

Abstract
Primary colorectal choriocarcinoma is an extremely rare neoplasm and is usually associated with a poor prognosis. Only 13 cases of colorectal choriocarcinoma have previously been reported. There is no standard chemotherapeutic regimen for this tumor type. A 68-year-old man presented with melena and was diagnosed with sigmoid colonic adenocarcinoma with multiple liver metastases. He underwent a laparoscopic sigmoidectomy. Pathology revealed choriocarcinoma with a focal component of moderately differentiated adenocarcinoma of colon origin. Based on the collagen gel droplet-embedded culture drug sensitivity test (CD-DST) results, mFOLFOX6 and bevacizumab were administered, which suppressed aggressive tumor growth for 4 mo. The patient died 9 mo after the initial diagnosis. Our study results suggest that the standard chemotherapy regimen for colorectal cancer might have suppressive effects against primary colorectal choriocarcinoma. Moreover, CD-DST may provide, at least in part, therapeutic insight for the selection of appropriate antitumor agents for such patients.
Keywords: Colon cancer, Colorectal cancer, Chemotherapy, Culture drug sensitivity test, Choriocarcinoma
Core tip: Primary colorectal choriocarcinoma is an extremely rare neoplasm and is usually associated with a poor prognosis. Only 13 cases of colorectal choriocarcinoma have previously been reported. Systemic chemotherapy is an important prognostic factor in these patients; however, there is no standard chemotherapeutic regimen for this tumor type. We encountered an extremely rare case of choriocarcinoma of the colon which was treated with mFOLFOX6 and bevacizumab based on the results of the culture drug sensitivity test (CD-DST), which suppressed aggressive tumor growth. This suggests that CD-DST may provide, at least in part, therapeutic insight for selecting appropriate antitumor agents for patients with colorectal choriocarcinoma.
INTRODUCTION
Choriocarcinoma is an uncommon malignant tumor that originates from the placenta in women and from germ cells of the gonads in men. Choriocarcinoma is more common in men than in women. Non-gestational or extra-gonadal choriocarcinoma are rare tumors that arise at various sites including the mediastinum[1], lung[2], stomach[3], pancreas[4], cervix[5], and ureter[6]. Primary choriocarcinoma of the colon and rectum is an extremely rare neoplasm and is usually associated with a poor prognosis. Only 13 cases of colorectal choriocarcinoma have previously been reported[7-19]. According to these reports, systemic chemotherapy also appeared to be an important prognostic factor in these patients; however, no standard chemotherapy regimen exists to treat this tumor.
The collagen gel droplet-embedded culture drug sensitivity test (CD-DST) is a new in vitro anticancer drug sensitivity test[20] that has been reported to provide valuable therapeutic information for patients with colorectal cancer[21-23] and pancreatic tumors[24]. We encountered an extremely rare case of primary choriocarcinoma of the sigmoid colon. CD-DST results revealed that the resected tumor was sensitive to several antitumor drugs including oxaliplatin (OHP). Based on the CD-DST results, we administered effective chemotherapy to this patient. To the best of our knowledge, this is the first report of the clinical utility of CD-DST in the treatment of a patient with colonic choriocarcinoma.
CASE REPORT
A 68-year-old man presented with melena. Colonoscopy revealed an ulcerated tumor that occupied half the diameter of the lumen of the sigmoid colon (Figure 1A). A barium enema revealed the tumor to be approximately 2.5 cm in diameter (Figure 1B). Abdominal computed tomography (CT) revealed multiple hepatic tumors and thickening of the intestinal wall of the sigmoid colon. Biopsy of the tumor in the sigmoid colon suggested moderately to poorly differentiated adenocarcinoma. The alpha-fetoprotein (AFP) level was markedly elevated at 298.7 ng/mL (normal range < 20 ng/mL); however, carcinoembryonic antigen (CEA) and CA19-9 levels were within the normal ranges. The patient underwent laparoscopic sigmoidectomy with lymph node dissection to determine the chemosensitivity of the tumor using CD-DST, after which final clinical staging was determined to be T2, N1a, M1a (Stage IVA; Tumor-node-metastasis Classification of Malignant Tumors, 7th Ed.). The surgical specimen was identified as a 20 mm × 20 mm tumor, and was microscopically diagnosed as choriocarcinoma with a focal component of moderately differentiated adenocarcinoma. The adenocarcinoma component was located at the bottom of the ulcer (Figure 2). Regional lymph node metastasis on the primary feeding artery of the tumor was identified. Immunohistochemical staining results were positive for beta-human chorionic gonadotropin (hCG-beta) expression, a marker of choriocarcinoma. The plasma hCG-beta level was elevated to 1.4 ng/mL (normal range < 0.5 ng/mL) even after surgery. CD-DST results revealed that the tumor was sensitive to various chemotherapeutic agents (Table 1).
Figure 1.
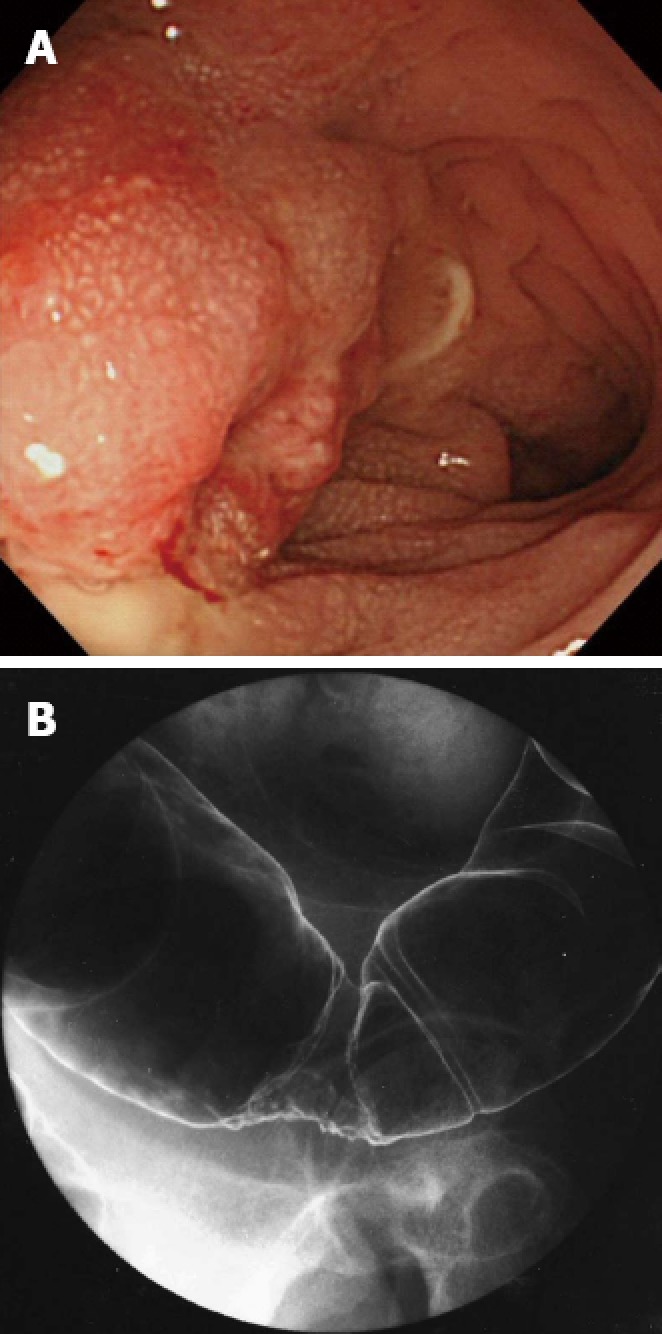
Findings of preoperative examinations. A: Colonoscopy. B: Barium enema.
Figure 2.
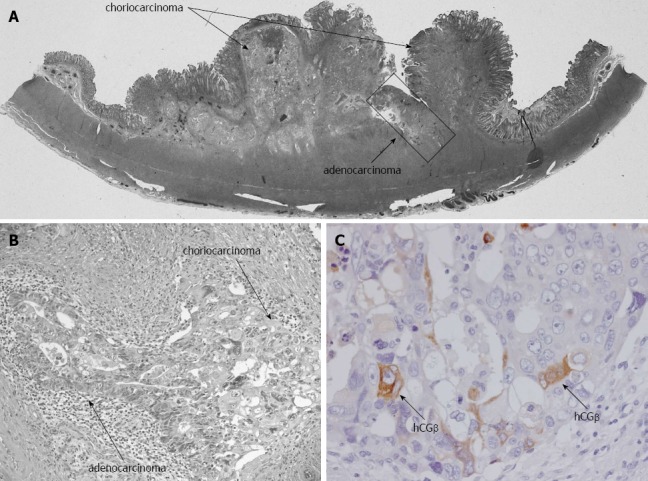
Microscopic findings. A, B: HE staining shows the co-existence of choriocarcinoma and adenocarcinoma cells (A: loupe, B: × 200); C: The tumor cells were positive for β-human chorionic gonadotropin (hCGβ) (× 400).
Table 1.
Summary of antitumor drug sensitivity test results
| Agent (μg/mL) | T/C |
| 5-FU (1.0) | 53.34% |
| Gemcitabine (0.03) | 58.47% |
| Docetaxel (0.1) | 56.07% |
| Epirubicin (0.1) | 58.47% |
| Cisplatin (0.2) | UD |
| 5-FU/SN38 (1.0/0.03) | 65.85% |
| 5-FU/OHP (1.0/0.5) | 46.85% |
The culture drug sensitivity test method was employed to study in vitro growth inhibition. The in vitro sensitivity is expressed as the T/C ratio, where T is the total volume of living cancer cells in the treated group, and C is the total volume of living cancer cells in the control group. 5-FU: 5-fluorouracil; SN38: The active metabolite of irinotecan; OHP: Oxaliplatin; UD: Undetectable because of the limited number of cells.
The patient received his first session of mFOLFOX6 3 wk after surgery. Because the CD-DST results indicated that the tumor was most sensitive to 5-fluorouracil (FU)/OHP, which simulates the FOLFOX combination, the patient received a further 8 courses of mFOLFOX6 with bevacizumab. The size of the hepatic metastases remained almost the same as before surgery; however, a small new lesion was observed on abdominal CT 4 mo after surgery. These findings indicated progressive disease according to RECIST criteria. However, at this point we considered the hepatic tumors unlikely to continue growing because of systemic chemotherapy (Figure 3A and B). However, at 6 mo after surgery, serum AFP and hCG-beta levels rapidly elevated to 3929 and 11 ng/mL, respectively. Thereafter, we administered a regimen of FOLFIRI with bevacizumab. Despite this treatment, the hepatic metastases enlarged markedly (Figure 3C), and the patient died 9 mo after the initial diagnosis.
Figure 3.
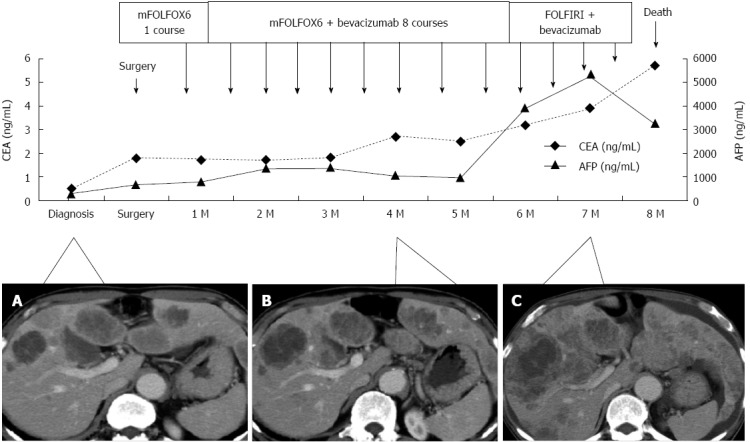
Clinical course of the patient. A, B: Hepatic metastases showed minimal growth until 4 mo after surgery; at 7 mo after surgery; C: The metastases had markedly enlarged, CEA: Carcinoembryonic antigen; AFP: Alpha-fetoprotein.
