

Abstract
While injuries of the upper extremity are widely discussed in rock climbers, reports about the lower extremity are rare. Nevertheless almost 50 percent of acute injuries involve the leg and feet. Acute injuries are either caused by ground falls or rock hit trauma during a fall. Most frequently strains, contusions and fractures of the calcaneus and talus. More rare injuries, as e.g., osteochondral lesions of the talus demand a highly specialized care and case presentations with combined iliac crest graft and matrix associated autologous chondrocyte transplantation are given in this review. The chronic use of tight climbing shoes leads to overstrain injuries also. As the tight fit of the shoes changes the biomechanics of the foot an increased stress load is applied to the fore-foot. Thus chronic conditions as subungual hematoma, callosity and pain resolve. Also a high incidence of hallux valgus and hallux rigidus is described.
Keywords: Rock climbing, Sport climbing, Feet injuries, Hallux valgus, Overstrain injuries
Core tip: While injuries of the upper extremity are widely discussed in rock climbers, reports about the lower extremity are rare. Nevertheless almost 50 percent of acute injuries involve the leg and feet and most frequently are strains, contusions and fractures of the calcaneus and talus. The chronic use of tight climbing shoes leads to overstrain injuries also. As the tight fit of the shoes changes the biomechanics of the foot an increased stress load is applied to the fore-foot. Thus chronic conditions as subungual hematoma, callosity and pain resolve. Also a high incidence of hallux valgus and hallux rigidus is described.
INTRODUCTION
Rock climbing is a fast growing sport with followers around the globe[1]. While alpine climbing has its inherent dangers, sport, indoor and competition climbing showed a minor injury risk[1-15]. Also, most of the injuries occurring are of minor severity and often due to overuse[1,3,16]. In rock climbing mostly only the hands and feet are used to be holding onto the rock or artificial climbing wall; thus placing extreme forces on the distal extremities[9,13,17-59]. However in falls frequently the feet are getting the most load while landing[21].
INJURY DISTRIBUTION
The literature data on injury distribution between the upper and lower extremity is inconsistent[1]. Many scientific climbing papers only present case studies or common hand injuries[17,19,30,41,48,54,55,60-63] and are therefore not suitable for injury distribution analysis. So far, most research indicates that the upper extremity to be the most injured body region in non-alpine rock-climbing[2,3,5,6,10,14,15,40,60,64-72]. Schöffl et al[61] analysed 604 injured climbers (sport climbing, indoor climbing) and reported 247 of 604 (40.9%) injuries involved the hand, 9.1% the foot. In contradiction two studies that analysed climbing injuries treated in American hospitals or emergency rooms[5,73] reported that most climbing injuries involved the lower extremities and resulted from big swings into the wall or big falls[5,73]. Bowie et al[5] found most fractures (63%) in rock climbers on the lower extremity, primarily the ankle, tibia or fibula. The authors suggest that these findings may be partially explained by the minor nature of many rock climbing related injuries recalled by participants in the other surveys. Backe et al[6] reported that out of all acute climbing injuries 50% involved the foot, toe and ankle. Largiadèr et al[74] found in an inquiry among 332 climbers, that 34.4% suffered from injuries and that 34.6% of these were feet injuries. In another recent study on rock climbing injuries, traumatic injuries involved the lower extremities (foot, toe and ankle) in 50% while upper extremities accounted for 36% of the injuries[6]. Killian et al[75] found a significant correlation between the incidence of ankle sprains and bouldering as well as in between ankle sprains and sport climbing. Neuhof et al[2] in contrast found a even injury distribution between the upper (42.6%) and lower extremities (41.3%) (Figure 1). In summary, most of the studies found that overuse injuries are mainly affecting the upper extremity, while acute traumatic injuries are more frequently located on the lower extremity[1,76]. Also, besides the acute lower limb injuries the incidence of chronic feet problems increases in the higher levels of sport climbing[23,25,75,77,78]. Scientific research in rock climbing up to date focused extensively on upper limb injuries. This may be based on the fact that various upper limb injuries as e.g., pulley injuries[44,60,79], lumbrical shift syndrome[32], extensor hood syndrome[80] or epiphyseal fatigue fractures in young climbers[63] are new pathologies and rather specific for the sport. Studies and reports on lower limb injuries and overuse syndromes are rare[23,25,33,75,77,78]. Nevertheless as e.g., the study by Neuhof et al[2] showed, that the mostly injured region were the feet (19.2%), these injuries are of a high importance and need to be examined further[1] (Table 1)[61].
Figure 1.
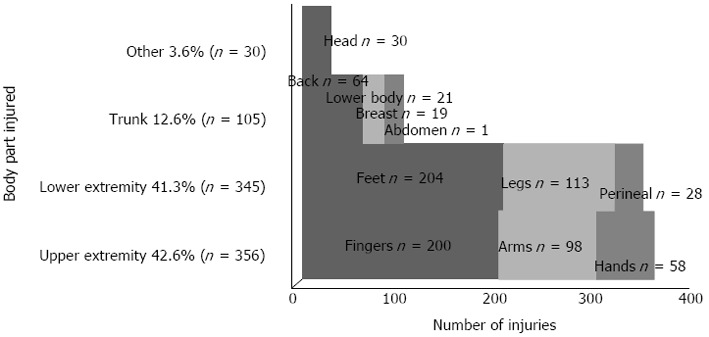
Distribution of Injuries by body part.
Table 1.
The ten most frequent localization of climbing specific diagnoses 1/98-12/01[61] n (%)
| Acute and chronic injuries | n = 604 |
| Fingers | 247 (41.0) |
| Forearm/elbow | 81 (13.4) |
| Foot | 55 (9.1) |
| Hand | 47 (7.8) |
| Spine/torso | 43 (7.1) |
| Skin | 42 (6.9) |
| Shoulder | 30 (5.0) |
| Knee | 30 (3.6) |
| Others | 37 (6.1) |
| Polytraumatic | 5 (0.8) |
INJURIES OR OVERSTRAIN
Climbing shoes
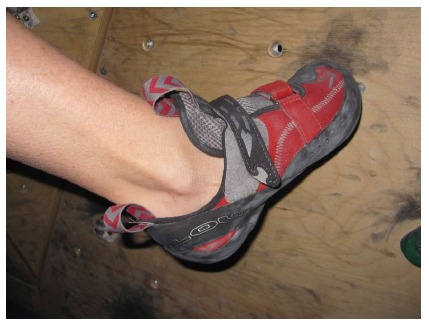
Up until about 40 years ago, most alpine climbing and rock climbing was done in heavy mountain boots. An extra pair of socks was often worn, and the foot was held in a leather cast that protected it but also took away any sensitivity and the need for strength in the toes. Leather boots were replaced by the legendary E.B. in the 1970 s, and a new generation of rock shoes with sticky rubber was just around the corner. Shoes today have become specialized into the type of rock climbing one wants to do. Attributes like downturn, the concave shape that places pressure on the toes, and asymmetry, concentrating the pressure on the big toe, are basic elements of modern climbing shoes[21,75] (Figure 2). These special climbing shoes should facilitate the ability to stand on friction with straight toes and on edges with bent toes with precision and proper contact[33,75,77,81]. The majority of climbing foot injuries result from wearing climbing shoes unnaturally shaped or too small in size[33,75,77,81]. The shoe seize reduction forces the foot to conform the shoe and changes the biomechanical position of the foot within the shoe. The foot shortens through supination and contraction of the digits[33,75,77,78]. In front pointing the proximal and mostly also the distal interphalangeal joints are flexed and the metatarsophalangeal joints are over extended (crimping toes)[78]. Lateral X rays within the climbing shoe show that the normal foot weight distribution onto the first and fifths metatarsal head and the heal is not given any more. The foot is front pointing onto the distal toe phalanges[75,77,78]. The plantar flexion of the metatarsal heads results in a tightening of the plantar fascia[33,35,75,77,78]. High ability climbers experience more foot deformities and injuries compared to climbers of lower ability due to the common practice of wearing climbing shoes sized smaller than normal street wear shoes (Figures 3 and 4A, B, C)[75,77,78]. Schöffl et al[78] reported about an average shoe seize difference between normal shoes and climbing shoes of 2.3 ± 0.73 continental seizes in high ability rock climbers [mean climbing level 9.7 (UIAA MedCom metric scale[82])]. Killian et al[75] reported about typically 1 to 2 seizes reduction (mean 1.699) in average climbers [mean climbing level 7.0 (UIAA MedCom metric scale[82])]. 80%-90% of the climbers reported[75,78] of suffering pain while using their climbing shoes, and that they accept to suffer this discomfort for improved performance[78]. Frequent problems are callosity, nail bed infections, pressure marks, neurologic complaints and subungual hematoma[33,75,77,78]. In the long term, using tight fit climbing shoes can lead to the development of a hallux valgus deformity[77,78]. van der Putten et al[77] even developed, based on their biomechanical analysis of climbers feet, a special climbing shoe sizing system, which includes an algorithm to accommodate differences between left and right foot.
Figure 2.
Modern climbing shoe.
Figure 3.
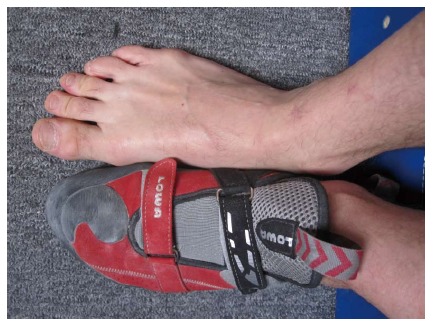
A standing climber’s barefoot and while wearing climbing shoes.
Figure 4.

X-ray. A: Climber’s bare foot while standing; B: Same subject’s foot in climbing shoe. Note “crimping” toes and hallux valgus position of the large toe; C: Lateral plane of the same foot in a climbing shoe-note that the forefoot does not rest on the head of the metacarpalia 1 and 5 as normal but on the crimping toes; D: Post surgery (Case 1); E: Subchondral bone cyst in a 42 year old female climber causing chronic pain within the climbing shoes; F: After removal of the cyst and iliac crest bone graft using the OATS®; G: Osseous integration after 3 mo.
For the further analysis acute injuries, mostly from falls and overuse (overstrain) injuries, due to the tight fitting climbing shoes must be distinguished.
Injuries to the feet
The most frequent inciting factor for injury to the lower extremity in rock climbing is a fall[1-3,5,83]. For further explaining the different ways injuries occur while climbing, a differentiation between two different types of falls is necessary: a wall-collision fall and a ground fall[21].
A wall-collision fall is one where the climber impacts the wall in a more or less vertical plane, while a ground fall is one where the climber impacts in more or less the horizontal plane[21]. In a wall-collision fall the climbers takes a fall while lead climbing. When falling the tensioning of the rope pulls him to, or against the rock face. In accordance to fall height, belay technique and rope stretch the impact onto the rock face varies[21] (Figure 5). Contrary to how it might appear, short falls, with a high impact factor (generally not far from the ground or the belay) can be the most dangerous. In these types of falls the climber is actually pulled back into the rock and the angle that he/she puts the foot (or arm) out at on impact creates a lot of stress on that particular spot. Also, auto-breaking devices, like the Gri-Gri® (Petzl, France) and Sirius® (TRE, Germany), can increase the fall factor[21]. Typical injuries are contusions or compound fractures[21]. A ground fall from as little as 8 feet high can lead to serious fractures of the calcaneus, talus and ankle joint (Figures 6, 7)[21]. Other ground fall injuries are distortions and ligamental injuries (ankle sprains)[6,21,73]. These injuries are on the increase with the growth in bouldering as a sport, but they are also fairly common with sport climbers who fall before reaching the first bolt or are dropped by their belayer[21]. One typical injury mechanism in indoor climbing, especially bouldering (ropeless climbing on low height with mattress belay) is a fall onto the mattresses and the foot getting stuck in the intermediate section between 2 mattresses[1,3,14,76,84,85]. As this injury mechanism was quite frequent 10 years ago it was addressed by the Medical Commission of the UIAA[85] (International Mountaineering Association) and nowadays the International Federation of Sport Climbing (IFSC) has a rule that these intersections must be closed in competitions (Figure 8)[76].
Figure 5.
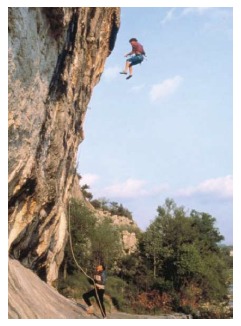
Wall-collision fall.
Figure 6.
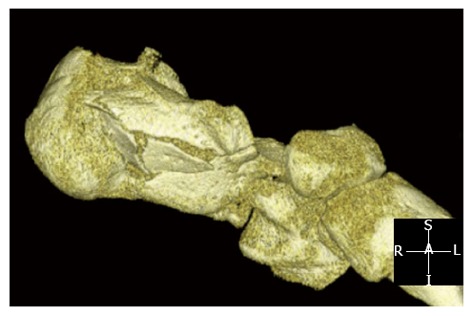
Calcaneus fracture after a ground fall (Computed tomography scan).
Figure 7.
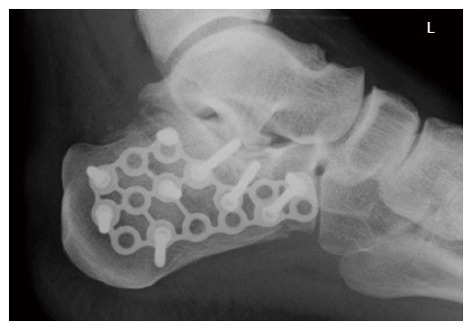
The same patient as above after surgery.
Figure 8.
