

Abstract
AIM: To evaluate the efficacy of gracilis muscle transposition and postoperative salvage irrigation-suction in the treatment of complex rectovaginal fistulas (RVFs) and rectourethral fistulas (RUFs).
METHODS: Between May 2009 and March 2012, 11 female patients with complex RVFs and 8 male patients with RUFs were prospectively enrolled. Gracilis muscle transposition was undertaken in all patients and postoperative wound irrigation-suction was performed in patients with early leakage. Efficacy was assessed in terms of the success rate and surgical complications. SF-36 quality of life (QOL) scores and Wexner fecal incontinence scores were compared before and after surgery.
RESULTS: The fistulas healed in 14 patients after gracilis muscle transposition; the initial healing rate was 73.7%. Postoperative leakage occurred and continuous irrigation-suction of wounds was undertaken in 5 patients: 4 healed and 1 failed, and postoperative fecal diversions were performed for the patient whose treatment failed. At a median follow-up of 17 mo, the overall healing rate was 94.7%. Postoperative complications occurred in 4 cases. Significant improvement was observed in the quality outcomes framework scores (P < 0.001) and Wexner fecal incontinence scores (P = 0.002) after the successful healing of complex RVFs or RUFs. There was no significant difference in SF-36 QOL scores between the initial healing group and irrigation-suction-assisted healing group.
CONCLUSION: Gracilis muscle transposition and postoperative salvage wound irrigation-suction gained a high success rate in the treatment of complex RVFs and RUFs. QOL and fecal incontinence were significantly improved after the successful healing of RVFs and RUFs.
Keywords: Rectovaginal fistula, Rectourethral fistula, Gracilis muscle, Quality of life, Therapeutic irrigation
Core tip: A prospective study of 19 patients with complex rectovaginal fistulas (RVFs) and rectourethral fistulas (RUFs) undergoing gracilis muscle transposition followed by postoperative salvage wound irrigation-suction was reported to yield an overall healing rate of 94.7%. In addition, quality of life and fecal incontinence were reported to be significantly improved after the successful healing of RVFs and RUFs.
INTRODUCTION
Rectovaginal fistulas (RVFs) and rectourethral fistulas (RUFs) are pathological sinus tracts between the rectum and vagina or urethra. The exact incidence of RVFs/RUFs is not known. The reported frequency of RVFs following low anterior rectal resection reached 10%[1-5], and RUFs developed in 0.53% of patients after radical prostatectomy[6]. Moreover, such fistulas have attracted appreciable attention because of their obvious influence on quality of life (QOL) and their difficulty of repair. Multiple surgical procedures to repair these fistulas have been described, but the success rates have varied dramatically, and the sample sizes reported were generally small[7]. The most popular treatments are transrectal or transvaginal flaps, direct peritoneal closure, a wide variety of abdominal procedures (including coloanal anastomosis and tissue interposition), and gracilis muscle transposition[8,9].
Gracilis muscle transposition was first described in 1928 by Garlock[10], who rotated the muscle subcutaneously to the fistula region. The treatment was subsequently applied in patients with vesicovaginal fistulas in 1952[11]. This method satisfies the criteria of relative safety afforded by perineal procedures while providing the healthy, well-vascularized tissue offered by abdominal procedures[12].
After reviewing the results of various repairs (including gracilis muscle transposition for RVFs and RUFs)[13], Wexner et al[11] reported that gracilis muscle transposition is associated with minimal morbidity and a high success rate, but a second repair is needed in some cases. The leakage of anastomoses in the digestive tract was found to be the predominant reason for postoperative fistulization[14]; anastomoses may be cured without surgical intervention by continued irrigation-suction[15].
In the present study, we hypothesized the following: (1) gracilis muscle transposition to repair complex RVFs and RUFs can improve QOL; and (2) continuous wound irrigation-suction during the perioperative period can avoid the need for a second repair and can yield a high success rate.
MATERIALS AND METHODS
Ethical approval of the study protocol
The study protocol was approved by the Ethics Committee of Capital Medical University (Beijing, China). All the patients provided written informed consent before being enrolled in the study.
Patient characteristics and study design
The prospectively registered data were as follows: patient demographics, etiology, clinical manifestation, diagnostic procedures, repair history, use of fecal and/or urinary diversions, fistula type, surgical details, morbidity, and preoperative management. The Wexner score[16] and the Short-Form (SF)-36 score[17] were recorded preoperatively and 6 mo postoperatively by an independent research assistant.
Inclusion criteria and exclusion criteria were: All patients with RUFs were enrolled. However, complex RVFs had to meet one or more of the following criteria: (1) positioning in the upper-third of the rectovaginal septum; (2) size of fistula orifice ≥ 2.5 cm; (3) secondary to inflammatory bowel disease, radiotherapy or a tumor; and (4) having experienced a previous failed repair.
Surgical procedure
The repair of complex RVFs and RUFs via gracilis muscle transposition was conducted as described previously[18]. At the end of surgery, two draining tubes were placed in perineal and leg wounds. All leakages were confirmed as fistula repair failures using the methylene blue test[19]. The perineal tube was routinely replaced with an irrigation-suction device (Changzhou Anker Medical Co., Ltd, Changzhou, China) as soon as leakage was observed from the vagina or from the perineal incision (Figure 1). The procedure was conducted by one surgeon, and local anesthesia was not used. Continuous irrigation with approximately 2000-3000 cm3 of 0.9% saline per day and suction with a negative pressure of 0-0.01 kPa were used for all patients with leakages. The criterion for ending irrigation-suction was that suction collection was clear for > 3 d.
Figure 1.
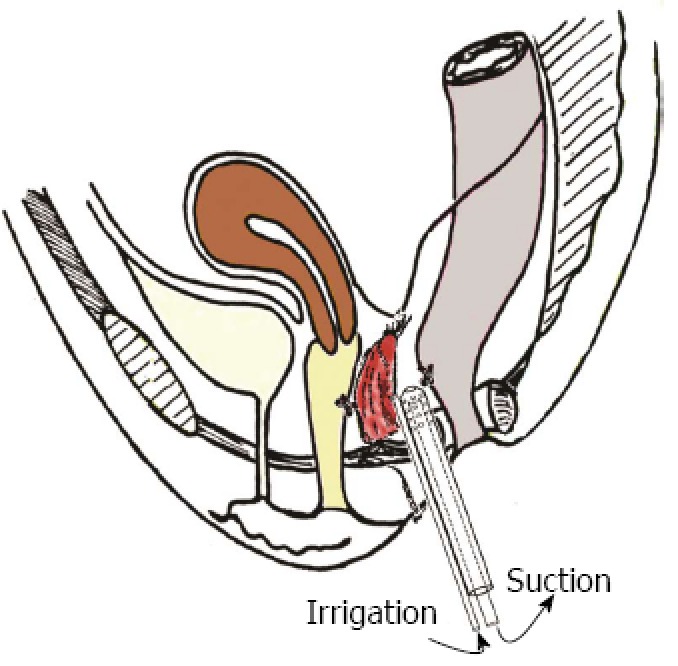
An irrigation-suction device was placed in the leakage site following gracilis muscle transposition.
Fecal diversions were used for 3 mo prior to gracilis interposition in 15 patients with RUFs and RVFs and were removed 3 mo after healing was confirmed. Epicystostomy was undertaken in 7 patients with RUFs before gracilis interposition and was closed 3 mo after healing was confirmed. A urinary catheter was left in place for 1 mo after the RUF procedures. The criteria for successful repair were that the fistula healed within 1 mo postoperatively or from the completion of irrigation-suction. Follow-up began 3 mo after the last hospitalization.
Statistical analysis
Quantitative data were presented as the mean and standard deviation or the median and interquartile range (IQR) depending on whether an underlying normal distribution can be assumed. Numeric data were presented as percentages. Score values were compared using Student’s t test or corresponding nonparametric methods. All the tests were two sided, and P < 0.05 was considered to be of statistical significance.
RESULTS
From May 2009 to November 2011, 18 patients (8 RUFs and 11 complex RVFs) were recruited into the study; 10 patients were excluded (6 because they had simple RVFs and 4 because they underwent procedures other than gracilis muscle transposition).
The median age of the study cohort was 47 years (range, 16-80 years). The median value of the body mass index (BMI) was 21.9 kg/m2 (range, 15.6-29.1 kg/m2). The median duration of the disease was 18 mo (range, 13-48 mo). The etiologies of the RUFs were previous surgery and pelvic irradiation of prostatic carcinoma (n = 5), congenital imperforation (n = 1), bulbourethral infection (n = 1) and pelvic injury (n = 1). The etiologies of the complex RVFs were surgery for rectal cancer (n = 4), gynecologic surgery (n = 3), birth trauma (n = 3) and pelvic injury (n = 1). The mean number of failed attempts was 1 (0-3). Fistulas associated with Crohn’s disease were not observed in this cohort.
All fistulas were in the upper external sphincter and had a mean diameter of 1.6 cm (range, 0.5-3.0 cm). The median duration of surgery was 247 min (range, 120-400 min). The median postoperative hospital stay was 21 d (range, 10-39 d). The median postoperative follow-up was 17 mo (range, 6-34 mo). Postoperative short-term complications were numbness and pain in the thigh (n = 2) and leg numbness (n = 2), and both normalized within 6 mo without surgical intervention. No long-term complications were reported. The initial success rate of fistula healing after gracilis muscle transposition was 73.7% (14/19).
As an early sign of repair failure, postoperative leakage occurred in 5 patients (one male and 4 female). The median age was 53 years (range, 30-75 years). The median time from gracilis muscle transposition to the first leakage was 7 d (range, 6-10 d). Four patients were healed after continuous irrigation-suction, and the median duration of irrigation-suction was 8 d (range, 4-27 d). The overall success rate was 94.7% (18/19). The failed case was a 30-year-old female with RVF following 2 failed repairs. Gracilis muscle transposition was undertaken without preoperative fecal diversion; leakage occurred 6 d after surgery; irrigation-suction was conducted for 27 d and a sigmoid colon stoma was made 12 d postoperatively. However, the fistula persisted during a follow-up period of 22 mo.
The median Wexner score for successfully repaired fistulas was 15 (IQR = 18) and 0 (IQR = 0) before and 6 mo after the surgery, respectively. Fecal incontinence improved significantly after successful repair (P = 0.002). QOL improved significantly after successful healing (P < 0.001; Table 1). No difference was found in QOL in subjects whose fistula repair was successful (“initial success group”) and those healing was successful after irrigation-suction (“secondary success group”; Table 2).
Table 1.
Comparison of SF-36 scores before and after gracilis muscle transposition for complex rectovaginal fistulas and rectourethral fistulas
| Items |
Preoperation (n = 18) |
Postoperation (n = 18) |
P value | ||
| Median | IQR | Median | IQR | ||
| Physical functioning | 65 | 25 | 95 | 5 | < 0.001 |
| Role limitations-physical | 13 | 25 | 100 | 0 | < 0.001 |
| Body pain | 52 | 36 | 90 | 9 | < 0.001 |
| General health | 34 | 19 | 87 | 16 | < 0.001 |
| Vitality | 50 | 16 | 90 | 6 | < 0.001 |
| Social functioning | 44 | 25 | 100 | 16 | < 0.001 |
| Role limitation-emotional | 17 | 33 | 100 | 0 | 0.001 |
| Mental health | 44 | 32 | 92 | 6 | < 0.001 |
IQR: Interquartile range. 0: Poorest; 100: Best.
Table 2.
SF-36 scores in the initial success group and the secondary success group after irrigation-suction
| Items |
Initial success group (n = 14) |
Secondary success group (n = 4) |
P value | ||
| Median | IQR | Median | IQR | ||
| Physical functioning | 95 | 8 | 95 | 4 | 0.277 |
| Role limitation-physical | 100 | 0 | 100 | 0 | 0.721 |
| Body pain | 90 | 16 | 90 | 5 | 0.645 |
| General health | 85 | 9 | 90 | 19 | 0.158 |
| Vitality | 90 | 15 | 88 | 13 | 0.798 |
| Social functioning | 100 | 28 | 100 | 9 | 0.505 |
| Role limitation-emotional | 100 | 0 | 100 | 0 | 0.721 |
| Mental health | 92 | 12 | 92 | 6 | 0.277 |
IQR: Interquartile range. 0: Poorest; 100: Best.
DISCUSSION
The success rate of RUF/RVF repair after gracilis muscle transposition has been reported to be between 77% and 90%[18,20-23]. Wexner et al[11] reported the largest series of 53 RVFs and RUFs with gracilis muscle interposition, and the overall initial success rate was 70%; after seven repeated gracilis muscle transpositions, the final success rate was 87%. In the present study, the initial success rate was 73.7%; after continuous irrigation-suction, the success rate increased to 94.7%. Repeated gracilis muscle transposition was not performed in the present study. Continuous irrigation-suction was effective in improving the success rate of gracilis muscle transposition for complex RVFs and RUFs, and it protected patients from the potential complications associated with a second repair.
QOL is one of the most important outcomes of RVF/RUF repair. However, data related to changes in the QOL of patients with RVFs/RUFs and to the improvement of QOL after repair are lacking. This is the first prospective study to compare the preoperative and postoperative SF-36 scores in RVF/RUF patients after gracilis muscle transposition. Our data showed that the QOL improved significantly after successful RUF/RVF repair. The QOL was similar between the initial success group and secondary success group after irrigation-suction. Successful healing of RUFs/RVFs, after either surgical repair or continuous irrigation-suction, was the key factor in improvement of QOL. Correlations were found between the Wexner score and the SF36 domain scores in patients with pelvic disorders such as urinary incontinence and pelvic organ prolapse[24]. The fecal incontinence score increased significantly after successful healing of RVFs/RUFs in the current study, which may have contributed to the improvement in QOL. However, Lefèvre et al[25] reported that patients with recurrent RVFs have significantly lower postoperative SF-36 scores compared with the general population, while the impact of RVF/RUF repair on QOL remained unknown because the authors did not compare QOL before and after successful repair. Samplaski et al[26] investigated the QOL outcomes in patients undergoing transperineal repair with gracilis muscle interposition for RUF and achieved reasonable bowel and bladder function postoperatively. Further studies aimed at QOL in patients with RVFs or RUFs, especially whether QOL is improved even when fecal incontinence remains unchanged after repair, are needed to provide consensus for clinical care.
An adequate length of the bulky muscular portion of a well-vascularized gracilis to place the muscle between the two suture lines is important for initial success. It is important to place the tip of the irrigation-suction tube close to the leakage site for successful healing. Hence, the length of the irrigation-suction tube underneath the skin should be exactly the same as that of the original tube.
The success rate of gracilis muscle transposition for RUFs is, in general, higher than that for RVFs, and the success rate is considerably higher in non-Crohn’s disease-associated RVFs than in Crohn’s disease-associated RVFs[13]. Crohn’s disease may have a negative impact on fistula healing. In the present study, Crohn’s disease-associated RVF was not encountered, which might explain why that initial success rate and final success rate were considerably higher compared with previous studies. The efficacy of gracilis muscle transposition for Crohn’s-associated RVF needs further verification.
The main limitation of the present study was the low prevalence of postoperative leakage. The number of patients in the secondary success group (only 4) seems too small to provide a meaningful comparison to the initially success group; therefore, we should accept the lack of difference in QOL between the two groups with caution. Further studies comparing postoperative leakage treated with or without perioperative irrigation-suction are necessary before this surgical method can be widely used.
According to the data, gracilis muscle transposition may be indicated in complex RVFs/RUFs resulting from pelvic irradiation, surgical injury, trauma and infection, especially they are associated with malignancy and failed repair. Postoperative irrigation-suction should be considered as soon as a leakage is found. Gracilis muscle transposition and postoperative salvage wound irrigation-suction to treat complex RVFs and RUFs was shown to have a high success rate. QOL and fecal incontinence were improved significantly after the successful healing of RVFs and RUFs.
COMMENTS
Background
The obvious influences of complex rectovaginal fistulas (RVFs) and rectourethral fistulas (RUFs) on quality of life (QOL) and the difficulty of their repairs have attracted extensive attention. Gracilis muscle repair is associated with minimal morbidity and a high success rate, but second repair is often required in some cases.
Research frontiers
The success rate of RUF/RVF repair after gracilis muscle transposition has been reported to be 77%-90%. Data related to changes in the QOL of patients with RVFs/RUFs and to the improvement of QOL after repair have not been reported. This is the first prospective study comparing the preoperative and postoperative SF-36 scores in RVF/RUF patients after gracilis muscle transposition. The data showed that the QOL improved significantly after successful repair of RUF/RVF.
Innovations and breakthroughs
In this study, the initial success rate was 73.7% and, after continuous irrigation-suction, the success rate increased to 94.7%. Repeated gracilis muscle transposition was not carried out in the study. In addition, QOL and fecal incontinence were first reported to significantly improve after successful healing of RVFs and RUFs.
Applications
Postoperative irrigation-suction should be considered as soon as leakage was found.