DISCUSSION
Primary choriocarcinoma of the colon and rectum is extremely rare. To our knowledge only 14 cases including ours have been documented to date. The median age of these patients was 52 years (range, 29-74 years) and included 6 men and 8 women. The median survival period was 4 mo (range, 0.3-60 mo). Metastatic tumors were found in distant organs at the time of colorectal choriocarcinoma diagnosis in 71.4% (10/14) of cases. Of the cases who had no distant metastases at the time of surgery, 80% (4/5) showed rapid development of distant metastases. Only 1 case was reported to have achieved long-term (60 mo), relapse-free survival. These tumors tend to rapidly progress, and are therefore, associated with very poor prognosis. Almost all of the reported patients [85.7% (12/14)] died within 1 year of diagnosis. The survival rate in patients without chemotherapy was significantly lower than that for patients who received some form of chemotherapy (median survival period, without systemic chemotherapy: 1.0 mo vs with systemic chemotherapy: 9 mo, Kaplan-Mayer analysis; Log rank test P = 0.0004, data not shown). Although intestinal resection with lymph node dissection was the standard treatment for colorectal choriocarcinoma in the previous reports, systemic chemotherapy also appeared to be an important prognostic factor. However, no standard chemotherapy regimen has been established for the treatment of this tumor type.
Since colorectal choriocarcinoma is generally considered biologically similar to choriocarcinoma of gestational trophoblastic neoplasia (GTN), almost all previously used chemotherapeutic regimens were based on those designed to treat GTN[25]. Choriocarcinoma is the most common malignant form of GTN. The standard chemotherapeutic regimen for GTN is EMA/CO (a combination of etoposide, methotrexate, and dactinomycin, alternating with cyclophosphamide and vincristine). EMA/CO is reported to have a 60.0%-90.6% complete remission rate and an 86.2% 5-year overall survival (OS)[26]. However, there is no evidence that EMA/CO is effective against colorectal choriocarcinoma.
The prognosis of choriocarcinoma that is of colorectal origin is extremely poor, as shown in this case report. The response of colorectal choriocarcinoma to chemotherapy is much worse than that of choriocarcinoma derived from germ cells. The cause of this difference in chemosensitivity is still unknown. It is known that colorectal choriocarcinoma cells undergo a syncytiotrophoblastic differentiation through retrodifferentiation or metaplasia of the adenocarcinoma component, rather than originating directly from ectopic germ cells. Therefore, it is possible that the differences in chemosensitivity may be associated with the origin of carcinoma cells.
A study by Harada et al[7] reported the efficacy of a systemic chemotherapeutic regimen that contained MEA-methotrexate, etoposide, and dactinomycin which targeted the choriocarcinoma, followed by oral administration of tegafur and uracil/leucovorin therapy which targeted the colonic adenocarcinoma. Although this was a report of a single case, the treatment resulted in very long-term, relapse-free survival (60 mo). Therefore, chemotherapy which not only targeted the choriocarcinoma, but also the adenocarcinoma of the large intestine, appeared to be the key to prolonging survival.
Recently, FOLFOX and FOLFIRI have become standard chemotherapeutic regimens for the treatment of colorectal cancer[27-29]. However, the use of irinotecan- or OHP-containing regimens to treat colorectal choriocarcinoma has not been reported. In this case, the CD-DST results indicated that the tumor was most sensitive to 5-FU/OHP, which simulates the FOLFOX combination. The tumor sample used in the CD-DST was mainly choriocarcinoma; however, the pathological findings revealed the co-existence of moderate-to-poorly differentiated adenocarcinoma. Noguchi et al[30] reported that the survival of a patient with gastric choriocarcinoma was prolonged by administering a chemotherapy regimen commonly given to patients with gastric adenocarcinoma, rather than to those with choriocarcinoma. The regimen for adenocarcinoma in the original tissue appeared to be effective against non-gestational or extra-gonadal choriocarcinoma. Therefore, we hypothesized that the standard regimen for the treatment of colorectal cancer might be effective against primary colorectal choriocarcinoma. We selected mFOLFOX6 combined with bevacizumab with the approval of the patient.
