

Summary
This study examined trends in overweight among women of reproductive age by educational level in 33 low- and middle income countries, and estimated the contribution of parity, age at first birth and breastfeeding to these trends. We used repeated cross-sectional demographic health surveys (DHS) of 255,828 women aged 25-49 years interviewed between 1992 and 2009. We applied logistic regression to model overweight (> 25 kg/m2) as a function of education, reproductive variables and time period by country and region. The prevalence of overweight ranged from 3.4% in South and Southeast Asia to 73.7% in North Africa West/Central Asia during the study period. The association between education and overweight differed across regions. In North Africa West/Central Asia and Latin American, lower education was associated with higher overweight prevalence, while the inverse was true in South/Southeast Asia and Sub-Saharan Africa. In all regions, there was a consistent pattern of increasing overweight trends across all educational groups. Older age at first birth, longer breastfeeding, and lower parity were associated with less overweight, but these variables did not account for the association or the increasing trends between education and overweight.
Keywords: overweight, education, parity, breastfeeding, developing countries
INTRODUCTION
Obesity is a major emerging risk factor for chronic disease among women in low- and middle-income countries1, but there are substantial differences in the prevalence of both overweight and obesity among these countries2. The most recent information showed that the prevalence of overweight among women during the last three decades has ranged from as low as 5.6% in Ethiopia to 93.0% in Tonga3, but there has been a pattern of increase in overweight and obesity in most countries1. Women of reproductive age have not been immune to these trends and have suffered important increases in body mass index during recent years 1. Evidence suggests that among these women, higher income and wealth are associated with higher prevalence of overweight and obesity4, 5. Not studies, however, have specifically examined how educational level relates to overweight and obesity, and how this association may have changed over time. An important consideration refers to the fact that women of reproductive age have experienced major changes in reproductive behaviour during the last decades, such as dramatic declines in fertility rates and parity, increases in age at first birth, and a general decrease in breastfeeding practices6-8. These changes have differentially affected women from different educational background, and they may have occurred at different pace among women in different countries. To our knowledge, no studies have examined whether these changes in reproductive behaviour may be associated with changes in overweight and obesity among women from different educational background.
Recent hypotheses suggest that parity (the number of times a female has given birth) is associated with obesity 9-11, and that total fertility rates may partly contribute to sex differences in obesity around the world 10. Physiological mechanisms proposed to explain this association include glucose alterations during pregnancy and postpartum periods, which decrease endogenous estrogens due to fewer ovulatory cycles 9. In addition, it has been argued that the increase in the amount of body fat that occurs during pregnancy may persist well beyond pregnancy 9, 10, making women with children particularly vulnerable to overweight and obesity. In principle, therefore, a reduction in fertility would be expected to lead to decreases the prevalence of overweight and obesity12, 13. However, studies indicate that lower-educated women have higher fertility and have experienced smaller reductions in fertility over time as compared to women from higher education14, 15. In combination with secular changes in diet and physical activity in low- and middle-income countries16-18, these diverging trends in fertility behaviour by educational level may have contributed to faster increases in overweight among lower-educated women.
In this study, we examine trends in overweight during the last two decades in 33 low- and middle-income countries, and estimate the potential contribution of parity, age at first birth, and duration of breastfeeding to differential trends in overweight by educational level in women of childbearing age. We hypothesised that the increasing trends in overweight in women of childbearing age have been more marked among women with lower education, and that differential trends in reproductive behaviour by education have contributed to this pattern. In particular, we hypothesised that differential trends in parity, age at first birth, and duration of breastfeeding by educational level have contributed to a larger occurrence of overweight in women with lower education in low- and middle-income countries.
METHODS
Data
We used data from the Demographic Health Survey (DHS), a cross-national household survey based on a multistage stratified cluster sampling design. The sample was selected using a stratified two- stage cluster design divided by residence areas (urban and rural) and additionally by country-specific geographic or administrative regions. Response percentages were high and ranged between 90% and 96%. The survey provides information on maternal and child health for women of reproductive age (15-49 years) and children less than 5 years. In most countries, measurements were taken every 5 years starting in the early 1990s 19. All DHS surveys were approved by the Opinion Research Corporation Company (ORC) Macro Institutional Review Board and informed consent was obtained from participants at time of interview 20. We used the publicly available version of the data available online (http://www.measuredhs.com) with no identifiable information on survey participants.
We used data for 33 countries regrouped into four regions: North Africa and West and Central Asia, South and Southeast Asia, Sub-Saharan Africa, and Latin America and the Caribbean. These countries were selected because they included information on height and weight in at least two points in time in the period 1992 to 2009. In most surveys, weight and height were only measured in women who had had at least one child during the five years prior to the survey. We therefore restricted our sample to eligible non-pregnant women aged 25-49 years who had valid data for weight and height (n= 270,202). We excluded women with missing values for height or weight, women with implausibly values for height (<100 cm or > 200cm) or weight (< 20kg or > 150kg) (n= 5,732 observations), and women with missing data for relevant covariates (n=8,642). The final sample included 255,828 women.
Body mass index
Trained personnel weighed and measured each woman between 1992 and 2009 using standardized procedures. Weight was measured using a solar powered scale (UNICEF electronic scale or Uniscale) which had a maximum capacity of 150kg and with a precision of 0.1 kg. Height was measured using an adjustable board calibrated with a precision of 0.1 cm. 20. Body Mass Index (BMI) was defined as body weight in kilograms divided by the square of height in meters. The prevalence of obesity (≥ 30 kg/m2) was very low in many of the countries included in the study. We therefore focus on overweight (>= 25 kg/m2), but using continuous BMI or obesity as outcome variable yielded similar results.
Educational level
Education was measured by asking all respondents their highest level of education completed, and the highest year completed at that level. We created 5 categories: level 1 (no education), level 2 (incomplete primary), level 3 (complete primary), level 4 (secondary) and level 5 (higher education). In supplementary analysis, we used years of schooling instead of educational level, but we do not present these results as they were qualitatively identical to those for educational level.
Reproductive variables and confounders
The key reproductive variables of interest in our study were parity, age at first birth, and duration of breastfeeding. In the majority of surveys parity was measured as the total number of children ever born. We recategorized this variable into three categories: one child, 2-3 children, and four or more children. Age at first birth was measured as a continuous variable in years. Months of breastfeeding was based on self-reports on breastfeeding of the most recent child born. About 56% of women reported that they were breastfeeding their last child at time of interview, but they did not report for how many months. For these women, we assumed that they had started breastfeeding their last child at the time of birth, and imputed duration of breastfeeding based on the current age of their last child. We categorized values for all women into not breastfeeding (less than one month), 1-12, 13-24, and >= 25 months.