Terminology
QOL referred to the general well-being of individuals and societies, which is used in a wide range of contexts, including the fields of international development, healthcare, and politics. Within the field of healthcares, QOL is often regarded in terms of how it is negatively affected, on an individual level, a debilitating weakness that is not life-threatening, life-threatening illness that is not terminal, terminal illness, the predictable, natural decline in the health of an elder, an unforeseen mental/physical decline of a beloved one, chronic, end-stage disease processes, etc. RVFs referred to pathological sinus tracts between the rectum and vagina. RUFs referred to pathological sinus tracts between the rectum and urethra.
Peer review
It is an innovative paper dealing with a relevant surgical intervention in fecal incontinence. Though this is a small series it does provide useful information to the readers.
Footnotes
Supported by National Natural Science Foundation of China, No. 81372586
P- Reviewers Chiarioni G, Heise CP S- Editor Cui XM L- Editor Ma JY E- Editor Ma S
References
- 1.Homsi R, Daikoku NH, Littlejohn J, Wheeless CR. Episiotomy: risks of dehiscence and rectovaginal fistula. Obstet Gynecol Surv. 1994;49:803–808. [PubMed] [Google Scholar]
- 2.Senatore PJ. Anovaginal fistulae. Surg Clin North Am. 1994;74:1361–1375. doi: 10.1016/s0039-6109(16)46487-x. [DOI] [PubMed] [Google Scholar]
- 3.Bahadursingh AM, Longo WE. Colovaginal fistulas. Etiology and management. J Reprod Med. 2003;48:489–495. [PubMed] [Google Scholar]
- 4.Saclarides TJ. Rectovaginal fistula. Surg Clin North Am. 2002;82:1261–1272. doi: 10.1016/s0039-6109(02)00055-5. [DOI] [PubMed] [Google Scholar]
- 5.Genadry RR, Creanga AA, Roenneburg ML, Wheeless CR. Complex obstetric fistulas. Int J Gynaecol Obstet. 2007;99 Suppl 1:S51–S56. doi: 10.1016/j.ijgo.2007.06.026. [DOI] [PubMed] [Google Scholar]
- 6.Thomas C, Jones J, Jäger W, Hampel C, Thüroff JW, Gillitzer R. Incidence, clinical symptoms and management of rectourethral fistulas after radical prostatectomy. J Urol. 2010;183:608–612. doi: 10.1016/j.juro.2009.10.020. [DOI] [PubMed] [Google Scholar]
- 7.Fürst A, Schmidbauer C, Swol-Ben J, Iesalnieks I, Schwandner O, Agha A. Gracilis transposition for repair of recurrent anovaginal and rectovaginal fistulas in Crohn’s disease. Int J Colorectal Dis. 2008;23:349–353. doi: 10.1007/s00384-007-0413-9. [DOI] [PubMed] [Google Scholar]
- 8.Hechenbleikner EM, Buckley JC, Wick EC. Acquired rectourethral fistulas in adults: a systematic review of surgical repair techniques and outcomes. Dis Colon Rectum. 2013;56:374–383. doi: 10.1097/DCR.0b013e318274dc87. [DOI] [PubMed] [Google Scholar]
- 9.Ommer A, Herold A, Berg E, Fürst A, Schiedeck T, Sailer M. German S3-Guideline: rectovaginal fistula. Ger Med Sci. 2012;10:Doc15. doi: 10.3205/000166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Garlock JH. The cure of an intractable vesicovaginal fistula by the use of pedicled muscle flap. Surgery Gynecol Obstet. 1928;47:255. [Google Scholar]
- 11.Wexner SD, Ruiz DE, Genua J, Nogueras JJ, Weiss EG, Zmora O. Gracilis muscle interposition for the treatment of rectourethral, rectovaginal, and pouch-vaginal fistulas: results in 53 patients. Ann Surg. 2008;248:39–43. doi: 10.1097/SLA.0b013e31817d077d. [DOI] [PubMed] [Google Scholar]
- 12.Gupta G, Kumar S, Kekre NS, Gopalakrishnan G. Surgical management of rectourethral fistula. Urology. 2008;71:267–271. doi: 10.1016/j.urology.2007.10.042. [DOI] [PubMed] [Google Scholar]
- 13.Nyam DC, Pemberton JH. Management of iatrogenic rectourethral fistula. Dis Colon Rectum. 1999;42:994–997; discussion 997-999. doi: 10.1007/BF02236689. [DOI] [PubMed] [Google Scholar]
