

Misperceptions about personal weight are common and include both under- and overestimates.1–6 Overweight misperception is found among both males and females across different racial/ethnic and age groups but is generally more common among females. Studies also indicate that body weight misperception is common among university students.2,4,7,8 In a study assessing the prevalence of weight misperception among U.S. college students, 12.9% of students had inflated body weight perception and 15.1% considered themselves to be thinner than they actually were.7 Gender and racial/ethnic differences in weight misperception have been observed among normal-weight college adults. According to the 2008 National College Health Assessment (NCHA), 28.8% of college females and 39.4% of college males were overweight or obese. However, more females (38.0%) than males (30.8%) described themselves as overweight or obese.8 Non-Hispanic white people are also more likely to report overweight misperception than other racial/ethnic minority groups.8,9
In the United States, trends suggest that the prevalence of weight misperception is increasing. Findings from the 2002–2003 NCHA study showed that 12% of U.S. college students had inaccurate weight perceptions; this prevalence increased to 28% during the 2006 NCHA assessment.8 These trends have led some researchers to argue that there may be conflicting influences on weight perception: recognition of the obesity epidemic as a public health concern could decrease misperception, while exposure to negative weight-related images and weight stigmatization could further exacerbate body weight inaccuracies.7
Prior studies suggest that while the increased prevalence of obesity in the population has an objectively measurable impact on the actual experience of one's health, the impact of excess body weight on subjective perceptions of quality-of-life domains must also be considered.10–14 Excess body weight has been associated with both immediate and long-term health, psychological, and emotional consequences.13,14 A study conducted on self-reported body mass index (BMI) and health-related quality of life (HRQoL) among U.S. adults, using data from the 1996 Behavioral Risk Factor Surveillance System (BRFSS), concluded that participants with a self-reported BMI <18.5 kilograms per square meter (kg/m2) and ≥30 kg/m2 had increased odds of reporting poor or fair self-rated health and ≥14 days of poor physical and mental health during the previous 30 days.13 A similar study among adults in Belgrade found that impaired physical functioning was an outcome for individuals with a self-reported BMI ≥25 kg/m2.14
Moreover, research has pointed to a possible link between weight perception and subjective assessments of health. Understanding this relationship is an important area of research because of the implications of weight misperception among college students. For example, misperception of overweight is regularly shown to be associated with negative self-concepts,1,15 psychological distress,16–18 depression,7,9,15 negative body image,9 and inappropriate weight-control practices,7,9,16 all of which are factors that may potentiate HRQoL impairments.1,15 Despite the large body of evidence linking misperceptions of overweight with psychological dysfunction, there is a paucity of research on the relationship between weight misperception and HRQoL.
HRQoL is a broad, multidimensional, subjective concept that can be used by clinicians, researchers, and public health professionals to understand the impact of disease, illness, and disability on an individual's perceived physical and mental health and ability to perform everyday activities.19 While it is not well known whether weight misperceptions are independently associated with HRQoL, some studies do suggest an association.9,15,17,18 A study conducted on weight perception and psychological and emotional resources among U.S. college students concluded that weight misperception was associated with increased odds of depression and binge eating.7 Furthermore, Eaton et al. found that regardless of actual BMI, high school adolescents who misperceived their weight were at increased risk for suicidal ideation.18 Similar outcomes have been documented for adult populations. Among adults, overweight perception increased risk for psychological distress regardless of weight status,15 while inflated body weight perception led to greater depressive symptomology.9
The potential health and psychosocial risks associated with weight misperception are well-established; however, very few studies are focused on the link between inaccurate body weight perception and HRQoL. Because weight misperception is associated with negative psychological and emotional outcomes, weight misperception may also represent a potential mechanism through which HRQoL is impaired. Therefore, we examined the association between weight misperception and HRQoL among college students. Examination of this phenomenon is particularly relevant among normal-weight college students because overweight misperception may be a precursor to diminished subjective health status. We hypothesized that misperception of overweight would lead to greater HRQoL deficits in otherwise healthy college students.
METHODS
Using data collected from 369 randomly selected college students attending a public university in central Appalachia, we examined how weight misperception was associated with HRQoL. We developed a survey to assess the general health of students. An individual was included in the study if he/she was ≥18 years of age and a full-time student. Electronic surveys were completed by students during January–February 2010.
We used the Centers for Disease Control and Prevention (CDC) Healthy Days core questions (HRQoL-4) to assess subjective HRQoL. CDC developed this four-item set of questions20 to address the need for a brief, valid measure to track mental and physical health disparities and trends in populations.21 The HRQoL-4 includes four questions: (1) “Would you say that in general your health is excellent, very good, good, fair, or poor?”; (2) “Now thinking about your physical health, which includes physical illness and injury, for how many days during the past 30 days was your physical health not good?”; (3) “Now thinking about your mental health, which includes stress, depression, and problems with emotions, for how many days during the past 30 days was your mental health not good?”; and (4) “During the past 30 days, for about how many days did poor physical or mental health keep you from doing your usual activities, such as self-care, work, or recreation?” Responses to the questions about number of recent days when physical or mental health was poor were then summed to create an unhealthy days summary index.
We based BMI on self-reported height and weight. We categorized participants as underweight (BMI <18.5 kg/m2), normal weight (BMI ≥18.5 kg/m2 and <25 kg/m2), overweight (BMI ≥25 kg/m2 and <30 kg/m2), and obese (BMI ≥30 kg/m2). We assessed weight perception with one question, “How do you describe your weight?” Response options ranged from “very underweight” to “very overweight.” Weight misperception occurs when one's subjective perceptions do not correspond with objective weight status.
A robust relationship exists between overweight misperception and psychological health;5,15–18 therefore, we chose to analyze differences in college students with normal self-reported BMI and inflated or accurate body weight perception. A total of 137 students had a normal self-reported BMI and described their weight as either “about the right weight,” “slightly overweight,” or “very overweight.” Based on prior recommendations,9,22 we categorized participants as having overweight misperception if they perceived themselves as slightly or very overweight when their BMIs were normal weight. Additionally, we categorized participants as having accurately perceived their weight if they perceived themselves as about the right weight when their BMIs were normal. We assessed dietary behaviors by asking six questions about daily fruit and vegetable intake (options ranged from 0 times in past seven days to four times per day). Responses were summed to calculate total daily fruit and vegetable intake. We assessed physical activity by asking, “During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day?” We assessed weight consciousness by asking, “If anything, what are you trying to do about your weight?” Response options ranged from “lose weight” to “gain weight.”
We explored bivariate relationships by weight perception using Chi-square and t-test statistics. We used these analyses to investigate the relationships between selected independent variables and weight misperception of college students. To examine the association of weight misperception with HRQoL, we used multiple logistic regression and multiple linear regression to simultaneously adjust for covariates. We included the following covariates because of their potential association with HRQoL: gender (male/female), age, race/ethnicity (white/Caucasian and racial/ethnic minority group), physical activity (number of physical activity days in past seven days), and dietary behaviors (daily fruit and vegetable intake).3,14,23 We considered an alpha level of 0.05 to be statistically significant. We performed all analyses using PASW Statistics version 18.0.24
RESULTS
The characteristics of the study sample are shown in Table 1. Among the 137 study respondents, 102 (74.5%) were female and 117 (85.4%) were white/Caucasian. The mean age of the study sample was 24.6 years (standard deviation [SD] = 8.2). Among respondents categorized as being normal weight (i.e., a BMI ≥18.5 kg/m2 and <25 kg/m2), 33 (24.1%) misperceived themselves as overweight (data not shown). Of this percentage, 27 (26.5%) were female and six (17.1%) were male. A total of 27 (23.1%) white college students and six (30.0%) students from racial/ethnic minority groups misperceived themselves as overweight. Overall, 71 (51.8%) respondents reported trying to lose weight, including those who did not perceive themselves to be overweight (Table 1).
Table 1.