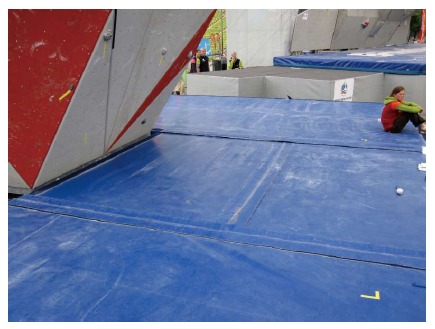
Closed mattress intersections at the International Federation of Sport Climbing Bouldering World Cup Munich 2011.
Typical feet injuries in rock climbers[1,2,7,8,10,21,73,78,84]: (1) Contusion; (2) Calcaneus fracture; (3) Talus fracture; (4) Ankle fracture; and (5) Ankle sprain with lateral ligament injury.
Neuhof et al[2] evaluated 1962 sport climbers and their injuries over a 5 year period and found a total of 699 injuries. 345 of these (41.3%) were on the lower extremity, 29.2% were on the feet. Most of the fractures (48.6%) and most of all contusions (42.5%) were on the feet, while most ligamental injuries and tendon injuries were on the fingers. Ankle sprains are frequent in boulderers and sport climbers with a significant correlation[75] to these climbing activities. Killian et al[75] reported about an incidence of 0.23 for ankle sprains and of 0.03 for feet fractures in rock climbers. Nelsen et al[73] found that ankle injuries accounted for 19.2% of all climbing injuries. Backe et al[6] reported that out of all acute climbing injuries 50% involved the foot, toe and ankle. The most common type was a ligament injury, followed by contusions and lacerations. Gerdes et al[10] also reported that sprains and strains were most common on the fingers (31.9%) and the ankle (23%). Fractures were most common on the foot (24.6%) and the ankle (22.1%). Especially in the older athletes also short falls can lead to feet and ankle fractures caused by the increased brittleness of the bone that occurs with aging[86].
These typical injuries undergo standard orthopedic trauma guidelines and in case of displaced fractures mainly operative reconstruction (open reduction and internal fixation). Considering that climbers are mostly young and highly active patients we also favor a surgical repair in most talus and calcaneus fractures (Figures 6, 7) to achieve an optimal outcome. While these standard guidelines are known and presented in the specific literature some rare injuries in climbers should be specifically addressed in this review. In particular we will focus on posttraumatic ostechondritis dissecans of the talus after climbing falls and the management of peroneal tendon dislocations in elite climbers.
Management of large osteochondritis dissecans defects of the talus: matrix associated autologous chondrocyte transplantation with combined iliac crest bone graft (Case 1)
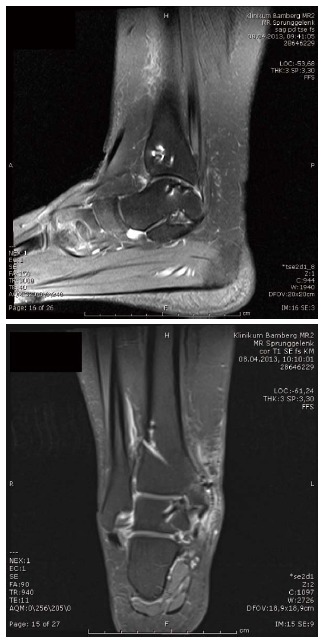
Posttraumatic osteochondritis dissecans is a well-known pathology after ankle sprains and dislocation[87-91]. As the initial X-ray often does not show the injury they are often detected only secondarily, if the patient still complains of ankle pain after more than 6 wk. In persistent ankle pain and a plain standard radiograph an MRI is indicated. The following case presentation is one out of several climbers with a similar pathology.
The patient was a female climber, 20 years old, who had an ankle sprain due to a ground fall from bouldering. 1.5 years after the trauma an osteochondritis dissecans was diagnosed in another hospital and an arthroscopic drill-hole procedure was performed. One year later she was still complaining about ankle pain and presented in our outpatient clinic. X-ray, MRI and CT scan revealed an osteochondritis dissecans with a large osseous defect at the medial talus shoulder (Figure 9).
Figure 9.

Computed tomography scan of a 20 year old female climber with osteochondritis dissecans of the medial talus shoulder.
While the management of chondral lesions of the talus with autologous chondrocyte transplantation is a standard procedure with positive results in over 90%[88,89,91], large osseous defects in combination with osteochondral lesions are more difficult to manage[87]. Mostly these lesions are treated with osteochondral autografts (OATS)[90,92]. Nevertheless one problem with OATS is that the talus shoulder demands a cartilage cover on two plains, on the horizontal surface and on its respective medial or lateral side. Based on our previous work on matrix associated autologous chondrocyte transplantation (MACT) with combined iliac crest bone graft in large defects of the talus[87] we performed a similar procedure in this young female climber. A 4th degree cartilage defect was already confirmed arthroscopically in addition to the CT and MRI images in another hospital. A drilling of the defect during the prior arthroscopy did not help to restore blood flow into the osteochondritic area and thus failed. Therefore a osteograft with cartilage transplant was necessary. After arthroscopic harvesting of two osteochondral cylinders of the ipsi-lateral knee we performed secondary a medial osteotomy with debridement and resection of all dead tissue of the ankle joint. Then the medial talus shoulder was reconstructed with a bicortical iliac crest implant, which was secured through countersink mini titanium screws. Following the bone transplant was covered with a MACT (NOVOCART®, TETEC Tissue Engineering Technologies, Braun Aesculap, Germany) (Figures 4D and 10).
Figure 10.
Medial talus shoulder reconstruction with iliac crest implant and associated autologous chondrocyte transplantation
The postsurgical procedure included 6 wk of cast immobilization followed by a step-wise load increase. Full weight bearing was allowed after 12 wk. MRI controls were performed after removal of the osteotomy screws after 3 and 6 mo. Standard MRI after 3 mo showed an osseous integration of the iliac crest graft and a contrast fluid enhancement of the MACT. After 6 mo morphological und biochemical magnetic resonance imaging showed the complete osteointegration of the bone graft and cartilage repair of the talus[93,94](Figure 11).
Figure 11.
Magnetic resonance imaging 3 mo after the procedure. The bone graft is integrated, the cartilage graft intact and osteotomy closed.
Pain decreased on a visual analog scale from 8 to 2. She could climb again at the same level as before the injury and American Orthopaedic Foot and Ankle Society Ankle-Hindfoot score[95] raised from 63 to 84 points.
Peroneal tendon dislocations in climbers (Case 2)
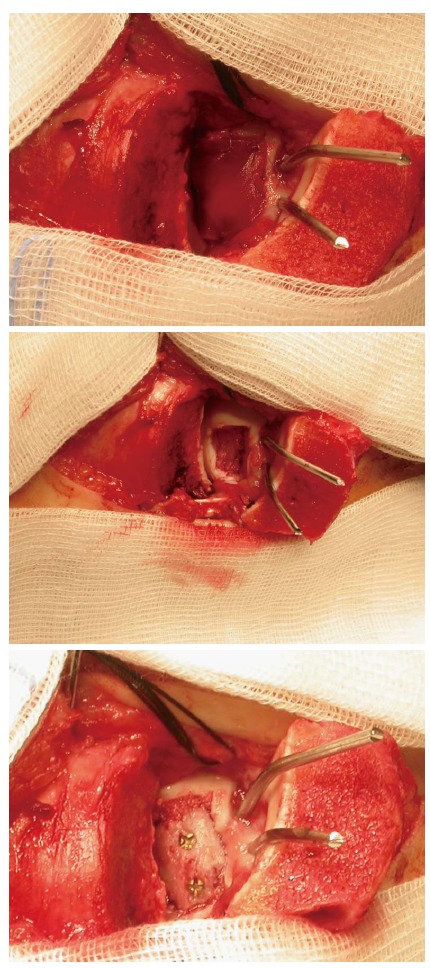
Acute peroneal tendon dislocations are rare and mostly seen in skiers[96-99]. Nevertheless evaluating 911 climbing injuries over 4 years (2009-2012)[100] we had 3 climbers with this pathology. All reported about a snap of the peroneal retinaculum while having the foot in a plantar flexion with maximum inversion and applying high tension onto the large toe while climbing (Figure 12). These acute peroneal tendon dislocations can be seen similar to pulley injuries in the fingers[60] in climbers. With the high strength impact onto the superior peroneal retinaculum, which serves analogous to the hand as a pulley, the retinaculum, which is also enhanced by the calcaneofibular ligament, fails and the peroneal tendons dislocate. In all 3 cases the peroneal tendon grove of the fibula was of normal shape, therefore no anatomical predisposition was given. In general literature recommend a non-surgical approach if the dislocation is treated immediate and the tendons stay in their normal position within the cast[96,97]. Nevertheless in active patients, especially in “feet depending” sports a surgical repair is recommended[96,97]. Surgical techniques are mostly described for chronic subluxation and contain a peroneal groove deepening, a tenoplasty or a bone block transfer[96-99,101]. Only in acute cases a direct repair of the ruptured structures may be possible, sometimes in combination with a periostal flap[96,101]. We performed a surgical repair in all cases (Figure 13), in two cases a direct repair was possible and in one case an additional periostal flap was necessary. Afterwards a 6 wk cast immobilisation was performed. Climbing activity was allowed 8 wk after injury. All athletes regained a full climbing ability with no reoccurance or consisting problems.
Figure 12.
Typical climbers foot position which transfers a high load onto the peroneal tendons retinaculum.
Figure 13.

Peroneal tendon dislocation through climbing.
OVERUSE INJURIES AND CHRONIC CONDITIONS
As described above rock climbing shoes are worn with a tight fit, roughly two seizes smaller than normal shoes[75,77,78]. This tight fit increases, due to the biomechanical chances of force distribution in the foot, the injury incidence in falls onto the foot or against the wall[75]. In addition to these acute conditions these malpositioning of the foot within the climbing shoe cause chronic conditions and complaints. Schöffl et al[78] evaluated 30 high level male sport climbers for chronic foot deformations. Every climber was at least climbing on a UIAA 9.0 level [mean climbing level 9.7 (UIAA MedCom metric scale[82])] and climbing more than 5 years (mean climbing years 12.8 years). Training hours per wk were a mean 12.3 h, which refers to roughly 10 h per wk within the small climbing shoes. The shoe seize difference between climbing shoes to standard shoes was in mean 2.3 seizes. 87% of the climbers were willingly accepting pain within the climbing shoes to achieve a better performance. Also 87% reported about chronic feet problems and pain within the climbing shoes. All climbers had callosity and pressure marks dorsally on their toes (100% dig.ped.1, 95% dig.ped.2, 85% dig.ped.3, 43% dig.ped.4, 8% dig.ped.5) (Figure 14A). Further conditions were: dead toe nails, broken and missing toe nails, nail bed infections, dermatomycosis, blisters, claw toes, subungual hematoma (Figure 14B) and hallux valgus (Figure 14C). For their incidence and distribution see Figure 15[78].
Figure 14.

Feet injuries. A: Pressure marks on the toes due to tight climbing shoes; B: Subungual hematoma caused by tight climbing shoes; C: Hallux valgus in a 20+ year long climber.
Figure 15.
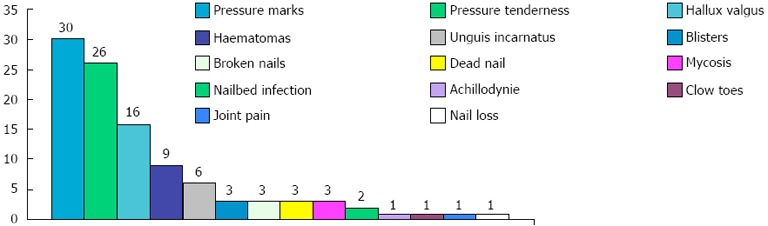
Chronic Feet Problems in Long time high ability rock climbers (n = 30)[78].
In comparison Largiadèr et al[74] reported only about 28% of climbers with feet nail dystrophy and feet deformities in 21%. Nevertheless their climber population was different, as most of their climber were only climbing in the 6th UIAA grade, thus having a shorter trainings time and less climbing years and therefore a reduced exposition to the very tight shoes in comparison to Schöffl et al[78]. Killian et al[75] surveyed 100 climbers through a questionnaire on feet conditions. 73 were male, 27 female, the mean climbing level was 5.109 US (7.0 UIAA[16]). 81% of the climber`s complaint about discomfort through the climbing shoes. Pain in the toes or hallux valgus was the most frequent complaint. They found a significant correlation between climbing ability and extent of shoe seize reduction, however no correlation between the extend of shoe seize reduction or skill level and the incidence of pain or discomfort. 65% of the climbers surveyed experienced either tingling or numbness a condition also frequently reported about by Peters[33] and Largiadèr et al[74]. These neurological complaints and neurinomas are known to be greatly exacerbated through constricting shoes[102]. van der Putten et al[77] also found frequently mycosis, splinter hemorrhage, nail fractures, hallux valgus, bunions, and callosity on their questioned 30 climber. Nevertheless as there paper focuses on the biomechanical development of a climbing shoe exact numbers of the distribution of these conditions were not given.
Schöffl et al[78] and Killian et al[75]also looked upon the long term effects of the wear of tight climbing shoes. Through radiographic analysis of a standing climber within a climbing shoe and barefoot Schöffl et al[78] demonstrate how the climbing shoes forces the foot into a hallux valgus position (Figures 4, 5). The hallux valgus angle increases from 14° barefoot to 21° within the shoe.[78] They found in 53% of the long time high level climbers a hallux valgus, in 20% bilateral (hallux valgus defined as a 20° difference between the axis of the first metatarsal and the axis of the proximal phalanx of the toe). The general incidence in a group of male adults (age: 17-44) is only 4.5%[103]. Killian et al[75] found an average incidence of a hallux valgus of 34% in climbers of all difficulty levels, but of 53% of the group of climbers in the 5.12 range (UIAA metric 8.3-9.0). Over the recent years we saw an increasing number of climbers with a hallux rigidus condition, even requiring a surgical therapy (cheilectomy or fusion)[21]. Rock climbing is still possible afterwards, nevertheless the risk of osteoarthritis in the adjunct joints increases. Sometimes also enchondroma (preexisting and not as a result of climbing activities) or bone cysts can cause chronic pain within the climbing shoes. Figure 4E, F, G (case 3) show a 42 year old female climber with chronic feet problems, revealing a large subchondral cyst of the big toe. The cyst was resected and the bone defect filled through a cortical-spongious bone graft from the iliac crest. To guarantee a press fit we used the OATS® (osteoarticular transfer system, Arthrex® Inc., Naples, FL, United States) instruments to harvest the graft and to shape the implant site as well. Postoperatively a cast was applied. Complete osseous integration was achieved and she could continue climbing without pain after 3 mo.
CONCLUSION
Considering the known high incidence of feet problems of rock climbers it is astonishing that only little scientific work has been done so far in this topic. Most climbing studies focus on the upper extremity, mainly the hand and fingers. With numbers of up to 90% of examined and questioned climbers with chronic feet conditions more work needs to be done in this respect. To reduce these complaints climbers need to be advised not to wear their shoes too tight and have an additional loose fit training shoe[21]. Also the industry producing climbing shoes must be involved, and new fitting strategies with less stretching outer materials and biomechanical adjusted constructions impaired. New shoes should have a inner lining to reduce bunions and callosity, while still guaranteeing a good perception of the rock. While high level climbing athletes may be in the need of a tight fit shoe the vast number of recreational climbers need the opposite. A comfortable fitting shoe which supports the foot and does not hurt.
Footnotes
P- Reviewer van den Bekerom MPJ S- Editor Wen LL L- Editor A E- Editor Liu XM
References
- 1.Schöffl V, Morrison A, Schöffl I, Küpper T. The epidemiology of injury in mountaineering, rock and ice climbing. Med Sport Sci. 2012;58:17–43. doi: 10.1159/000338575. [DOI] [PubMed] [Google Scholar]
- 2.Neuhof A, Hennig FF, Schöffl I, Schöffl V. Injury risk evaluation in sport climbing. Int J Sports Med. 2011;32:794–800. doi: 10.1055/s-0031-1279723. [DOI] [PubMed] [Google Scholar]
- 3.Schöffl V, Morrison A, Schwarz U, Schöffl I, Küpper T. Evaluation of injury and fatality risk in rock and ice climbing. Sports Med. 2010;40:657–679. doi: 10.2165/11533690-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 4.Schöffl V, Schöffl I, Schwarz U, Hennig F, Küpper T. Injury-risk evaluation in water ice climbing. Med Sport. 2009;2:32–38. [Google Scholar]
- 5.Bowie WS, Hunt TK, Allen HA. Rock-climbing injuries in Yosemite National Park. West J Med. 1988;149:172–177. [PMC free article] [PubMed] [Google Scholar]
- 6.Backe S, Ericson L, Janson S, Timpka T. Rock climbing injury rates and associated risk factors in a general climbing population. Scand J Med Sci Sports. 2009;19:850–856. doi: 10.1111/j.1600-0838.2008.00851.x. [DOI] [PubMed] [Google Scholar]
- 7.Josephsen G, Shinneman S, Tamayo-Sarver J, Josephsen K, Boulware D, Hunt M, Pham H. Injuries in bouldering: a prospective study. Wilderness Environ Med. 2007;18:271–280. doi: 10.1580/06-WEME-OR-071R1.1. [DOI] [PubMed] [Google Scholar]
- 8.Jones G, Asghar A, Llewellyn DJ. The epidemiology of rock-climbing injuries. Br J Sports Med. 2008;42:773–778. doi: 10.1136/bjsm.2007.037978. [DOI] [PubMed] [Google Scholar]
- 9.Smith LO. Alpine climbing: injuries and illness. Phys Med Rehabil Clin N Am. 2006;17:633–644. doi: 10.1016/j.pmr.2006.05.003. [DOI] [PubMed] [Google Scholar]
- 10.Gerdes EM, Hafner JW, Aldag JC. Injury patterns and safety practices of rock climbers. J Trauma. 2006;61:1517–1525. doi: 10.1097/01.ta.0000209402.40864.b2. [DOI] [PubMed] [Google Scholar]
- 11.Locker T, Chan D, Cross S. Factors predicting serious injury in rock-climbing and non-rock-climbing falls. J Trauma. 2004;57:1321–1323. doi: 10.1097/01.ta.0000130609.23499.2f. [DOI] [PubMed] [Google Scholar]
- 12.Wright DM, Royle TJ, Marshall T. Indoor rock climbing: who gets injured? Br J Sports Med. 2001;35:181–185. doi: 10.1136/bjsm.35.3.181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rohrbough JT, Mudge MK, Schilling RC. Overuse injuries in the elite rock climber. Med Sci Sports Exerc. 2000;32:1369–1372. doi: 10.1097/00005768-200008000-00002. [DOI] [PubMed] [Google Scholar]
- 14.Schöffl V, Winkelmann HP. [Accident statistics at “indoor climbing walls”] Sportverletz Sportschaden. 1999;13:14–16. doi: 10.1055/s-2007-993308. [DOI] [PubMed] [Google Scholar]
- 15.Paige TE, Fiore DC, Houston JD. Injury in traditional and sport rock climbing. Wilderness Environ Med. 1998;9:2–7. doi: 10.1580/1080-6032(1998)009[0002:iitasr]2.3.co;2. [DOI] [PubMed] [Google Scholar]
- 16.Schöffl V, Morrison A, Hefti U, Ullrich S, Küpper T. The UIAA Medical Commission injury classification for mountaineering and climbing sports. Wilderness Environ Med. 2011;22:46–51. doi: 10.1016/j.wem.2010.11.008. [DOI] [PubMed] [Google Scholar]
- 17.Holtzhausen LM, Noakes TD. Elbow, forearm, wrist, and hand injuries among sport rock climbers. Clin J Sport Med. 1996;6:196–203. doi: 10.1097/00042752-199607000-00010. [DOI] [PubMed] [Google Scholar]
- 18.Bollen SR. Upper limb injuries in elite rock climbers. J R Coll Surg Edinb. 1990;35:S18–S20. [PubMed] [Google Scholar]
- 19.Bollen SR, Gunson CK. Hand injuries in competition climbers. Br J Sports Med. 1990;24:16–18. doi: 10.1136/bjsm.24.1.16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bollen SR. Soft tissue injury in extreme rock climbers. Br J Sports Med. 1988;22:145–147. doi: 10.1136/bjsm.22.4.145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hochholzer T, Schöffl V. One move too many. 2nd ed. Ebenhausen: Lochner Verlag; 2006. [Google Scholar]
- 22.Schöffl VR, Einwag F, Strecker W, Schöffl I. Strength measurement and clinical outcome after pulley ruptures in climbers. Med Sci Sports Exerc. 2006;38:637–643. doi: 10.1249/01.mss.0000210199.87328.6a. [DOI] [PubMed] [Google Scholar]
- 23.Morrison AB, Schöffl VR. Physiological responses to rock climbing in young climbers. Br J Sports Med. 2007;41:852–861; discussion 861. doi: 10.1136/bjsm.2007.034827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.MacLeod D, Sutherland DL, Buntin L, Whitaker A, Aitchison T, Watt I, Bradley J, Grant S. Physiological determinants of climbing-specific finger endurance and sport rock climbing performance. J Sports Sci. 2007;25:1433–1443. doi: 10.1080/02640410600944550. [DOI] [PubMed] [Google Scholar]
- 25.Morrison A, Schöffl V. Climbing shoes-is pain insane? In: BMC Medical., editor. London: BMC; 2009. pp. p. 1–4. [Google Scholar]
- 26.Schweizer A, Frank O, Ochsner PE, Jacob HA. Friction between human finger flexor tendons and pulleys at high loads. J Biomech. 2003;36:63–71. doi: 10.1016/s0021-9290(02)00242-7. [DOI] [PubMed] [Google Scholar]
- 27.Schweizer A. Biomechanical properties of the crimp grip position in rock climbers. J Biomech. 2001;34:217–223. doi: 10.1016/s0021-9290(00)00184-6. [DOI] [PubMed] [Google Scholar]
- 28.Schweizer A. Biomechanical effectiveness of taping the A2 pulley in rock climbers. J Hand Surg Br. 2000;25:102–107. doi: 10.1054/jhsb.1999.0335. [DOI] [PubMed] [Google Scholar]
- 29.Danion F. Grip force safety margin in rock climbers. Int J Sports Med. 2008;29:168–172. doi: 10.1055/s-2007-965112. [DOI] [PubMed] [Google Scholar]
- 30.Kubiak EN, Klugman JA, Bosco JA. Hand injuries in rock climbers. Bull NYU Hosp Jt Dis. 2006;64:172–177. [PubMed] [Google Scholar]
- 31.Moutet F, Forli A, Voulliaume D. Pulley rupture and reconstruction in rock climbers. Tech Hand Up Extrem Surg. 2004;8:149–155. doi: 10.1097/01.bth.0000128545.94060.99. [DOI] [PubMed] [Google Scholar]
- 32.Schweizer A. Lumbrical tears in rock climbers. J Hand Surg Br. 2003;28:187–189. doi: 10.1016/s0266-7681(02)00250-4. [DOI] [PubMed] [Google Scholar]
- 33.Peters P. Nerve compression syndromes in sport climbers. Int J Sports Med. 2001;22:611–617. doi: 10.1055/s-2001-18527. [DOI] [PubMed] [Google Scholar]
- 34.Vandeputte G, Dubert T. Closed traumatic rupture of the flexor pulleys of a long finger associated with avulsion of the flexor digitorum superficialis. J Hand Surg Br. 2001;26:266–268. doi: 10.1054/jhsb.2001.0559. [DOI] [PubMed] [Google Scholar]
- 35.Peters P. Orthopedic problems in sport climbing. Wilderness Environ Med. 2001;12:100–110. doi: 10.1580/1080-6032(2001)012[0100:opisc]2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 36.Carmeli E, Wertheim M. [Hand injuries in young and old wall climbers] Handverletzungen bei jugendlichen und erwachsenen Sportkletterern. D Z Sportmed. 2001;52:285–288. [Google Scholar]
- 37.Stelzle FD, Gaulrapp H, Pförringer W. Injuries and overuse syndromes due to rock climbing on artificial walls. Sportverletz Sportschaden. 2000;14:128–133. doi: 10.1055/s-2000-8951. [DOI] [PubMed] [Google Scholar]
- 38.Aronowitz ER, Leddy JP. Closed tendon injuries of the hand and wrist in athletes. Clin Sports Med. 1998;17:449–467. doi: 10.1016/s0278-5919(05)70096-x. [DOI] [PubMed] [Google Scholar]
- 39.Jebson PJ, Steyers CM. Hand injuries in rock climbing: reaching the right treatment. Phys Sportsmed. 1997;25:54–63. doi: 10.3810/psm.1997.05.1341. [DOI] [PubMed] [Google Scholar]
- 40.Rooks MD. Rock climbing injuries. Sports Med. 1997;23:261–270. doi: 10.2165/00007256-199723040-00005. [DOI] [PubMed] [Google Scholar]
- 41.Haas JC, Meyers MC. Rock climbing injuries. Sports Med. 1995;20:199–205. doi: 10.2165/00007256-199520030-00006. [DOI] [PubMed] [Google Scholar]
- 42.Shea KG, Shea OF, Meals RA. Manual demands and consequences of rock climbing. J Hand Surg Am. 1992;17:200–205. doi: 10.1016/0363-5023(92)90390-b. [DOI] [PubMed] [Google Scholar]
- 43.Maitland M. Injuries associated with rock climbing. J Orthop Sports Phys Ther. 1992;16:68–73. doi: 10.2519/jospt.1992.16.2.68. [DOI] [PubMed] [Google Scholar]
- 44.Toussaint B, Cartier JL, Herry JP, Allieu Y. Pathologie tendineuse et des poulies de la main chez le grimpeur. In: La main du sportif, Allieu Y (ed), editors. Expansion Scientific: France; 1985. pp. 154–160. [Google Scholar]
- 45.Schöffl I, Oppelt K, Jüngert J, Schweizer A, Neuhuber W, Schöffl V. The influence of the crimp and slope grip position on the finger pulley system. J Biomech. 2009;42:2183–2187. doi: 10.1016/j.jbiomech.2009.04.049. [DOI] [PubMed] [Google Scholar]
