

Abstract
Plans of patients with prostate tumor have been studied. These patients have been scanned in the CT simulator and the images have been sent to the Focal, the system where the doctor delineates the tumor and the organs at risk. After that in the treatment planning system XiO there are created for the same patients three dimensional conformal and intensity modulated radiotherapy treatment plans. The planes are compared according to the dose volume histograms. It is observed that the plans with IMRT technique conform better the isodoses to the planning target volume and protect more the organs at risk, but the time needed to create such plans and to control it is higher than 3D CRT. So it necessary to decide in which patients to do one or the other technique depending on the full dose given to PTV and time consuming in genereral.
Key words: treatment planning system, organ at risk, radiation dose, dose volume histogram.
1. INTRODUCTION
Radiotherapy aims to give the prescribed dose to the tumor and to protect as much as possible the organs at risk and surrounded healthy tissue. The radiotherapy nowadays, together with chemotherapy and surgery, is a way to treat the patients which have different kind of tumors. Intensity-modulated radiation therapy (IMRT) is an advanced technique of high-precision radiotherapy that uses computer-controlled linear accelerator to deliver precise radiation doses to a malignant tumor or specific areas within the tumor. IMRT allows for the radiation dose to conform more precisely to the three-dimensional (3-D) shape of the tumor by modulating or controlling the intensity of the radiation beam in multiple small volumes. Also it allows higher radiation doses to be focused to regions within the tumor while minimizing the dose to surrounding normal critical structures (1). The process of radiotherapy starts with scanning of the patients, delineating areas of interest, creating the treatment plans and sending all the data to the machine through a verification system, mosaiq. An important part of this chain is the plan which is created in the treatment planning system. This system is able to create 3D CRT and IMRT plans. Even the all process of these two techniques is similar the design plan differs significantly. Conventional 3D CRT treatment planning is manually optimized (2). This means that the treatment planner chooses all beams parameters, such as the number of beams, beam directions, shapes, weights etc., and the computer calculates the resulting dose distribution (3). In the case of IMRT dose distribution is inversely determined, meaning that the treatment planner has to decide before the dose distribution he wants and the computer then calculates a group of beam intensities that will be produced, as nearly as possible, the desired dose distribution (4). It is necessary to compare and to know advantages and disadvantages of these two methods, and so to choose the right method for every single patient.
2. METHODS AND MATERIALS
In this study are taken into account five patients with prostate tumors. The patients are scanned in the CT simulator. They are positioning with the help of immobilization devices such as prostep and knee fix in the supine positions. On the body are putted three orientated points in the crosses of lasers’ room. These are some kind of tattoo. The slices’ thickness is 3 mm and then the images are sanded to the Focal. The Focal is the system where the doctors delineate the target volumes and the organs at risk. Then the images go from Focal to the treatment planning system. Treatment planning system that is in use is XiO version 4.62, which is a family of two and three dimensional treatment plans systems. It is composed of several modules, the most important are module of patients’ data, including patient demographic and anatomic data and the teletherapy planning module.
The treatment planning system can create plans with both techniques three dimensional conformal radiotherapy and intensity modulated radiotherapy. The plans with the first technique treatment are done in two phases. In the first phase the plan is a simple box technique with four beams. Each beam has the energy 18 MV and in the second phase it is created a plan with six or more beams, again with energy 18 MV. The number of beams in the second phase is more than four in such a way to protect better the organs at risk. The beams are conformed with the help of MLC to the treatment planning volume PTV. It has to be mention that in the second phase the PTV is delineated smaller than in the first phase because of the dose limits for the organs at risk. The second technique (IMRT) is done with one phase (5). The number of beams is fixed. There are nine beams, with energy 6 MV, in different angles which are used to create the plan. All the beams are created by more small beams in order to modulate the intensity in such a way to have the desire dose distribution (6). When the plans are finished they are compared, for both methods, first according to dose-volume histogram and then according to time consuming for quality control procedures. The checks for the position of the patients, so the giving of the right dose to the right part of the body, for 3D CRT are done in the machine according to the set-up beams with the help of electronic portal imaging device (EPID) and for the IMRT it is used a device which is placed on the coach of the LINAC and connected with a software. So the first is done with the patient in the machine and the second before the entering of the patient in the machine. The time which is needed to treat the patients with the first technique is much shorter than the second technique.
3. RESULTS AND DISCUSSIONS
There are done plans with both techniques, three dimensional conformal radiotherapy and intensity modulated radiotherapy for five patients with prostate tumors. Their comparison is done first according to dose-volume histograms and then according to time consuming for QC checks. For all organs at risk the comparison is done for the mean doses which have been taken for 20 % and 50 % volume [7]. It is observed that the average doses, for all patients, are much lower in IMRT technique then in 3D CRT Fig. 1 and Fig. 2.
Figure 1.