Also, we incorporated age and urban versus rural residence as potential confounders of the association between education and overweight. Wealth index (http://www.measuredhs.com/topics/Wealth-Index.cfm) 21 was also included in all models as it was associated with both education and reproductive variables. Although wealth may be considered a mediator of the association between education and BMI, it may also operate as a confounder as it influences both educational opportunities, overweight and reproductive variables, particularly at younger ages.
Statistical Analysis
We used logistic regression to model overweight as a function of age, urban/rural residence, and reproductive variables. To provide an overall assessment of the association between the independent variables and overweight, we collapsed data across three time periods (1992- 1997, 1998-2003 and 2004-2009) and presented odds ratios for each region. We first examined the association between educational level and overweight controlling for age, residence area, wealth, country and year of interview. At a second stage, we examined the association between reproductive variables and overweight, and we used linear regression models to examine the association between educational level and reproductive behaviour. Subsequently, we examined whether the association between educational level and overweight was attenuated after controlling for parity, age at first birth and breastfeeding.
To examine changes in overweight over time by education, we incorporated year as a continuous variable in the logistic regression models to obtain the annual percent change (APC) in overweight in each region. To formally assess whether trends differed by educational level, we incorporated a set of interaction terms between educational level and year to obtain APC estimates for each educational level in each region. We first estimated models controlling for basic demographics only. To assess the role of reproductive behaviour, we then introduced parity, age at first birth and breastfeeding variables in the models and examined whether APC estimates changed after incorporating these variables.
All analysis was carried out using SAS 9.2 (SAS, Cary, NC, USA). Significance was considered at p < 0.05. Survey sample weights were applied in all analysis.
RESULTS
In most regions, average educational levels increased over the study period. While the proportion of those with no education ranged from 22.8% in Latin America and the Caribbean to 72% in South and Southeast Asia in 1992-1997, in the last years in 2004-2009, it ranged from 7.8% in Latin America and the Caribbean to 51% in Sub-Saharan Africa. Mean BMI increased in all regions during the 17 years of analysis. This increase was more noticeable in North Africa/West and Central Asia (26.7 kg/m2 in 1992-1997 compared to 28.5 kg/m2 in 2004-2009) followed by Latin America and the Caribbean (24.7 kg/m2 in 1992-1997 compared to 25.7 kg/m2 in 2004-2009). Likewise, the prevalence of overweight increased in all regions. Overall, women in North Africa/West and Central Asia had the highest prevalence of overweight (73.7%) in the period 2004-2009, while women in South/Southeast Asia had the lowest prevalence (13.3%). The mean of parity ranged from 3.5 to 5.1 children per woman, and decreased significantly in all regions during the observation period (Table 1).
Table 1.
Characteristics of women aged 25- 49 years by region across 33 low and middle income countries in the period 1992- 2009
| North Africa/West & Central Asia1 | South & Southeast Asia2 | Sub-Saharan Africa3 | Latin America & Caribbean4 | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1992-1997 | 1998-2003 | 2004-2009 | 1992-1997 | 1998-2003 | 2004-2009 | 1992-1997 | 1998-2003 | 2004-2009 | 1992-1997 | 1998-2003 | 2004-2009 | |||||||||||||
| Characteristics | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD | n/mean | %/ SD |
| Participants | 9719 | 3.8 | 9572 | 3.7 | 8764 | 3.4 | 3733 | 1.5 | 18,995 | 7.4 | 28,215 | 11.0 | 20,007 | 7.8 | 48,561 | 19.0 | 49,113 | 19.2 | 17,733 | 6.9 | 23,297 | 9.1 | 18,119 | 7.1 |
| BMI | 26.7 | 5.2 | 27.7 | 5.1 | 28.5 | 5.1 | 19.9 | 2.5 | 20.4 | 3.0 | 21.1 | 3.5 | 20.4 | 3.0 | 21.1 | 3.5 | 21.7 | 3.4 | 24.7 | 4.1 | 25.4 | 4.3 | 25.7 | 4.4 |
| Overweight | 5483 | 56.4 | 6410 | 67.0 | 6458 | 73.7 | 125 | 3.4 | 1417 | 7.5 | 3758 | 13.3 | 2566 | 12.8 | 7062 | 14.5 | 9631 | 19.6 | 7421 | 41.9 | 11,060 | 47.5 | 9222 | 50.9 |
| Age (years) | 32.1 | 5.4 | 31.6 | 5.2 | 32.1 | 5.4 | 30.9 | 5.2 | 30.4 | 4.9 | 30.6 | 4.8 | 32.3 | 5.7 | 32.8 | 6.0 | 32.6 | 5.9 | 32.6 | 5.7 | 32.9 | 5.8 | 32.6 | 5.6 |
| Education | ||||||||||||||||||||||||
| Non education | 3125 | 32.2 | 3066 | 32.0 | 2258 | 25.8 | 2687 | 72.0 | 9964 | 52.5 | 11,178 | 39.6 | 11,588 | 57.9 | 28,033 | 57.7 | 25,061 | 51.0 | 4035 | 22.8 | 4265 | 18.3 | 1418 | 7.8 |
| Incomplete | ||||||||||||||||||||||||
| Primary | 1271 | 13.1 | 858 | 9.0 | 709 | 8.1 | 407 | 10.9 | 2652 | 14.0 | 3590 | 12.7 | 4615 | 23.1 | 10,280 | 21.2 | 9629 | 19.6 | 5029 | 28.4 | 8016 | 34.4 | 4986 | 27.5 |
| Primary | 2205 | 22.7 | 2724 | 28.5 | 1922 | 21.9 | 473 | 12.7 | 3610 | 19.0 | 8887 | 31.5 | 3400 | 17.0 | 8100 | 16.7 | 10,648 | 21.7 | 4990 | 28.1 | 5691 | 24.4 | 5136 | 28.4 |
| Secondary | 1989 | 20.5 | 2067 | 21.6 | 2474 | 28.2 | 76 | 2.0 | 1069 | 5.6 | 1533 | 5.4 | 292 | 1.5 | 1428 | 2.9 | 2382 | 4.9 | 2012 | 11.4 | 2753 | 11.8 | 3350 | 18.5 |
| Higher | 1129 | 11.6 | 857 | 9.0 | 1401 | 16.0 | 90 | 2.4 | 1700 | 9.0 | 3027 | 10.7 | 112 | 0.6 | 720 | 1.5 | 1393 | 2.8 | 1667 | 9.4 | 2572 | 11.0 | 3229 | 17.8 |
| Parity | 4.5 | 2.7 | 3.7 | 2.3 | 3.8 | 2.1 | 4.5 | 2.2 | 4.0 | 2.2 | 3.5 | 2.0 | 5.4 | 2.6 | 5.1 | 2.6 | 5.0 | 2.5 | 4.5 | 2.8 | 4.3 | 2.7 | 3.5 | 2.3 |
| Residence | ||||||||||||||||||||||||
| Rural | 4405 | 45.3 | 4275 | 44.7 | 4542 | 51.8 | 3284 | 88.0 | 14,271 | 75.1 | 17,458 | 61.9 | 14,016 | 70.1 | 35,924 | 74.0 | 35,339 | 72.0 | 8854 | 49.9 | 11,547 | 49.6 | 7157 | 39.5 |
| Urban | 5314 | 54.7 | 5297 | 55.3 | 4222 | 48.2 | 449 | 12.0 | 4724 | 24.9 | 10,757 | 38.1 | 5991 | 29.9 | 12,637 | 26.0 | 13,774 | 28.1 | 8879 | 50.1 | 11,750 | 50.4 | 10,962 | 60.5 |
North Africa/West & Central Asia countries included (Egypt, Jordan, Kazakhstan, Turkey)
South & Southeast Asia countries included (Bangladesh, Cambodia, India, Nepal)
Sub-Saharan Africa countries included (Benin, Burkina Faso, Cameroon, Chad, Cote D'Ivoire, Ethiopia, Ghana, Guinea, Kenya, Madagascar, Malawi, Mali, Mozambique, Namibia, Niger, Nigeria, Rwanda, Tanzania, Uganda)
Latin America & Caribbean countries included (Bolivia, Colombia, Guatemala, Haiti, Nicaragua, Peru)
Educational level and overweight level and trends
The association between education and overweight differed across regions. In North Africa/West and Central Asia as well as in Latin America and the Caribbean, there was a U-shaped association between education and overweight. Women with only primary education had generally a higher prevalence of overweight than women with secondary or higher education, but prevalence in women with incomplete primary or lower education was sometimes comparable or lower than that in higher educated women. In contrast, in South and Southeast Asia and Sub- Saharan Africa, lower education was consistently associated with lower overweight prevalence. Despite some fluctuations across interview years, there was not a consistent pattern of increase in inequalities in overweight by education in any region. Although there appeared to be a non-significant increase in inequalities from 1992-1997 to 1998-2003 in some regions, this was followed by a decreasing trend in inequalities between the second and the third period (Table 2).
Table 2.
Odds ratio estimates of the association of overweight (BMI ≥ 25.0 kg/m2) with educational level among women aged 25- 49 years by region across 33 low and middle income countries in the period 1992- 2009.
| Region | 1992-1997 OR (95% CI) | Period 1998-2003 OR (95% CI) | 2004-2009 OR (95% CI) |
|---|---|---|---|
| North Africa/West & Central Asiaa | |||
| Non-education | 1.10 (0.92- 1.32) | 1.17 (0.95- 1.43) | 0.84 (0.69- 1.02) |
| Incomplete Primary | 1.46 (1.20- 1.77) | 1.31 (1.04- 1.65) | 0.87 (0.69- 1.10) |
| Primary | 1.65 (1.40- 1.95) | 1.88 (1.55- 2.27) | 1.65 (1.39- 1.95) |
| Secondary | 1.33 (1.14- 1.56) | 1.34 (1.11- 1.61) | 1.23 (1.04- 1.44) |
| Higher | Reference | ||
| South & Southeast Asiab | |||
| Non-education | 0.24 (0.12- 0.48) | 0.31 (0.25- 0.39) | 0.40 (0.34- 0.47) |
| Incomplete Primary | 0.23 (0.10- 0.55) | 0.40 (0.30- 0.51) | 0.58 (0.48- 0.69) |
| Primary | 0.47 (0.24- 0.90) | 0.58 (0.48- 0.69) | 0.72 (0.64- 0.81) |
| Secondary | 0.62 (0.26- 1.52) | 0.82 (0.66- 1.03) | 0.97 (0.82- 1.14) |
| Higher | Reference | ||
| Sub-Saharan Africac | |||
| Non-education | 0.33 (0.21- 0.52) | 0.33 (0.27- 0.40) | 0.41 (0.36- 0.47) |
| Incomplete Primary | 0.48 (0.31- 0.76) | 0.50 (0.42- 0.61) | 0.54 (0.47- 0.62) |
| Primary | 0.66 (0.42- 1.02) | 0.69 (0.58- 0.83) | 0.67 (0.60- 0.76) |
| Secondary | 0.73 (0.43- 1.24) | 0.86 (0.70- 1.06) | 0.76 (0.67- 0.87) |
| Higher | Reference | ||
| Latin America & Caribbeand | |||
| Non-education | 1.40 (1.19- 1.63) | 1.29 (1.13- 1.48) | 1.35 (1.14- 1.59) |
| Incomplete Primary | 1.70 (1.49- 1.94) | 1.67 (1.50- 1.87) | 1.73 (1.55- 1.95) |
| Primary | 1.69 (1.50- 1.90) | 1.85 (1.67- 2.05) | 1.74 (1.57- 1.93) |
| Secondary | 1.36 (1.20- 1.55) | 1.35 (1.22- 1.51) | 1.39 (1.26- 1.54) |
| Higher | Reference |
Variables included in the model: age, household wealth, residence, country and time period
North Africa/West & Central Asia countries included (Egypt, Jordan, Kazakhstan, Turkey)
South & Southeast Asia countries included (Bangladesh, Cambodia, India, Nepal)
Sub-Saharan Africa countries included (Benin, Burkina Faso, Cameroon, Chad, Cote D'Ivoire, Ethiopia, Ghana, Guinea, Kenya, Madagascar, Malawi, Mali, Mozambique, Namibia, Niger, Nigeria, Rwanda, Tanzania, Uganda)
Latin America & Caribbean countries included (Bolivia, Colombia, Guatemala, Haiti, Nicaragua, Peru)
Supplementary figure 1 shows the annual percent change in the prevalence of overweight for each educational level controlling for demographics. Overweight has increased consistently in all regions, and across all educational groups. In North Africa/West and Central Asia and Latin America and the Caribbean, increases in overweight were larger among those with lower education, and were smallest among those with higher education. In contrast, in South and Southeast Asia and Sub- Saharan Africa, overweight has increased at a similar pace in all education groups. As a result, those with lower education had consistently lower prevalence of overweight over the entire study period.
Educational level and reproductive behaviour
The relationship between parity and educational level for each region shows that in all regions, lower education was associated with higher parity, and in most cases, a larger decrease in parity seems to have occurred in the lower educated groups (Supplementary figure 2). Higher education was associated with higher age at first birth. Overall, the mean age at first birth was about 5 years higher in women with post-secondary education compared with women with no education (Supplementary figure 3). In addition, lower education was associated with significantly higher duration of breastfeeding in all regions, and this association remained over the study period. In Latin America and the Caribbean and North Africa/West and Central Asia, mean duration of breastfeeding increased over the study period, while this trend was less clear in other regions (Supplementary figure 4).
The association between reproductive behaviour and overweight
Before examining the contribution of reproductive behaviour to differences in overweight by education, we assessed the independent association between reproductive variables and overweight. In all regions except South and Southeast Asia, women who had had four children or more had an increased likelihood of overweight as compared with women who had had only one child, without adjusting for age at first birth and breastfeeding. In Latin America and the Caribbean women who had had four children or more had 52% (Odds Ratio [OR] =1.52, 95% confidence interval [CI] 1.43, 1.63) higher odds of having overweight than women who had had only one child. In contrast, in South and Southeast Asia, those who had had four children or more had reduced odds of overweight compared to women who had had only one child (OR=0.76, 95%CI 0.67, 0.87). In models that controlled for age at first birth and breastfeeding, associations between parity and overweight were substantially attenuated, but remained significant in most analyses. In fully adjusted models, higher age at first birth was associated with reduced odds of overweight, with the strongest association observed in Latin America and the Caribbean (OR=0.96, 95%CI 0.96, 0.97). In all regions except North Africa/West and Central Asia, no or shorter breastfeeding was associated with increased odds of overweight. In fully adjusted models for South and Southeast Asia, women who did not breastfed their last child had a 55% higher odds (OR=1.55, 95%CI1.33-1.81) of overweight compared with women that breasted for 13 to 24 months (Table 3).
Table 3.
Odds ratio estimates of the association of overweight (BMI ≥ 25.0 kg/m2) with parity, age at first birth and breastfeeding among women aged 25- 49 years by region across 33 low and middle income countries in the period 1992- 2009.
| Models | North Africa/West & Central Asiaa OR (95% CI) | South & Southeast Asiab OR (95% CI) | Sub-Saharan Africac OR (95% CI) | Latin America & Caribbeand OR (95% CI) |
|---|---|---|---|---|
| Model 1 | ||||
| 1 child | Reference | |||
| 2-3 Children | 1.23 (1.12- 1.34) | 1.05 (0.95- 1.16) | 1.24 (1.15- 1.34) | 1.44 (1.36- 1.52) |
| > 4 Children | 1.27 (1.15- 1.41) | 0.76 (0.67- 0.87) | 1.37 (1.27- 1.49) | 1.52 (1.43- 1.63) |
| Model 2 | ||||
| Age at first birth | 0.98 (0.97- 0.99) | 1.00 (0.99- 1.01) | 0.97 (0.97- 0.98) | 0.96 (0.96- 0.96) |
| Model 3 | ||||
| Never breastfeeding | 1.03 (0.92- 1.15) | 1.53 (1.31- 1.78) | 1.23 (1.13- 1.33) | 1.28 (1.18- 1.39) |
| 1- 12 months | 0.92 (0.86- 0.97) | 1.06 (0.98- 1.15) | 1.11 (1.07- 1.15) | 1.09 (1.05- 1.13) |
| 13- 24 months | Reference | |||
| > 25 months | 0.87 (0.77- 0.99) | 1.06 (0.97- 1.16) | 0.86 (0.81- 0.92) | 1.24 (1.17- 1.32) |
| Full Model | ||||
| 1child | Reference | |||
| 2- 3 Children | 1.15 (1.05- 1.27) | 0.99 (0.88- 1.11) | 1.12 (1.03- 1.21) | 1.19 (1.12- 1.27) |
| > 4 Children | 1.13 (0.99- 1.28) | 0.67 (0.56- 0.79) | 1.11 (1.01- 1.22) | 1.07 (0.99- 1.17) |
| Age at first birth | 0.98 (0.98- 0.99) | 0.98 (0.97- 1.00) | 0.98 (0.97- 0.99) | 0.96 (0.96- 0.97) |
| Never breastfeeding | 1.05 (0.94- 1.18) | 1.55 (1.33- 1.81) | 1.24 (1.14- 1.34) | 1.32 (1.22- 1.43) |
| 1- 12 months | 0.93 (0.87- 0.98) | 1.08 (0.99- 1.17) | 1.12 (1.08- 1.16) | 1.10 (1.06- 1.15) |
| 13- 24 months | Reference | |||
| > 25 months | 0.87 (0.76- 0.98) | 1.04 (0.95- 1.14) | 0.85 (0.80- 0.91) | 1.23 (1.15- 1.30) |
Variables included in the model 1: parity, age, household wealth, residence, country time period and educational level.
Variables included in the model 2: age at first birth, age, household wealth, residence, country, time period and educational level.
Variables included in the model 3: months of breastfeeding, age, household wealth, residence, country, time period and educational level.
Variables included in the full model: parity, age at first birth, months of breastfeeding, age, household wealth, residence, country, time period and educational level.
North Africa/West & Central Asia countries included (Egypt, Jordan, Kazakhstan, and Turkey)
South & Southeast Asia countries included (Bangladesh, Cambodia, India, and Nepal)
Sub-Saharan Africa countries included (Benin, Burkina Faso, Cameroon, Chad, Cote D'Ivoire, Ethiopia, Ghana, Guinea, Kenya, Madagascar, Malawi, Mali, Mozambique, Namibia, Niger, Nigeria, Rwanda, Tanzania, and Uganda)
Latin America & Caribbean countries included (Bolivia, Colombia, Guatemala, Haiti, Nicaragua, Peru)
The role of reproductive behaviour in explaining the link between educational level and overweight
Associations between educational level and overweight shown Table 2 did not change after controlling for reproductive variables (Table 4). In South and Southeast Asia and Sub- Saharan Africa, women with lower educated had lower overweight prevalence than women with higher education, while in North Africa/West, Central Asia, Latin America and the Caribbean, there was a U-shaped association between education and overweight.
Table 4.
Odds ratio estimates of the association of overweight (BMI ≥ 25.0 kg/m2) with educational level controlling for reproductive variables among women aged 25- 49 years by region across 33 low and middle income countries in the period 1992- 2009.
| Region | Period | ||
|---|---|---|---|
| 1992-1997 | 1998-2003 | 2004-2009 | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| North Africa/West & Central Asiaa | |||
| Non-education | 0.98 (0.81- 1.19) | 1.04 (0.84- 1.29) | 0.81 (0.66- 0.99) |
| Incomplete Primary | 1.32 (1.08-1.61) | 1.19 (0.94- 1.51) | 0.82 (0.65- 1.05) |
| Primary | 1.52 (1.29- 1.81) | 1.71 (1.41- 2.08) | 1.59 (1.33- 1.89) |
| Secondary | 1.27 (1.08- 1.50) | 1.28 (1.06- 1.54) | 1.20 (1.02- 1.41) |
| Higher | Reference | ||
| South & Southeast Asiab | |||
| Non-education | 0.20 (0.09- 0.45) | 0.34 (0.26- 0.43) | 0.44 (0.37- 0.52) |
| Incomplete Primary | 0.19 (0.07- 0.48) | 0.42 (0.32- 0.55) | 0.61 (0.51- 0.74) |
| Primary | 0.38 (0.18- 0.80) | 0.59 (0.49- 0.72) | 0.74 (0.66- 0.84) |
| Secondary | 0.54 (0.21- 1.35) | 0.83 (0.66- 1.05) | 0.97 (0.82- 1.15) |
| Higher | Reference | ||
| Sub-Saharan Africac | |||
| Non-education | 0.28 (0.18- 0.45) | 0.27 (0.22- 0.33) | 0.37 (0.32- 0.42) |
| Incomplete Primary | 0.41 (0.26- 0.65) | 0.42 (0.34- 0.50) | 0.49 (0.42- 0.56) |
| Primary | 0.59 (0.37- 0.92) | 0.59 (0.49- 0.71) | 0.62 (0.55- 0.70) |
| Secondary | 0.70 (0.41- 1.19) | 0.82 (0.66- 1.01) | 0.73 (0.64- 0.84) |
| Higher | Reference | ||
| Latin America & Caribbeand | |||
| Non-education | 1.13 (0.95- 1.33) | 1.05 (0.91- 1.21) | 1.06 (0.89- 1.26) |
| Incomplete Primary | 1.40 (1.22- 1.62) | 1.39 (1.24- 1.56) | 1.39 (1.23- 1.58) |
| Primary | 1.44 (1.27- 1.63) | 1.57 (1.41- 1.75) | 1.44 (1.29- 1.60) |
| Secondary | 1.26 (1.11- 1.43) | 1.24 (1.11- 1.38) | 1.26 (1.13- 1.39) |
| Higher | Reference | ||
Variables included in the adjusted model: age, household wealth, residence, country, time period, parity, age at first birth and breastfeeding.
North Africa/West & Central Asia countries included (Egypt, Jordan, Kazakhstan, Turkey)
South & Southeast Asia countries included (Bangladesh, Cambodia, India, Nepal)
Sub-Saharan Africa countries included (Benin, Burkina Faso, Cameroon, Chad, Cote D'Ivoire, Ethiopia, Ghana, Guinea, Kenya, Madagascar, Malawi, Mali, Mozambique, Namibia, Niger, Nigeria, Rwanda, Tanzania, Uganda)
Latin America & Caribbean countries included (Bolivia, Colombia, Guatemala, Haiti, Nicaragua, Peru)
Figure 1 shows odds ratios that compare the prevalence of overweight between women with lower education to that in women with highest education separately for each country. Estimates from model 1 are adjusted for demographics (model 1), while those in model 2 adjust for both demographics and reproductive variables (model 2). In Sub- Saharan Africa and South and Southeast Asia, where most DHS countries were located, lower education was associated with a lower prevalence of overweight. In contrast, in most populations in Latin America and the Caribbean, as well as North Africa/West and Central Asia, lower education was associated with a higher prevalence of overweight. Overall, associations between educational level and overweight were very similar between models that controlled for demographics only, as compared to estimates from models that controlled for both demographics and reproductive behavior.
Figure 1.
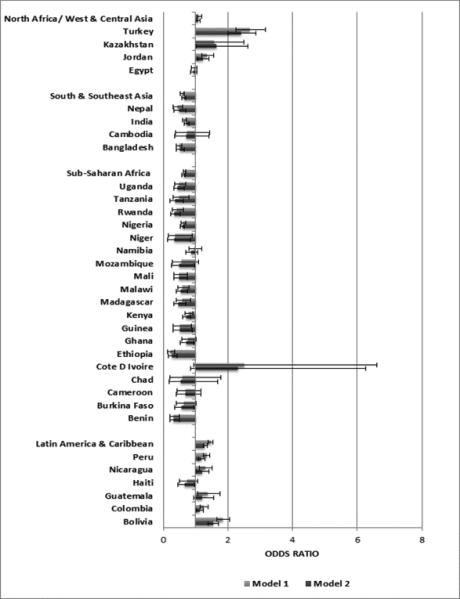
Odds ratios of the effect of lowest educational level compare with the highest on overweight among women aged 25-49 years by region across 33 low and middle income countries in the period 1992-2009.
Figure 2 shows the annual percent change in the prevalence of overweight for each educational level controlling for demographics and reproductive behaviour. Results are almost identical to those in Supplementary Figure 1, and suggest that independently of changes in reproductive behaviour, overweight has increased consistently in all regions, and across all educational groups. These findings suggest that trends in reproductive behaviour do not explain trends in overweight among women from different educational background.
Figure 2.
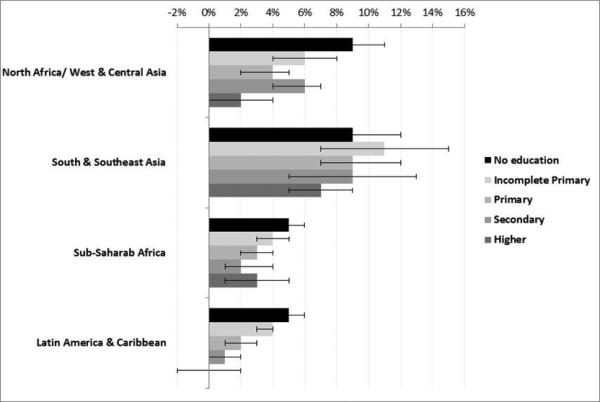
Annual percent change in the odds of overweight among women aged 25- 49 years by educational level and region across 33 low and middle income countries in the period 1992-2009
DISCUSSION
Results from this study suggest that the association between educational level and overweight varies substantially across regions. As compared to having secondary education or higher, having only primary education is associated with higher overweight prevalence in North Africa/West and Central Asia as well as in Latin America and the Caribbean. In contrast, in South and Southeast Asia as well as in Sub- Saharan Africa, lower education is associated with lower prevalence of overweight. Nevertheless, the prevalence of overweight has increased in all regions and it has done so across all educational groups. We find no evidence of a significant shift in the association between education and overweight in the period 1992-2009, although increases in overweight prevalence have generally been larger in those with lower education in some regions. Reproductive variables do not seem to play a role in explaining trends in overweight by educational level during the last decades.
Studies conducted the early 1990's suggested that higher wealth or income were associated with higher prevalence of overweight and obese in developing countries14, 18, 21-23. Nonetheless, consistently with our results, recent evidence shows that women with lower education had a 40% higher prevalence of overweight than women with higher education in some developing countries5, 24. Previous studies based on a single cross-sectional measurement have suggested that middle- and low-income countries are experiencing an epidemiological transition characterized by increases in body mass index, and a shift from a positive to a negative association between income and BMI due to larger increases in the lower income groups 21, 23. Our results suggest that this pattern does not hold in all countries when using education as indicator of socioeconomic status. In South and Southeast Asia, as well as in Sub- Saharan Africa we observed the same positive association for education as reported for income and wealth. In contrast, in Latin America and the Caribbean and North Africa/West and Central Asia, we find that more schooling seems to protect against overweight. These discrepancies may suggest that education represents a different human capital stock than wealth and income, so that even in societies where higher income and wealth are associated with higher BMI, education may still have a protective effect. This may relate to the specific mechanisms through which education relates to overweight, which may not be the same as those for income and wealth.
A possible explanation for the observation that in low-income countries, lower education is associated with lower prevalence of overweight is that education may be strongly linked with under nutrition and high physical activity at work, as well as a reduced availability of certain foods. In contrast, in middle income countries, the recent transition towards a market economy characterized by trade liberalization may have increased intake of energy-dense foods 25, 26. Globally, food consumption per person has been increased almost 400 kcal per person per day from 2411 in 1969/1971 to 2789 kcal in 1999/200126. However, this rise is associated to a large extent with increased consumption of fat and sugars17, 27, 28. For example, in the last 40 years, China experienced major increases in vegetable oil, meat and sugar intake, paired with a decline in the consumption of tubers and roots in the same period26”. In addition, urban populations are increasingly exposed to processed energy-dense foods that may affect the association between education and overweight4. In sensitivity analyses, we found that in all regions, living in urban areas was associated with a significantly higher risk of overweight as compared with living in rural areas, most markedly for South/Southeast Asia and Sub-Saharan Africa regions. In the Sub-Saharan Africa region, for example, women who lived in urban areas had 74% higher odds (OR=1.74, 95%CI 1.67-1.82) of overweight compared with women lived in rural areas. Thus, urbanization remains an important potential driver of trends in overweight to be explored in future studies.
We found that overweight increased consistently in all educational groups within each region. In some regions, increases in overweight were larger in those with lower education, although this pattern has so far been insufficient to generate a consistent shift in the association between education and overweight. More favorable trends in women from higher education in some countries may be explained partly by their higher levels of health awareness, and their healthier diets characterized by greater intake of fruits and vegetables 6. The highest educated may also have greater access to health information and more choice regarding physical activity26, 29. On the other hand, other risk factors for overweight such as access to a high-fat diet and more sedentary occupations may be more common in highly educated women, while women in lower educated groups may maintain low-fat diets and work in occupations with higher levels of physical activity 28, 30. These compensating forces may have resulted in similar increases in overweight in all educational groups.
Variations across regions and countries may also be explained by differences in social and cultural values. In some Asian countries, body size has been associated with opulence and wealth31, while the opposite may be true in Latin America and the Caribbean, potentially leading to different patterns of behaviour32. In some studies, obese persons have reported high levels of stigmatization and discrimination that specifically affect more women than men33, 34. The consequences of stigma have been linked with less likelihood of completing schooling, finding a partner, and have better household incomes35. These mechanisms may differ across countries and regions, partly contributing to the cross-national variations in the link between education and overweight.
Our results suggest that reproductive variables are associated with overweight prevalence among women aged 25-49 years, and that this association holds for women in a wide range of low- and middle-income countries. This is consistent with previous studies reporting a positive association between parity and body size 7, 11, 14, 36-39, hypothesising this to be the result of cumulative cycles of pregnancy weight gain and postpartum weight retention 7, 14. In contrast, breastfeeding could be a protective factor against overweight. A previous study suggested that breastfeeding for more than 6 months is associated with lower BMI and may be beneficial to control long-term weight 40. Similarly, a US study found that breastfeeding for more than 12 months was associated with decreased odds of obesity 11. Our results are consistent with these findings.
Contrary to our hypotheses, trends in reproductive behaviour did not explain the increasing trends in overweight in all educational groups. While there have been substantial changes in reproductive behaviour, inequalities in overweight by education have remained relatively constant. Several explanations may account for this finding. Reproductive variables in our study may not have a strong impact on overweight in middle- and low-income countries. In addition, decreases in parity and increases in the age at first birth appear to have occurred in some educational groups. If anything, the lower educated may have experienced a larger increase in breastfeeding and a larger decrease in parity, potentially leading to smaller increases in overweight. The fact that we have not observed this pattern suggests that other factors such as diet and physical activity may be stronger drivers of trends in overweight.
We found that parity, age at first birth and breastfeeding explained part of the association between education and BMI in Latin America and the Caribbean, but not in other regions. This may be due to a larger effect of education on reproductive behaviour for women in Latin America and the Caribbean. A possible explanation for this is a differential impact of education on labour force participation in this region, with highly educated women entering the labour market at disproportionately higher rates as compared to highly educated women in other regions. This may have led to a larger association between education and reproductive behaviour among Latin American women, which could potentially have translated into larger effects of education on overweight. Although preliminary, these findings may suggest that differences in labour force participation by education may have contributed to differences in reproductive behaviour, which may in turn have led to differences in overweight among women.
Limitations
Despite several strengths of the DHS data, some limitations of our study should be considered. We were unable to introduce details of the context and other variables that are relevant. However our study offers a first glance of how key reproductive variables are related to inequalities in BMI and overweight. Our observations are limited to women between the ages of 25 to 49 years. Although DHS provides comparable data for many countries, our results are limited to women aged 25–49 years who had recently had children and are therefore not generalizable to all women of reproductive age. However, among all women aged 25–49 years in countries participating in DHS, the proportion having at least one fertile pregnancy ranged from 93.6% in the Central African Republic to 99% in Bolivia, suggesting that our results cover most women in this age range41.
Misclassification of educational level is another potential source of bias. Individuals may report education differently across countries, and reclassification of national levels into an internationally comparable classification may not be accurate. Nevertheless, we used broad categories instead of very specific levels to diminish the potential bias associated with misclassification. In addition, misclassification in the measurement of reproductive variables may be a larger concern for some variables, particularly for breastfeeding. Many women were still breastfeeding at time of interview so that total duration was not observed, and some women may have reported duration inaccurately.
We used multiple cross-sectional assessments, but DHS does not follow participants over time so that assessments of individual weight change were not possible. In addition, we had no data on BMI before pregnancy and we could not establish the temporal ordering between reproductive variables, overweight, and education. Reproductive variables may have a causal effect on both educational achievements and BMI, thus operating as confounders. However, education may also have a causal impact on reproductive variables and through this pathway influence BMI. The causal pathways explaining associations can only be assessed with longitudinal data.
Our models incorporated wealth as a covariate, because we conceptualized wealth as a potential confounder of the association between educational level and overweight. However, wealth may also be a mediator in the pathway between educational level and overweight, so that controlling for wealth may have removed part of the effect of education on overweight mediated by wealth. In a sensitivity analysis (supplementary table 1), we found that the association between educational level and overweight in South and Southeast Asia and Sub-Saharan Africa was somewhat attenuated, but remained similar between models without wealth and models that incorporated wealth, whereby lower education was associated with lower overweight prevalence. In North Africa/West & Central Asia and Latin America & Caribbean, in models without controlling for wealth, women with none or only primary education had lower odds of overweight compared with their higher educated counterparts. After controlling for wealth, the net effect of education reversed so that women with none or only primary education had higher overweight compared to higher educated women in most periods. Overall, we emphasized our results from models controlling for wealth, as educational attainment is strongly influenced by pre-existing wealth levels in low- and middle-income countries42, so that wealth remains a major confounder. Accumulated wealth may become more important at older ages, but in this relatively young cohort of women, wealth may to a large extent reflect parental family resources that influenced educational achievement43. Controlling for wealth, therefore, was important to isolate the association between education and overweight, net of wealth. Nevertheless, our conclusions on the role of reproductive behaviour in explain trends in overweight across educational groups did not change regardless of whether wealth was included in the models (supplementary table 1).
Conclusion
Previous studies in low- and middle-income countries have argued that overweight remains concentrated in higher socioeconomic groups 5, 24. Although this is true for South/Southeast Asia and Sub-Saharan Africa, we find that in North Africa West/Central Asia and Latin American lower education was generally associated with higher overweight prevalence. Furthermore, overweight prevalence has increased consistently in all regions and across all educational groups in the period 1992-2009, suggesting that increasing overweight trends do not only affect the higher socioeconomic groups. However, trends in reproductive behaviour did not explain trends in overweight by educational level. Our results raise the need to understand the causes of increasing trends in overweight, and emphasize the need to focus overweight and obesity prevention efforts across all levels of society.
Supplementary Material
Acknowledgements
Sandra Lopez-Arana was supported by the European Union Erasmus Mundus Partnerships program Erasmus-Columbus (ERACOL) at Erasmus MC in the Netherlands. Mauricio Avendano was supported by a Starting Researcher grant from the European Research Council (ERC) (grant No 263684), a fellowship from Erasmus University Rotterdam and a grant from the National Institute of Ageing (R01AG037398).
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Authors‘ contributions: Design (Sandra Lopez- Arana, Mauricio Avendano), data analysis (Sandra Lopez- Arana, Mauricio Avendano), interpretation of the results (Sandra Lopez- Arana, Mauricio Avendano, Alex Burdorf), manuscript preparation (Sandra Lopez- Arana), manuscript review (Sandra Lopez- Arana, Mauricio Avendano, Alex Burdorf),
REFERENCES
- 1.Finucane MM, Stevens GA, Cowan MJ, et al. National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet. 2011;377:557–67. doi: 10.1016/S0140-6736(10)62037-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Swinburn BA, Sacks G, Hall KD, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378:804–14. doi: 10.1016/S0140-6736(11)60813-1. [DOI] [PubMed] [Google Scholar]
- 3.IASO Global prevalence of adult overweight and obesity by region. International Association for the study of obesity. 2013 [Google Scholar]
- 4.Shankar B. Socio-economic drivers of overnutrition in China. J Hum Nutr Diet. 2010;23:471–9. doi: 10.1111/j.1365-277X.2009.01035.x. [DOI] [PubMed] [Google Scholar]
- 5.Subramanian SV, Perkins JM, Ozaltin E, Davey Smith G. Weight of nations: a socioeconomic analysis of women in low- to middle-income countries. Am J Clin Nutr. 2011;93:413–21. doi: 10.3945/ajcn.110.004820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Barros FC, Victora CG, Scherpbier R, Gwatkin D. Socioeconomic inequities in the health and nutrition of children in low/middle income countries. Rev Saude Publica. 2010;44:1–16. doi: 10.1590/s0034-89102010000100001. [DOI] [PubMed] [Google Scholar]
- 7.Kim SA, Stein AD, Martorell R. Country development and the association between parity and overweight. Int J Obes (Lond) 2007;31:805–12. doi: 10.1038/sj.ijo.0803478. [DOI] [PubMed] [Google Scholar]
- 8.Kulie T, Slattengren A, Redmer J, Counts H, Eglash A, Schrager S. Obesity and Women's Health: An Evidence-Based Review. J Am Board Fam Med. 2011;24:75–85. doi: 10.3122/jabfm.2011.01.100076. [DOI] [PubMed] [Google Scholar]
- 9.Bastian LA, West NA, Corcoran C, Munger RG. Cache County Study on Memory H, Aging. Number of children and the risk of obesity in older women. Prev Med. 2005;40:99–104. doi: 10.1016/j.ypmed.2004.05.007. [DOI] [PubMed] [Google Scholar]
- 10.Brooks R, Maklakov A. Sex differences in obesity associated with total fertility rate. PLoS One. 2010;5:e10587. doi: 10.1371/journal.pone.0010587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cohen SS, Larson CO, Matthews CE, et al. Parity and breastfeeding in relation to obesity among black and white women in the southern community cohort study. J Womens Health (Larchmt) 2009;18:1323–32. doi: 10.1089/jwh.2008.1181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Castro-Martin T. Women's Education and Fertility: Results from 26 Demographic and Health Surveys. Stud Fam Plann. 1995;26 [PubMed] [Google Scholar]
- 13.Popkin BM. The nutrition transition in low-income countries: an emerging crisis. Nutr Rev. 1994;52:285–98. doi: 10.1111/j.1753-4887.1994.tb01460.x. [DOI] [PubMed] [Google Scholar]
- 14.Kim SA, Yount KM, Ramakrishnan U, Martorell R. The relationship between parity and overweight varies with household wealth and national development. Int J Epidemiol. 2007;36:93–101. doi: 10.1093/ije/dyl252. [DOI] [PubMed] [Google Scholar]
- 15.Silva S, Hotchkiss DR. How does the spread of primary and secondary schooling influence the fertility transition? Evidence from rural Nepal. J Biosoc Sci. FirstView. 2013:1–31. doi: 10.1017/S0021932013000096. [DOI] [PubMed] [Google Scholar]
- 16.Kain J, Vio F, Albala C. Obesity trends and determinant factors in Latin America. Cad Saude Publica. 2003;19(Suppl 1):S77–86. doi: 10.1590/s0102-311x2003000700009. [DOI] [PubMed] [Google Scholar]
- 17.Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70:3–21. doi: 10.1111/j.1753-4887.2011.00456.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sobal J, Stunkard AJ. Socioeconomic status and obesity: a review of the literature. Psychol Bull. 1989;105:260–75. doi: 10.1037/0033-2909.105.2.260. [DOI] [PubMed] [Google Scholar]
- 19.Rutstein SO, Rojas G. Guide to DHS statistics. ORC Macro; Calverton, MD: 2006. [Google Scholar]
- 20.ICF I. Survey Organization Manual for Demographic and Health Surveys. In: DHS M, editor. ICF International. Maryland; Calverton: 2012. [Google Scholar]
- 21.Rutstein SO, Johnson K. The DHS Wealth Index. ORC Macro; Calverton, MD: 2004. [Google Scholar]
- 22.Mendez MA, Monteiro CA, Popkin BM. Overweight exceeds underweight among women in most developing countries. Am J Clin Nutr. 2005;81:714–21. doi: 10.1093/ajcn/81.3.714. [DOI] [PubMed] [Google Scholar]
- 23.Subramanian SV, Finlay JE, Neuman M. Global trends in body-mass index. Lancet. 2011;377:1915–16. doi: 10.1016/S0140-6736(11)60803-9. [DOI] [PubMed] [Google Scholar]
- 24.Jones-Smith JC, Gordon-Larsen P, Siddiqi A, Popkin BM. Is the burden of overweight shifting to the poor across the globe? Time trends among women in 39 lowand middle-income countries (1991-2008). Int J Obes (Lond) 2012;36:1114–20. doi: 10.1038/ijo.2011.179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Monteiro CA, Conde WL, Popkin BM. Independent Effects of Income and Education on the Risk of Obesity in the Brazilian Adult Population. J Nutr. 2001;131:881S–86S. doi: 10.1093/jn/131.3.881S. [DOI] [PubMed] [Google Scholar]
- 26.Kearney J. Food consumption trends and drivers. Philos Trans R Soc Lond B Biol Sci. 2010;365:2793–807. doi: 10.1098/rstb.2010.0149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Martorell R, Khan LK, Hughes ML, Grummer-Strawn LM. Obesity in women from developing countries. Eur J Clin Nutr. 2000;54:247–52. doi: 10.1038/sj.ejcn.1600931. [DOI] [PubMed] [Google Scholar]
- 28.Popkin BM. The nutrition transition: an overview of world patterns of change. Nutr Rev. 2004;62:S140–3. doi: 10.1111/j.1753-4887.2004.tb00084.x. [DOI] [PubMed] [Google Scholar]
- 29.Case A, Menendez A. Sex differences in obesity rates in poor countries: evidence from South Africa. Econ Hum Biol. 2009;7:271–82. doi: 10.1016/j.ehb.2009.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Monteiro CA, Moura EC, Conde WL, Popkin BM. Socioeconomic status and obesity in adult populations of developing countries: a review. Bull World Health Organ. 2004;82:940–6. [PMC free article] [PubMed] [Google Scholar]
- 31.Hermann S, Rohrmann S, Linseisen J, et al. The association of education with body mass index and waist circumference in the EPIC-PANACEA study. BMC Public Health. 2011;11:169. doi: 10.1186/1471-2458-11-169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.McLaren L. Socioeconomic status and obesity. Epidemiologic reviews. 2007;29:29–48. doi: 10.1093/epirev/mxm001. [DOI] [PubMed] [Google Scholar]
- 33.Chen EY, Brown M. Obesity stigma in sexual relationships. Obes Res. 2005;13:1393–7. doi: 10.1038/oby.2005.168. [DOI] [PubMed] [Google Scholar]
- 34.Muennig P. The body politic: the relationship between stigma and obesity-associated disease. BMC Public Health. 2008;8:128. doi: 10.1186/1471-2458-8-128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Gortmaker SL, Must A, Perrin JM, Sobol AM, Dietz WH. Social and economic consequences of overweight in adolescence and young adulthood. N Engl J Med. 1993;329:1008–12. doi: 10.1056/NEJM199309303291406. [DOI] [PubMed] [Google Scholar]
- 36.Bastian LA. Impact of parity and breastfeeding on racial differences in obesity. J Womens Health (Larchmt) 2009;18:1311–2. doi: 10.1089/jwh.2009.1569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Coitinho DC, Sichieri R, D'Aquino Benicio MH. Obesity and weight change related to parity and breast-feeding among parous women in Brazil. Public Health Nutr. 2001;4:865–70. doi: 10.1079/phn2001125. [DOI] [PubMed] [Google Scholar]
- 38.Mishra G, Kuh D. Commentary: The relationship between parity and overweight—a life course perspective. Int J Epidemiol. 2007;36:102–03. doi: 10.1093/ije/dyl285. [DOI] [PubMed] [Google Scholar]
- 39.Villamor E, Cnattingius S. Interpregnancy weight change and risk of adverse pregnancy outcomes: a population-based study. Lancet. 2006;368:1164–70. doi: 10.1016/S0140-6736(06)69473-7. [DOI] [PubMed] [Google Scholar]
- 40.Rooney BL, Schauberger CW. Excess pregnancy weight gain and long-term obesity: one decade later. Obstet Gynecol. 2002;100:245–52. doi: 10.1016/s0029-7844(02)02125-7. [DOI] [PubMed] [Google Scholar]
- 41.Rutstein SO, Shah IH. DHS Comparative Reports N 9. ORC Macro and the World Health Organization; Calverton, Maryland: 2004. Infecundity, Infertility, and Childlessness in Developing Countries. [Google Scholar]
- 42.Hruschka DJ, Brewis AA. Absolute wealth and world region strongly predict overweight among women (ages 18-49) in 360 populations across 36 developing countries. Econ Hum Biol. 2012 doi: 10.1016/j.ehb.2012.01.001. [DOI] [PubMed] [Google Scholar]
- 43.Galobardes B, Shaw M, Lawlor DA, Lynch JW, Davey Smith G. Indicators of socioeconomic position (part 1). J Epidemiol Community Health. 2006;60:7–12. doi: 10.1136/jech.2004.023531. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.