- 46.Schöffl I, Oppelt K, Jüngert J, Schweizer A, Bayer T, Neuhuber W, Schöffl V. The influence of concentric and eccentric loading on the finger pulley system. J Biomech. 2009;42:2124–2128. doi: 10.1016/j.jbiomech.2009.05.033. [DOI] [PubMed] [Google Scholar]
- 47.Schöffl V. [Hand Injuries in Rock Climbing] Handverletzungen beim Klettern. D Z Sportmed. 2008;59:85–90. [Google Scholar]
- 48.Schöffl VR, Hochholzer T, Imhoff AB, Schöffl I. Radiographic adaptations to the stress of high-level rock climbing in junior athletes: a 5-year longitudinal study of the German Junior National Team and a group of recreational climbers. Am J Sports Med. 2007;35:86–92. doi: 10.1177/0363546506293256. [DOI] [PubMed] [Google Scholar]
- 49.Arora R, Fritz D, Zimmermann R, Lutz M, Kamelger F, Klauser AS, Gabl M. Reconstruction of the digital flexor pulley system: a retrospective comparison of two methods of treatment. J Hand Surg Eur Vol. 2007;32:60–66. doi: 10.1016/j.jhsb.2006.09.019. [DOI] [PubMed] [Google Scholar]
- 50.Giles LV, Rhodes EC, Taunton JE. The physiology of rock climbing. Sports Med. 2006;36:529–545. doi: 10.2165/00007256-200636060-00006. [DOI] [PubMed] [Google Scholar]
- 51.Sylvester AD, Christensen AM, Kramer PA. Factors influencing osteological changes in the hands and fingers of rock climbers. J Anat. 2006;209:597–609. doi: 10.1111/j.1469-7580.2006.00640.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Klauser A, Gabl M, Smekal V, Nedden DZ. [High frequency sonography in the detection of finger injuries in sport climbing] Rontgenpraxis. 2005;56:13–19. doi: 10.1016/j.rontge.2005.06.001. [DOI] [PubMed] [Google Scholar]
- 53.Hernandez JD, Stern PJ. Complex injuries including flexor tendon disruption. Hand Clin. 2005;21:187–197. doi: 10.1016/j.hcl.2004.12.001. [DOI] [PubMed] [Google Scholar]
- 54.Schöffl V, Hochholzer T, Imhoff A. Radiographic changes in the hands and fingers of young, high-level climbers. Am J Sports Med. 2004;32:1688–1694. doi: 10.1177/0363546503262805. [DOI] [PubMed] [Google Scholar]
- 55.Logan AJ, Makwana N, Mason G, Dias J. Acute hand and wrist injuries in experienced rock climbers. Br J Sports Med. 2004;38:545–548. doi: 10.1136/bjsm.2002.003558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Watts PB. Physiology of difficult rock climbing. Eur J Appl Physiol. 2004;91:361–372. doi: 10.1007/s00421-003-1036-7. [DOI] [PubMed] [Google Scholar]
- 57.Roloff I. (Biomechanical modelling of the climbers hand: estimation of the mechanical constrains applied on the finger flexor tendon pulleys) Modélisation biomécanique de la main du grimpeur: estimation des contraintes mécaniques exercées sur les poulies digitalis (Master thesis) Grenoble: Université Joseph Fourier Grenoble 1;; 2004. [Google Scholar]
- 58.Quaine F, Vigouroux L. Maximal resultant four fingertip force and fatigue of the extrinsic muscles of the hand in different sport climbing finger grips. Int J Sports Med. 2004;25:634–637. doi: 10.1055/s-2004-821117. [DOI] [PubMed] [Google Scholar]
- 59.MacDermid JC, Lee A, Richards RS, Roth JH. Individual finger strength: are the ulnar digits “powerful”? J Hand Ther. 2004;17:364–367. doi: 10.1197/j.jht.2004.04.006. [DOI] [PubMed] [Google Scholar]
- 60.Schöffl V, Hochholzer T, Winkelmann HP, Strecker W. Pulley injuries in rock climbers. Wilderness Environ Med. 2003;14:94–100. doi: 10.1580/1080-6032(2003)014[0094:piirc]2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 61.Schöffl V, Hochholzer T, Winkelmann HP, Strecker W. (Differential diagnosis of finger pain in sport climbers) Differentialdiagnose von Fingerschmerzen bei Sportkletterern. D Z Sportmed. 2003;54:38–43. [Google Scholar]
- 62.Schöffl VR, Schöffl I. Injuries to the finger flexor pulley system in rock climbers: current concepts. J Hand Surg Am. 2006;31:647–654. doi: 10.1016/j.jhsa.2006.02.011. [DOI] [PubMed] [Google Scholar]
- 63.Hochholzer T, Schöffl VR. Epiphyseal fractures of the finger middle joints in young sport climbers. Wilderness Environ Med. 2005;16:139–142. doi: 10.1580/pr15-04.1. [DOI] [PubMed] [Google Scholar]
- 64.Rooks MD, Johnston RB, Ensor CD, McIntosh B, James S. Injury patterns in recreational rock climbers. Am J Sports Med. 1995;23:683–685. doi: 10.1177/036354659502300608. [DOI] [PubMed] [Google Scholar]
- 65.McIntosh SE, Campbell AD, Dow J, Grissom CK. Mountaineering fatalities on Denali. High Alt Med Biol. 2008;9:89–95. doi: 10.1089/ham.2008.1047. [DOI] [PubMed] [Google Scholar]
- 66.Hohlrieder M, Lutz M, Schubert H, Eschertzhuber S, Mair P. Pattern of injury after rock-climbing falls is not determined by harness type. Wilderness Environ Med. 2007;18:30–35. doi: 10.1580/06-weme-or-020r.1. [DOI] [PubMed] [Google Scholar]
- 67.Monasterio ME. Accident and fatality characteristics in a population of mountain climbers in New Zealand. N Z Med J. 2005;118:U1249. [PubMed] [Google Scholar]
- 68.Schussmann LC, Lutz LJ, Shaw RR, Bohn CR. The epidemiology of mountaineering and rock climbing accidents. J Wilderness Med. 1990;1:235–248. [Google Scholar]
- 69.Krueger DW, Hutcherson R. Suicide attempts by rock-climbing falls. Suicide Life Threat Behav. 1978;8:41–45. [PubMed] [Google Scholar]
- 70.Rettig A. [Mountain climbing accidents--measures and problems in first aid] Osterr Schwesternztg. 1973;26:174–177. [PubMed] [Google Scholar]
- 71.Brice DE, Ellis FR, Keaney NP, Proctor EA, Smith RB. Cardiorespiratory response to dangling on a rope in simulated rock-climbing accident. J Physiol. 1973;230:35P–36P. [PubMed] [Google Scholar]
- 72.Patscheider H. (Morphologic findings in fatal mountain-climbing accidents) Schweiz Z Sportmed. 1971;19:7–27. [PubMed] [Google Scholar]
- 73.Nelson NG, McKenzie LB. Rock climbing injuries treated in emergency departments in the U.S., 1990-2007. Am J Prev Med. 2009;37:195–200. doi: 10.1016/j.amepre.2009.04.025. [DOI] [PubMed] [Google Scholar]