Sample characteristics and characteristics by weight perception accuracy among college students (n=137) in central Appalachia with normal actual BMI: January–February 2010

aSignificant at p≤0.05
bRefers to the unhealthy days summary index (i.e., number of recent days when physical or mental health was poor)
cDefined as ≥14 physically unhealthy days in the past 30 days
dDefined as ≥14 mentally unhealthy days in the past 30 days
eDefined as ≥14 days with limitations to daily activities in the past 30 days
fRefers to consuming less than the daily recommended number of fruit and vegetables (<5 per day)
gRefers to ≥60 minutes a day of moderate to vigorous physical activity
BMI = body mass index
SD = standard deviation
In the bivariate analysis, weight misperception prevalence varied substantially by selected characteristics (Table 1). Three (9.1%) college students who misperceived themselves as overweight reported being in fair to poor health compared with one (1.0%) student who accurately perceived his/her weight (p=0.04). Students who misperceived themselves as overweight were also more likely than those who accurately perceived their weight to report frequent mental distress (i.e., defined as ≥14 mentally unhealthy days in the past 30 days [25.8% vs. 9.8%, p=0.02]). Overweight misperception was further associated with dietary and physical activity behaviors. The students who misperceived themselves as overweight consumed less fruit and vegetables than those who accurately perceived their weight. Approximately 97.0% of these students consumed less than the daily recommended amount of fruit and vegetables (i.e., ≥5 fruit and vegetables daily) compared with 84.3% of students who accurately perceived their weight (p=0.04).
Self-perception of overweight was also an indicator of weight-loss intentions. Approximately three-quarters of college students who misperceived themselves as overweight (n=26, 78.8%) were trying to lose weight compared with only 45 (43.3%) students who accurately perceived their weight (p=0.002). College students misperceiving their weight reported fewer physical activity days in the past seven days (mean = 3.3, SD=1.9) than those who accurately perceived their weight (mean = 4.3, SD=2.2) (p=0.02). There were no significant differences observed in overweight misperception and accurate weight perception by gender, age, race/ethnicity, or other HRQoL domains.
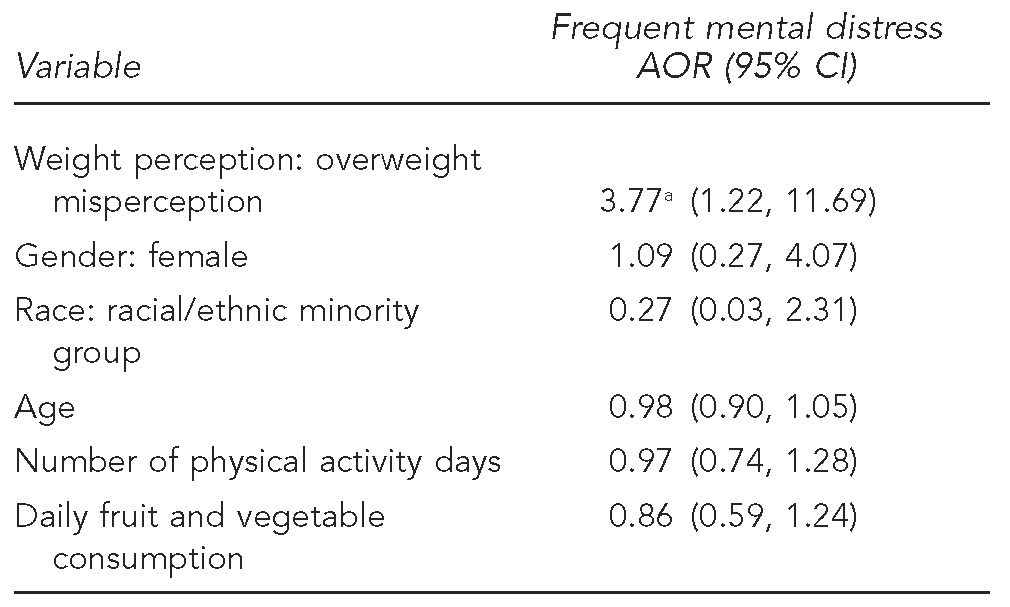
After adjusting for age, race/ethnicity, gender, physical activity, and dietary behaviors, frequent mental distress was the only HRQoL outcome that had a significant association with weight misperception. Among normal-weight college students, those who misperceived themselves as overweight were almost four times more likely to have frequent mental distress than those students with accurate weight perception (odds ratio = 3.77, 95% confidence interval 1.22, 11.69) (Table 2).
Table 2.
Adjusted odds for frequent mental distress by weight perception among college students (n=137) in central Appalachia with normal self-reported BMI: January–February 2010
ap<0.05
BMI = body mass index
OR = adjusted odds ratio
CI = confidence interval
DISCUSSION
We explored the association between overweight misperception and HRQoL among normal-weight college students and found that a significant percentage of normal-weight students (24.1%) perceived themselves as overweight and that more than half (51.8%) reported trying to lose weight despite their normal BMI. These findings are similar to results from other studies.7,8,25–27 It is apparent that there is an ongoing concern regarding weight among college students of both normal and overweight perception categories; however, in this study, concern for weight was more apparent among students who misperceived themselves as overweight, an outcome consistent with prior research.9,26,27 An unexpected finding was that there were no gender or racial/ethnic differences in weight perception accuracy in this sample, despite strong support in the literature for these assocations.7–9,28,29 This finding may be due in part to the small sample size in each subgroup. There is growing acknowledgement, however, that sociocultural pressures to remain thin are increasing among college-aged males and racial/ethnic minority groups.4 Furthermore, inconsistencies in recent research suggest a normalizing of overweight misperception across racial/ethnic categories.7 Overweight misperception was also associated with lower levels of physical activity and poorer dietary behaviors, findings that warrant further investigation due to the inconsistent associations reported in prior studies.30
We also found that overweight misperception was associated with several dimensions of HRQoL. In our study, normal-weight students who considered themselves overweight reported poorer self-rated health and more frequent mental distress. These findings suggest that overweight misperception is important in the -formulation of one's subjective health status and quality of life.7,9,15,18 Health education interventions are needed across college campuses to counter weight perception inaccuracies and to promote a healthy body esteem, factors that are important for improving the students' physical, psychological, and emotional health.
The results of our study were confirmed by a multivariate linear regression model that linked overweight misperception to frequent mental distress after adjusting for personal characteristics, which is in agreement with prior studies.15,17,18 Longitudinal studies are needed to prospectively examine how self-perception of overweight impacts the various aspects of mental health. This finding suggests, however, that misperception of overweight may be important in shaping college students' psychological functioning, independent of personal characteristics. Correcting misperceptions about weight status may be important to buttressing the psychological well-being and resilience of college students. Moreover, that weight stigma can have adverse immediate and long-term effects on physical and emotional health31 may explain the robust relationship between overweight misperception and the mental health of students. Positive media messages are needed to draw attention to weight bias that is pervasive in Western societies. Likewise, studies indicate that weight perceptions are modifiable and, therefore, important clinical considerations.32 Although there has been considerable research on changes in body weight norms and weight desensitization,33–36 this study underscores the importance of continued surveillance of weight misperception and its relationship to HRQoL in normal-weight populations. Providing information about weight misperception, body image, and self-acceptance to college students may be useful when planning obesity prevention efforts on university campuses.
There appeared to be no independent link between overweight misperception and the various physical domains of health when controlling for demographic differences, which may indicate that weight misperception has a more robust effect on the psycho-emotive dimensions of quality of life. Likewise, other research that focused on weight misperception yielded similar findings. For example, Atlantis and Ball argue that inconsistencies in the obesity-depression literature suggest that weight perception rather than actual BMI is associated with depression.15 Our results confirmed this finding and further demonstrate the need for clinicians and public health professionals to examine the role of overweight misperception in the formulation of subjective assessments of health, specifically with regard to psychological and emotional functioning.
Limitations
Caution should be used when interpreting and generalizing these findings. Causality cannot be determined with a cross-sectional design. The low response rate (12%) may limit the validity of the study's findings; however, several recent reviews suggest little relationship between response rates and nonresponse bias.37–39 Another important limitation was that BMI was obtained through self-report, although many prior studies examining weight misperception used self-report measurements of BMI.9,26 Misclassification bias due to underreporting of weight with overreporting of height22,40 is an inherent problem with self-report measures. Despite this limitation, several studies have suggested that self-reported BMI may be appropriate with certain populations.41 For example, there is generally less underreporting of weight with overreporting of height in younger adults compared with older populations.42 Finally, this study did not assess factors potentially related to HRQoL, such as presence of chronic conditions, eating disorders, or social support.9,15,17,18
CONCLUSIONS
This study provides new information on the nature of the association between overweight misperception and HRQoL. Overweight misperception should be considered when attempting to understand and predict which college students are likely to have impaired mental health functioning. Additional programming targeting body weight distortion is needed by colleges and universities to promote greater awareness and self-acceptance, regardless of weight status. Future longitudinal research on the relationship between overweight misperception and HRQoL should examine this relationship across BMI classifications to more effectively screen at-risk populations.