CD-DST cultures extract cancer cells three-dimensionally in a collagen gel droplet. This three-dimensional culture with collagen matrix is preferable to establish cell cultures from human cancer tissue[31]. Here, we report that CD-DST may provide useful information to tailor chemotherapy regimens to individual patients[21,23,24]. Our study demonstrates that patients with synchronous stage IV colorectal cancer who were treated with tumor-sensitive chemotherapeutics as evidenced by the CD-DST had higher response rates (85.71%) than patients receiving drugs that the CD-DST did not identify as tumor-sensitive (41.67%). Moreover, progression-free survival (PFS) and OS were superior in patients treated with in vitro sensitive drugs by CD-DST (median PFS, 696.5 d vs 297.5 d; median OS, 1023.4 d vs 518.5 d)[23]. Unfortunately, the cell culture was not maintained long enough for additional examination of anti-tumor drugs for the EMA/CO regimen after the results of immunohistochemical staining were obtained. Although the best regimen according to the results of the CD-DST suppressed rapid progression of choriocarcinoma in this case, the therapeutic effect in this patient was not remarkable compared with our previous findings of the CD-DST in common colorectal adenocarcinoma[23]. We could not evaluate hepatic metastatic lesions using the CD-DST in this case. It is possible that the chemosensitivity of the hepatic metastases may be different from that of the primary lesion.
In conclusion, we report an extremely rare case of primary choriocarcinoma of the sigmoid colon. Systemic chemotherapy appeared to improve the patient’s survival. This case suggests that the standard regimen for the treatment of colorectal cancer might have suppressive effects against primary colorectal choriocarcinoma. Moreover, CD-DST may provide, at least in part, therapeutic insight for the selection of appropriate antitumor agents which may be effective for treating patients with colonic choriocarcinoma on an individual basis.
Footnotes
P- Reviewer Tsujikawa T S- Editor Zhai HH L- Editor Webster JR E- Editor Ma S
References
- 1.Moran CA, Suster S. Primary mediastinal choriocarcinomas: a clinicopathologic and immunohistochemical study of eight cases. Am J Surg Pathol. 1997;21:1007–1012. doi: 10.1097/00000478-199709000-00004. [DOI] [PubMed] [Google Scholar]
- 2.Seol HJ, Lee JH, Lee KY, Kim JH, Lee NW, Park HJ. Primary pulmonary choriocarcinoma presenting with a hemothorax. J Thorac Oncol. 2009;4:663–665. doi: 10.1097/JTO.0b013e31819cce6c. [DOI] [PubMed] [Google Scholar]
- 3.Imai Y, Kawabe T, Takahashi M, Matsumura M, Komatsu Y, Hamada E, Niwa Y, Kurita M, Shiina S, Shimada T. A case of primary gastric choriocarcinoma and a review of the Japanese literature. J Gastroenterol. 1994;29:642–646. doi: 10.1007/BF02365449. [DOI] [PubMed] [Google Scholar]
- 4.Childs CC, Korsten MA, Choi HS, Schwarz R, Fisse RD. Pancreatic choriocarcinoma presenting as inflammatory pseudocyst. Gastroenterology. 1985;89:426–431. doi: 10.1016/0016-5085(85)90347-6. [DOI] [PubMed] [Google Scholar]
- 5.Maestá I, Michelin OC, Traiman P, Hokama P, Rudge MV. Primary non-gestational choriocarcinoma of the uterine cervix: a case report. Gynecol Oncol. 2005;98:146–150. doi: 10.1016/j.ygyno.2005.03.045. [DOI] [PubMed] [Google Scholar]
- 6.Deodhare S, Leung CS, Bullock M. Choriocarcinoma associated with transitional cell carcinoma in-situ of the ureter. Histopathology. 1996;28:363–365. doi: 10.1046/j.1365-2559.1996.d01-446.x. [DOI] [PubMed] [Google Scholar]
- 7.Harada M, Inoue T, Hamano K. Choriocarcinoma of the sigmoid colon: report of a case. Surg Today. 2012;42:93–96. doi: 10.1007/s00595-011-0026-3. [DOI] [PubMed] [Google Scholar]
- 8.Kubosawa H, Nagao K, Kondo Y, Ishige H, Inaba N. Coexistence of adenocarcinoma and choriocarcinoma in the sigmoid colon. Cancer. 1984;54:866–868. doi: 10.1002/1097-0142(19840901)54:5<866::aid-cncr2820540518>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 9.Lind HM, Haghighi P. Carcinoembryonic antigen staining in choriocarcinoma. Am J Clin Pathol. 1986;86:538–540. doi: 10.1093/ajcp/86.4.538. [DOI] [PubMed] [Google Scholar]
- 10.Nguyen GK. Adenocarcinoma of the sigmoid colon with focal choriocarcinoma metaplasia: a case report. Dis Colon Rectum. 1982;25:230–234. doi: 10.1007/BF02553111. [DOI] [PubMed] [Google Scholar]
- 11.Ordóñez NG, Luna MA. Choriocarcinoma of the colon. Am J Gastroenterol. 1984;79:39–42. [PubMed] [Google Scholar]
- 12.Park CH, Reid JD. Adenocarcinoma of the colon with choriocarcinoma in its metastases. Cancer. 1980;46:570–575. doi: 10.1002/1097-0142(19800801)46:3<570::aid-cncr2820460325>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 13.Tokisue M, Yasutake K, Oya M, Nishisaki H, Nakashima T, Hasegawa H, Sakoda Y, Kizaki T, Sashikata T, Morita R. Coexistence of choriocarcinoma and adenocarcinoma in the rectum: molecular aspects. J Gastroenterol. 1996;31:431–436. doi: 10.1007/BF02355035. [DOI] [PubMed] [Google Scholar]
- 14.Verbeek W, Schulten HJ, Sperling M, Tiesmeier J, Stoop H, Dinjens W, Looijenga L, Wörmann B, Füzesi L, Donhuijsen K. Rectal adenocarcinoma with choriocarcinomatous differentiation: clinical and genetic aspects. Hum Pathol. 2004;35:1427–1430. doi: 10.1016/j.humpath.2004.06.005. [DOI] [PubMed] [Google Scholar]
- 15.Le DT, Austin RC, Payne SN, Dworkin MJ, Chappell ME. Choriocarcinoma of the colon: report of a case and review of the literature. Dis Colon Rectum. 2003;46:264–266. doi: 10.1007/s10350-004-6532-2. [DOI] [PubMed] [Google Scholar]
- 16.Kawahara M, Takada A, Tachibana A, Kodama T, Kobayashi H, Takino Y, Sugishita T, Oono Y, Oka T. Germ cell tumor of the colon with an adenocarcinomatous component. Int J Clin Oncol. 2009;14:537–540. doi: 10.1007/s10147-009-0880-9. [DOI] [PubMed] [Google Scholar]
- 17.Froylich D, Shiloni E, Lavie O, Neumann A, Vlodavsky E, Hazzan D. Colon and lung choriocarcinoma. Isr Med Assoc J. 2010;12:642–644. [PubMed] [Google Scholar]
- 18.Kourda N, Bettaïeb I, Blel A, Zoghlami A, Bedoui R, Najah N, Ben Jilani SB, Zermani R. An aggressive course of de novo ulcerative colitis after renal transplantation: colonic adenocarcinoma with choriocarcinomatous differentiation. Tunis Med. 2009;87:359–361. [PubMed] [Google Scholar]
- 19.Jiang L, Wu JT, Peng X. Primary choriocarcinoma of the colon: a case report and review of the literature. World J Surg Oncol. 2013;11:23. doi: 10.1186/1477-7819-11-23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yasuda H, Takada T, Wada K, Amano H, Isaka T, Yoshida M, Uchida T, Toyota N. A new in-vitro drug sensitivity test (collagen-gel droplet embedded-culture drug sensitivity test) in carcinomas of pancreas and biliary tract: possible clinical utility. J Hepatobiliary Pancreat Surg. 1998;5:261–268. doi: 10.1007/s005340050044. [DOI] [PubMed] [Google Scholar]