- 14.Schweigert M, Dubecz A, Beron M, Muschweck H, Stein HJ. Management of anastomotic leakage-induced tracheobronchial fistula following oesophagectomy: the role of endoscopic stent insertion. Eur J Cardiothorac Surg. 2012;41:e74–e80. doi: 10.1093/ejcts/ezr328. [DOI] [PubMed] [Google Scholar]
- 15.Peng J, Lu J, Xu Y, Guan Z, Wang M, Cai G, Cai S. Standardized pelvic drainage of anastomotic leaks following anterior resection without diversional stomas. Am J Surg. 2010;199:753–758. doi: 10.1016/j.amjsurg.2009.03.026. [DOI] [PubMed] [Google Scholar]
- 16.Rockwood TH, Church JM, Fleshman JW, Kane RL, Mavrantonis C, Thorson AG, Wexner SD, Bliss D, Lowry AC. Patient and surgeon ranking of the severity of symptoms associated with fecal incontinence: the fecal incontinence severity index. Dis Colon Rectum. 1999;42:1525–1532. doi: 10.1007/BF02236199. [DOI] [PubMed] [Google Scholar]
- 17.Lam CL, Tse EY, Gandek B, Fong DY. The SF-36 summary scales were valid, reliable, and equivalent in a Chinese population. J Clin Epidemiol. 2005;58:815–822. doi: 10.1016/j.jclinepi.2004.12.008. [DOI] [PubMed] [Google Scholar]
- 18.Zmora O, Tulchinsky H, Gur E, Goldman G, Klausner JM, Rabau M. Gracilis muscle transposition for fistulas between the rectum and urethra or vagina. Dis Colon Rectum. 2006;49:1316–1321. doi: 10.1007/s10350-006-0585-3. [DOI] [PubMed] [Google Scholar]
- 19.Costa EC, Ferreira CT, Salle JL, Fraga JC. Diagnosis and management of congenital rectourethral fistula in a child with long tubular duplication of the colon and Klippel-Feil syndrome. J Pediatr Surg. 2011;46:2184–2186. doi: 10.1016/j.jpedsurg.2011.08.022. [DOI] [PubMed] [Google Scholar]
- 20.Zmora O, Potenti FM, Wexner SD, Pikarsky AJ, Efron JE, Nogueras JJ, Pricolo VE, Weiss EG. Gracilis muscle transposition for iatrogenic rectourethral fistula. Ann Surg. 2003;237:483–487. doi: 10.1097/01.SLA.0000059970.82125.DB. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rabau M, Zmora O, Tulchinsky H, Gur E, Goldman G. Recto-vaginal/urethral fistula: repair with gracilis muscle transposition. Acta Chir Iugosl. 2006;53:81–84. doi: 10.2298/aci0602081r. [DOI] [PubMed] [Google Scholar]
- 22.Ulrich D, Roos J, Jakse G, Pallua N. Gracilis muscle interposition for the treatment of recto-urethral and rectovaginal fistulas: a retrospective analysis of 35 cases. J Plast Reconstr Aesthet Surg. 2009;62:352–356. doi: 10.1016/j.bjps.2008.11.067. [DOI] [PubMed] [Google Scholar]
- 23.Nassar OA. Primary repair of rectovaginal fistulas complicating pelvic surgery by gracilis myocutaneous flap. Gynecol Oncol. 2011;121:610–614. doi: 10.1016/j.ygyno.2011.02.008. [DOI] [PubMed] [Google Scholar]
- 24.de Mello Portella P, Feldner PC, da Conceição JC, Castro RA, Sartori MG, Girão MJ. Prevalence of and quality of life related to anal incontinence in women with urinary incontinence and pelvic organ prolapse. Eur J Obstet Gynecol Reprod Biol. 2012;160:228–231. doi: 10.1016/j.ejogrb.2011.11.009. [DOI] [PubMed] [Google Scholar]
- 25.Lefèvre JH, Bretagnol F, Maggiori L, Alves A, Ferron M, Panis Y. Operative results and quality of life after gracilis muscle transposition for recurrent rectovaginal fistula. Dis Colon Rectum. 2009;52:1290–1295. doi: 10.1007/DCR.0b013e3181a74700. [DOI] [PubMed] [Google Scholar]
- 26.Samplaski MK, Wood HM, Lane BR, Remzi FH, Lucas A, Angermeier KW. Functional and quality-of-life outcomes in patients undergoing transperineal repair with gracilis muscle interposition for complex rectourethral fistula. Urology. 2011;77:736–741. doi: 10.1016/j.urology.2010.08.009. [DOI] [PubMed] [Google Scholar]