A significant portion of normal-weight college students misperceived themselves as overweight. This study also suggests that overweight misperception is associated with frequent mental distress among normal-weight college students. These findings highlight the need to (1) address both weight perceptions and subjective assessments of health and (2) change individual normative perceptions as well as the environments that affect those perceptions. For example, while the majority of public health efforts concentrate on the obesity epidemic in our society, our results highlight the need for a comprehensive approach to addressing healthy weight issues among college students. Many university administrators working to address obesity issues may target overweight or obese college students, with little attention given to the majority of students who, despite their normal weight, may struggle with psychological distress as a result of conflicting social media messages and images. As the role of overweight misperception in identifying college students at risk for frequent mental distress becomes more established, research into how individuals conceptualize their weight may aid in developing public health campaigns throughout university campuses that facilitate more accurate assessments of body image and weight perception.
Footnotes
Study procedures were approved by the Eastern Tennessee State University (ETSU) Institutional Review Board and informed consent was obtained from study participants.
REFERENCES
- 1.Chang VW, Christakis NA. Self-perception of weight appropriateness in the United States. Am J Prev Med. 2003;24:332–9. doi: 10.1016/s0749-3797(03)00020-5. [DOI] [PubMed] [Google Scholar]
- 2.Saules KK, Collings AS, Hoodin F, Angelella NE, Alschuler K, Ivezaj V, et al. The contributions of weight problem perception, BMI, gender, mood, and smoking status to binge eating among college students. Eat Behav. 2009;10:1–9. doi: 10.1016/j.eatbeh.2008.07.010. [DOI] [PubMed] [Google Scholar]
- 3.Yan AF, Zhang G, Wang MQ, Stoesen CA, Harris BM. Weight perception and weight control practice in a multiethnic sample of US adolescents. South Med J. 2009;102:354–60. doi: 10.1097/SMJ.0b013e318198720b. [DOI] [PubMed] [Google Scholar]
- 4.Sheldon P. Pressure to be perfect: influences on college students' body esteem. South J Comm. 2010;75:277–98. [Google Scholar]
- 5.Dorsey RR, Eberhardt MS, Ogden CL. Racial/ethnic differences in weight perception. Obesity (Silver Spring) 2009;17:790–5. doi: 10.1038/oby.2008.603. [DOI] [PubMed] [Google Scholar]
- 6.Foti K, Lowry R. Trends in perceived overweight status among overweight and nonoverweight adolescents. Arch Pediatr Adolesc Med. 2010;164:636–42. doi: 10.1001/archpediatrics.2010.90. [DOI] [PubMed] [Google Scholar]
- 7.Harring HA, Montgomery K, Hardin J. Perceptions of body weight, weight management strategies, and depressive symptoms among U.S. college students. J Am Coll Health. 2011;59:43–50. doi: 10.1080/07448481.2010.483705. [DOI] [PubMed] [Google Scholar]
- 8.American College Health Association. American College Health Association-National College Health Assessment Spring 2008 Reference Group data report (abridged): the American College Health Association. J Am Coll Health. 2009;57:477–88. doi: 10.3200/JACH.57.5.477-488. [DOI] [PubMed] [Google Scholar]
- 9.Ratanasiripong P, Burkey H. Body mass index and body size perception: a normalizing of overweight and obesity among diverse college students. Californian J Health Promot. 2011;9:18–24. [Google Scholar]
- 10.Sullivan M, Karlsson J, Ware JE., Jr The Swedish SF-36 Health Survey—I. Evaluation of data quality, scaling assumptions, reliability, and construct validity across general populations in Sweden. Soc Sci Med. 1995;41:1349–58. doi: 10.1016/0277-9536(95)00125-q. [DOI] [PubMed] [Google Scholar]
- 11.Visscher TL, Seidel JC. The public health impact of obesity. Annu Rev Public Health. 2001;22:355–75. doi: 10.1146/annurev.publhealth.22.1.355. [DOI] [PubMed] [Google Scholar]
- 12.Kolotkin RL, Meter K, Williams GR. Quality of life and obesity. Obes Rev. 2001;2:219–29. doi: 10.1046/j.1467-789x.2001.00040.x. [DOI] [PubMed] [Google Scholar]
- 13.Ford ES, Moriarty DG, Zack MM, Mokdad AH, Chapman DP. Self-reported body mass index and health-related quality of life: findings from the Behavioral Risk Factor Surveillance System. Obes Res. 2001;9:21–31. doi: 10.1038/oby.2001.4. [DOI] [PubMed] [Google Scholar]
- 14.Vasiljevic N, Ralevic S, Marinkovic J, Kocev N, Maksimovic M, Milosevic GS, et al. The assessment of health-related quality of life in relation to the body mass index value in the urban population of Belgrade. Health Qual Life Outcomes. 2008;6:106. doi: 10.1186/1477-7525-6-106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Atlantis E, Ball K. Association between weight perception and psychological distress. Int J Obes (Lond) 2008;32:715–21. doi: 10.1038/sj.ijo.0803762. [DOI] [PubMed] [Google Scholar]
- 16.Farrell C, Lee M, Shafran R. Assessment of body size estimation: a review. Eur Eat Disord Rev. 2005;13:75–88. [Google Scholar]
- 17.Bogt TF, van Dorsselaer SA, Monshouwer K, Verdurmen JE, Engels RC, Vollebergh WA. Body mass index and body weight perception as risk factors for internalizing and externalizing problem behavior among adolescents. J Adolesc Health. 2006;39:27–34. doi: 10.1016/j.jadohealth.2005.09.007. [DOI] [PubMed] [Google Scholar]
- 18.Eaton DK, Lowry R, Brener ND, Galuska DA, Crosby AE. Associations of body mass index and perceived weight with suicide ideation and suicide attempts among US high school students. Arch Pediatr Adolesc Med. 2005;159:513–9. doi: 10.1001/archpedi.159.6.513. [DOI] [PubMed] [Google Scholar]
- 19.Centers for Disease Control and Prevention (US) Measuring healthy days: population assessment of health-related quality of life. 2000 [cited 2013 Jun 11] Available from: URL: http://www.cdc.gov/hrqol/pdfs/mhd.pdf.
- 20.Centers for Disease Control and Prevention (US) Health-related quality of life (HRQoL) [cited 2011 Jul 1] Available from: URL: http://www.cdc.gov/hrqol/index.htm.
- 21.Hennessy CH, Moriarty DG, Zack MM, Scherr PA, Brackbill R. Measuring health-related quality of life for public health surveillance. Public Health Rep. 1994;109:665–72. [PMC free article] [PubMed] [Google Scholar]
- 22.Wharton CM, Adams T, Hampl JS. Weight loss practices and body weight perceptions among US college students. J Am Coll Health. 2008;56:579–84. doi: 10.3200/JACH.56.5.579-584. [DOI] [PubMed] [Google Scholar]
- 23.Schünemann HJ, Sperati F, Barba M, Santesso N, Melegari C, Akl EA, et al. An instrument to assess quality of life in relation to nutrition: item generation, item reduction and initial validation. Health Qual Life Outcomes. 2010;8:26. doi: 10.1186/1477-7525-8-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.SPSS Inc. PASW Statistics: Version 18.0 for Windows. Chicago: SPSS Inc.; 2009. [Google Scholar]
- 25.Brener ND, Eaton DK, Lowry R, McManus T. The association between weight perception and BMI among high school students. Obes Res. 2004;12:1866–74. doi: 10.1038/oby.2004.232. [DOI] [PubMed] [Google Scholar]