- 21.Okumura K, Shiomi H, Mekata E, Kaizuka M, Endo Y, Kurumi Y, Tani T. Correlation between chemosensitivity and mRNA expression level of 5-fluorouracil-related metabolic enzymes during liver metastasis of colorectal cancer. Oncol Rep. 2006;15:875–882. [PubMed] [Google Scholar]
- 22.Fujii R, Seshimo A, Kameoka S. Relationships between the expression of thymidylate synthase, dihydropyrimidine dehydrogenase, and orotate phosphoribosyltransferase and cell proliferative activity and 5-fluorouracil sensitivity in colorectal carcinoma. Int J Clin Oncol. 2003;8:72–78. doi: 10.1007/s101470300013. [DOI] [PubMed] [Google Scholar]
- 23.Takebayashi K, Mekata E, Sonoda H, Shimizu T, Endo Y, Tani T. Clinical potential of the anticancer drug sensitivity test for patients with synchronous stage IV colorectal cancer. Cancer Chemother Pharmacol. 2013;72:217–222. doi: 10.1007/s00280-013-2189-7. [DOI] [PubMed] [Google Scholar]
- 24.Shimizu T, Murata S, Mekata E, Miyake T, Abe H, Kurumi Y, Endo Y, Kushima R, Tani T. Clinical potential of an antitumor drug sensitivity test and diffusion-weighted MRI in a patient with a recurrent solid pseudopapillary tumor of the pancreas. J Gastroenterol. 2007;42:918–922. doi: 10.1007/s00535-007-2105-1. [DOI] [PubMed] [Google Scholar]
- 25.May T, Goldstein DP, Berkowitz RS. Current chemotherapeutic management of patients with gestational trophoblastic neoplasia. Chemother Res Pract. 2011;2011:806256. doi: 10.1155/2011/806256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.El-Helw LM, Hancock BW. Treatment of metastatic gestational trophoblastic neoplasia. Lancet Oncol. 2007;8:715–724. doi: 10.1016/S1470-2045(07)70239-5. [DOI] [PubMed] [Google Scholar]
- 27.Furuta T. Pharmacogenomics in chemotherapy for GI tract cancer. J Gastroenterol. 2009;44:1016–1025. doi: 10.1007/s00535-009-0124-9. [DOI] [PubMed] [Google Scholar]
- 28.Park LC, Lee HS, Shin SH, Park SJ, Park MI, Oh SY, Kwon HC, Baek JH, Choi YJ, Kang MJ, et al. Bevacizumab as a second- or later-line of treatment for metastatic colorectal cancer. World J Gastroenterol. 2012;18:1104–1109. doi: 10.3748/wjg.v18.i10.1104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Wang Y, Shen L, Xu N, Wang JW, Jiao SC, Liu ZY, Xu JM. UGT1A1 predicts outcome in colorectal cancer treated with irinotecan and fluorouracil. World J Gastroenterol. 2012;18:6635–6644. doi: 10.3748/wjg.v18.i45.6635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Noguchi T, Takeno S, Sato T, Takahashi Y, Uchida Y, Yokoyama S. A patient with primary gastric choriocarcinoma who received a correct preoperative diagnosis and achieved prolonged survival. Gastric Cancer. 2002;5:112–117. doi: 10.1007/s101200200019. [DOI] [PubMed] [Google Scholar]
- 31.Kobayashi H. Development of a new in vitro chemosensitivity test using collagen gel droplet embedded culture and image analysis for clinical usefulness. Recent Results Cancer Res. 2003;161:48–61. doi: 10.1007/978-3-642-19022-3_5. [DOI] [PubMed] [Google Scholar]