- 74.Largiadèr U, Oelz O. [An analysis of overstrain injuries in rock climbing] Schweiz Z Sportmed. 1993;41:107–114. [PubMed] [Google Scholar]
- 75.Killian RB, Nishimoto GS, Page JC. Foot and ankle injuries related to rock climbing. The role of footwear. J Am Podiatr Med Assoc. 1998;88:365–374. doi: 10.7547/87507315-88-8-365. [DOI] [PubMed] [Google Scholar]
- 76.Schöffl V, Schöffl I. Competition Climbing. Sportortho Sporttrauma. 2012;28:22–28. [Google Scholar]
- 77.van der Putten EP, Snijder CJ. Shoe design for prevention of injuries in sport climbing. Appl Ergon. 2001;32:379–387. doi: 10.1016/s0003-6870(01)00004-7. [DOI] [PubMed] [Google Scholar]
- 78.Schöffl V, Winkelmann HP. [Footdeformations in sportclimbers] Fußdeformitäten bei Sportkletterern. 1. D Z Sportmed. 1999;50:73–76. [Google Scholar]
- 79.Bollen SR. Injury to the A2 pulley in rock climbers. J Hand Surg Br. 1990;15:268–270. doi: 10.1016/0266-7681_90_90135-q. [DOI] [PubMed] [Google Scholar]
- 80.Schöffl V, Hochholzer T, Schöffl I. Extensor hood syndrome--osteophytic irritation of digital extensor tendons in rock climbers. Wilderness Environ Med. 2010;21:253–256. doi: 10.1016/j.wem.2010.04.007. [DOI] [PubMed] [Google Scholar]
- 81.Schöffl V, Winkelmann HP. Footdeformations in Sportclimbers. ö. J Sportmed. 1999:58. [Google Scholar]
- 82.Schöffl V, Morrison AB, Hefti U, Schwarz U, Küpper T. The UIAA Medical Commission Injury Classification for Mountaineering and Climbing Sports. ed. In: No.17. 10.05; 2010. pp. Official Standards of the Union Internationale des Associations d’Alpinisme (UIAA), 2010: 1–8. [DOI] [PubMed] [Google Scholar]
- 83.Mosimann U. Notfölle beim Eisklettern. Bergundsteigen. 2006:70–73. [Google Scholar]
- 84.Schöffl VR, Kuepper T. Injuries at the 2005 World Championships in Rock Climbing. Wilderness Environ Med. 2006;17:187–190. doi: 10.1580/pr26-05. [DOI] [PubMed] [Google Scholar]
- 85.Schlegel C, Schöffl V. Statement Competition Climbing. Available from: http://www.uiaa.ch [10/2000 2000]
- 86.Hartsock LA, Feagin JA, Ogilvie BC. Climbing and the older athlete. Clin Sports Med. 1991;10:257–267. [PubMed] [Google Scholar]
- 87.Dickschas J, Welsch G, Strecker W, Schöffl V. Matrix-associated autologous chondrocyte transplantation combined with iliac crest bone graft for reconstruction of talus necrosis due to villonodular synovitis. J Foot Ankle Surg. 2012;51:87–90. doi: 10.1053/j.jfas.2011.09.004. [DOI] [PubMed] [Google Scholar]
- 88.Koulalis D, Schultz W, Heyden M. Autologous chondrocyte transplantation for osteochondritis dissecans of the talus. Clin Orthop Relat Res. 2002;(395):186–192. doi: 10.1097/00003086-200202000-00021. [DOI] [PubMed] [Google Scholar]
- 89.Aurich M, Venbrocks RA, Fuhrmann RA. Autologous chondrocyte transplantation for osteochondritis dissecans of the talus. Der Orthopade. 2008;37:90–95. doi: 10.1007/s00132-008-1210-z. [DOI] [PubMed] [Google Scholar]
- 90.Lin JS, Andersen LB, Juliano PJ. Effectiveness of composite bone graft substitute plugs in the treatment of chondral and osteochondral lesions of the talus. J Foot Ankle Surg. 2010;49:224–231. doi: 10.1053/j.jfas.2010.02.008. [DOI] [PubMed] [Google Scholar]
- 91.Preiss A, Heitmann M, Frosch KH. [Osteochondritis dissecans of the talus. Diagnosis and treatment] Unfallchirurg. 2012;115:1099–1108; quiz 1109-1110. doi: 10.1007/s00113-012-2308-7. [DOI] [PubMed] [Google Scholar]
- 92.Kreuz PC, Steinwachs M, Erggelet C, Lahm A, Henle P, Niemeyer P. Mosaicplasty with autogenous talar autograft for osteochondral lesions of the talus after failed primary arthroscopic management: a prospective study with a 4-year follow-up. Am J Sports Med. 2006;34:55–63. doi: 10.1177/0363546505278299. [DOI] [PubMed] [Google Scholar]
- 93.Welsch GH, Mamisch TC, Hughes T, Domayer S, Marlovits S, Trattnig S. Advanced morphological and biochemical magnetic resonance imaging of cartilage repair procedures in the knee joint at 3 Tesla. Semin Musculoskelet Radiol. 2008;12:196–211. doi: 10.1055/s-0028-1083104. [DOI] [PubMed] [Google Scholar]
- 94.Trattnig S, Millington SA, Szomolanyi P, Marlovits S. MR imaging of osteochondral grafts and autologous chondrocyte implantation. Eur Radiol. 2007;17:103–118. doi: 10.1007/s00330-006-0333-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994;15:349–353. doi: 10.1177/107110079401500701. [DOI] [PubMed] [Google Scholar]
- 96.Arrowsmith SR, Fleming LL, Allman FL. Traumatic dislocations of the peroneal tendons. Am J Sports Med. 1983;11:142–146. doi: 10.1177/036354658301100306. [DOI] [PubMed] [Google Scholar]
- 97.Brage ME, Hansen ST. Traumatic subluxation/dislocation of the peroneal tendons. Foot Ankle. 1992;13:423–431. doi: 10.1177/107110079201300711. [DOI] [PubMed] [Google Scholar]
- 98.Mendicino RW, Orsini RC, Whitman SE, Catanzariti AR. Fibular groove deepening for recurrent peroneal subluxation. J Foot Ankle Surg. 2001;40:252–263. doi: 10.1016/s1067-2516(01)80026-0. [DOI] [PubMed] [Google Scholar]
- 99.Kollias SL, Ferkel RD. Fibular grooving for recurrent peroneal tendon subluxation. Am J Sports Med. 1997;25:329–335. doi: 10.1177/036354659702500310. [DOI] [PubMed] [Google Scholar]
- 100.Schöffl V, Küpper T. Prospective evaluation of Rock Climbing Injuries. In preparation. 2013 [Google Scholar]
- 101.Tan V, Lin SS, Okereke E. Superior peroneal retinaculoplasty: a surgical technique for peroneal subluxation. Clin Orthop Relat Res. 2003;(410):320–325. doi: 10.1097/01.blo.0000063594.67412.32. [DOI] [PubMed] [Google Scholar]
- 102.Bouche RT, Sullivan K, Ichikawa DJ. Atheltic injuries. In: Musculoskeletal disorders of the lower extremities, Oloff LM (ed), vol 1st., editors. 410. WB Saunders: Philadelphia; 1994. p. 34. [Google Scholar]
- 103.Gudas CJ, Marcinko DE. Hallux valgus: eine komplexe Deformität. In: Morphologie , Klinik , operative Therpie, editors. Ullstein Mosby: Berlin; 1994. pp. 11–27. [Google Scholar]