- 26.Talamayan KS, Springer AE, Kelder SH, Gorospe EC, Joye KA. Prevalence of overweight misperception and weight control behaviors among normal weight adolescents in the United States. Scientific World J. 2006;6:365–73. doi: 10.1100/tsw.2006.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wharton CM, Adams T, Hampl JS. Weight loss practices and body weight perceptions among US college students. J Am Coll Health. 2008;56:579–84. doi: 10.3200/JACH.56.5.579-584. [DOI] [PubMed] [Google Scholar]
- 28.Serdula MK, Collins ME, Williamson DF, Anda RF, Pamuk E, Byers TE. Weight control practices of U.S. adolescents and adults. Ann Intern Med. 1993;119:667–71. doi: 10.7326/0003-4819-119-7_part_2-199310011-00008. [DOI] [PubMed] [Google Scholar]
- 29.Kumanyika SK. Special issues regarding obesity in minority populations. Ann Intern Med. 1993;119(7 Pt 2):650–4. doi: 10.7326/0003-4819-119-7_part_2-199310011-00005. [DOI] [PubMed] [Google Scholar]
- 30.Atlantis E, Barnes EH, Ball K. Weight status and perception barriers to healthy physical activity and diet behavior. Int J Obes (Lond) 2008;32:343–52. doi: 10.1038/sj.ijo.0803707. [DOI] [PubMed] [Google Scholar]
- 31.Major B, Eliezer D, Rieck H. The psychological weight of weight stigma. Soc Psychol Pers Sci 2012 Oct 12 [cited 2013 Jan 19] Available from: URL: http://spp.sagepub.com/content/early/2012/0/18/1948550611434400.
- 32.Abid A, Galuska D, Khan LK, Gillespie C, Ford ED, Serdula MK. Are healthcare professionals advising obese patients to lose weight? A trend analysis. MedGenMed. 2005;7:10. [PubMed] [Google Scholar]
- 33.Kuk JL, Ardern CI, Church TS, Hebert JR, Sui X, Blair SN. Ideal weight and weight satisfaction: association with health practices. Am J Epidemiol. 2009;170:456–63. doi: 10.1093/aje/kwp135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Burke MA, Heiland FW, Nadler CM. From “overweight” to “about right”: evidence of a generational shift in body weight norms. Obesity (Silver Spring) 2010;18:1226–34. doi: 10.1038/oby.2009.369. [DOI] [PubMed] [Google Scholar]
- 35.Johnson-Taylor WL, Fisher RA, Hubbard VS, Starke-Reed R, Eggers PS. The change in weight perception of weight status among the overweight: comparison of NHANES III (1988–1994) and 1999–2004 NHANES. Int J Behav Nutr Phys Act. 2008;5:9. doi: 10.1186/1479-5868-5-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Stommel M, Osier N. Temporal changes in bias of body mass index score based on self-reported height and weight. Int J Obes (Lond) 2013;37:461–7. doi: 10.1038/ijo.2012.67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Groves RM, Peytcheva E. The impact of nonresponse rates on nonresponse bias: a meta-analysis. Public Opin Q. 2008;72:167–89. [Google Scholar]
- 38.Groves RM. Nonresponse rates and nonresponse bias in household surveys. Public Opin Q. 2006;70:646–75. [Google Scholar]
- 39.Keeter S, Kennedy C, Dimock M, Best J, Craighill P. Gauging the impact of growing nonresponse on estimates from a national RDD telephone survey. Public Opin Q. 2006;70:759–9. (5 special issue) [Google Scholar]
- 40.Brener ND, McManus T, Galuska DA, Lowry R, Wechsler H. Reliability and validity of self-reported height and weight among high school students. J Adolesc Health. 2003;32:281–7. doi: 10.1016/s1054-139x(02)00708-5. [DOI] [PubMed] [Google Scholar]
- 41.Spencer EA, Appleby PN, Davey GK, Key TJ. Validity of self-reported height and weight in 4808 EPIC-Oxford participants. Public Health Nutr. 2002;5:561–5. doi: 10.1079/PHN2001322. [DOI] [PubMed] [Google Scholar]
- 42.Kuczmarski MF, Kuczmarski RJ, Najjar M. Effects of age on validity of self-reported height, weight, and body mass index: findings from the Third National Health and Nutrition Examination Survey, 1988–1994. J Am Diet Assoc. 2001;101:28–34. doi: 10.1016/S0002-8223(01)00008-6. [DOI] [PubMed] [Google Scholar]