A case of IMRT treatment plan DVH.
Figure 2.

A case of 3D CRT treatment plan DVH.
Table 1 gives a picture of such results.
Table 1.
The mean doses in Gy for 50 % and 20% of OR volume for both technique
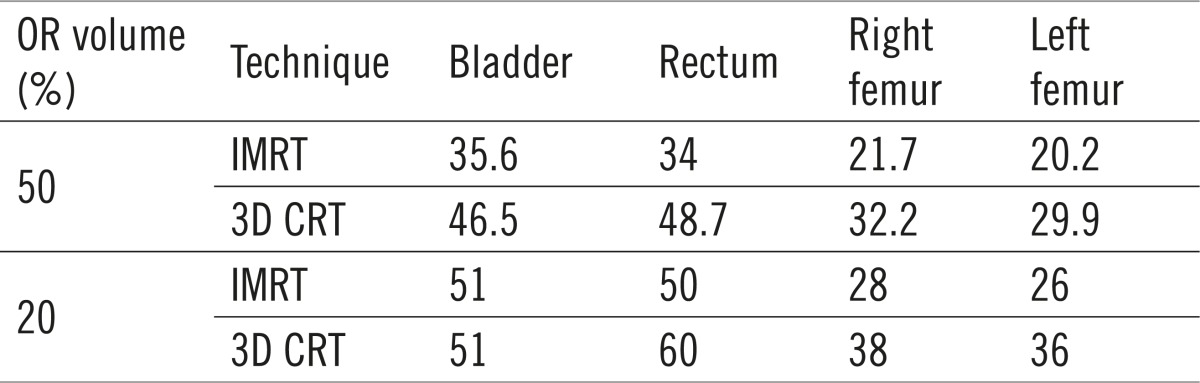 |
From the obtain histograms, Fig. 1 and Fig. 2, it is seen that the conformity to planning target volume doesn’t differ too much. Anyway a bit better conformity it is observed with the IMRT technique. Regarding to the doses to the organs at risk it is a big difference between doses taken by organs at risk in the IMRT and 3D CRT technique. So according to the histograms we can say that the IMRT technique is better for protection of the organs at risk and irradiating with the best coverage the treatment planning volume, because in the 3D CRT due to the dose limits for the organs at risk it should be irradiate first the planning target volume as the doctors delineate and then a smaller planning target volume. So in IMRT technique it is irradiated the appropriate planning target volume with the maximum protection of the organs at risk and not only a part of it.
According to the time consuming for the quality control it is needed much more time for checking the IMRT plans. With a special device connected to a software it is evaluated the isodoses in different directions, but for this it is necessary that the LINAC to be busy for a long time and so to stop the other normal treatment in the department.
4. CONCLUSIONS
The work done in this paper stresses the advantages and disadvantages of two treatment methods for prostate tumors. To choose between two techniques it is necessary to see the patients characteristics case by case. It is important the total dose which has to be given to the planning target volume. When the doctor decides to give to treatment planning volume a total dose which creates the possibility to have dose for the organs at risk under the dose limits it will be preferable to use 3D CRT technique because it is less time consuming for QC and more comfortable for the patient which in this case has to stay less time in the machine during the treatment. For the cases when the doses which have to be given to the treatment planning volume will be large, around, 70 Gy it will be use IMRT technique as the best solution for keeping the doses to organ at risk in the permitted level.
Conflict of interest
None declared.
REFERENCES
- 1.Chui CS, Chan MF, Yorke E, Spirou E, Ling CC. Delivery of Intensity-modulated radiation therapy with a conventional multileaf collimator: Comparison of dynamic and segmental methods. