(1), 125–130, DOI: 10.1037/a0014502 [DOI] [PubMed] [Google Scholar]
- Múthen L.K., Múthen B.O. (1998–2007) MPlus User's Guide, Fourth Edition. Los Angeles CA: Múthen & Múthen. [Google Scholar]
- de Ross R.L., Gullone E. (2002) The Revised Child Anxiety and Depression Scale: A psychometric investigation with Australian youth. Behaviour Change, 19(2), 90–101, DOI: 10.1375/bech.19.2.90 [DOI] [Google Scholar]
- Rueter M.A., Scaramella L., Wallace L.E., Conger R.D. (1999) First onset of depressive or anxiety disorders predicted by the longitudinal course of internalizing symptoms and parent–adolescent disagreements. Archives of General Psychiatry, 56(8), 726–732, DOI: 10.1001/archpsyc.56.8.726 [DOI] [PubMed] [Google Scholar]
- Rusticus S.A., Hubley A.M., Zumbo B.D. (2008) Measurement invariance of the appearance schemas inventory‐revised and the body image quality of life inventory across age and gender. Assessment, 15(1), 60–71, DOI: 10.1177/1073191107306805 [DOI] [PubMed] [Google Scholar]
- Schermelleh‐Engel K., Moosbrugger H., Müller H. (2003) Evaluating the fit of structural equation models: Test of significance and descriptive goodness‐of‐fit measures. Methods in Psychology Research, 8(2), 23–74. [Google Scholar]
- Scholing A. (2000) Nederlandse Vertaling van de SCAS (SCAS‐NL – kinderversie). Amsterdam: Universiteit van Amsterdam. [Google Scholar]
- Spence S.H. (1997) Structure of anxiety symptoms among children: a confirmatory factor‐analytic study. Journal of Abnormal Psychology, 106(2), 280–297, DOI: 10.1037//0021-843x.106.2.280 [DOI] [PubMed] [Google Scholar]
- Spence S.H. (1998) A measure of anxiety symptoms among children. Behaviour Research and Therapy, 36(5), 545–566, DOI: 10.1016/s0005-7967(98)00034-5 [DOI] [PubMed] [Google Scholar]
- Steiger J.H. (1990) Structural model evaluation and modification: An interval estimation approach. Multivariate Behavioral Research, 25(2), 173–180, DOI: 10.1207/s15327906mbr2502_4 [DOI] [PubMed] [Google Scholar]
- Szabo A.N., Mullen S.P., White S.M., Wojcicki T.R., Mailey E.L., Gothe N., Olson E.A., Fanning J., Kramer A.F., McAuley E. (2011) Longitudinal invariance and construct validity of the Abbreviated Late‐Life Function and Disability Instrument in healthy older adults. Archives of Physical Medicine and Rehabilitation, 92(5), 785–791, DOI: 10.1016/j.apmr.2010.12.033 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tucker L.R., Lewis C. (1973) A reliability coefficient for maximum likelihood factor analysis. Psychometrika, 38(1), 1–10. [Google Scholar]
- Widaman K.F., Reise S.P. (1997) Exploring the measurement invariance of psychological instruments: applications in the substance abuse domain In Bryant K., Windle M., West S.G. (eds) The Science of Prevention: Methodological Advances from Alcohol and Substance Abuse Research, pp. 281–323. Washington, DC: American Psychological Association. [Google Scholar]
- de Winter A.F., Oldehinkel A.J., Veenstra R., Brunnekreef J.A., Verhulst F.C., Ormel J. (2005) Evaluation of non‐response bias in mental health determinants and outcomes in a large sample of pre‐adolescents. European Journal of Epidemiology, 20(2), 173–181, DOI: 10.1007/s10654-004-4948-6 [DOI] [PubMed] [Google Scholar]
- ter Wolbeek M., van Doornen L.J.P., Kavelaars A., Tersteeg‐Kamperman M.D.J., Heijnen C.J. (2011) Fatigue, depressive symptoms, and anxiety from adolescence up to young adulthood: a longitudinal study. Brain, Behavior, and Immunity, 25(6), 1249–1255, DOI: 10.1016/j.bbi.2011.04.015 [DOI] [PubMed] [Google Scholar]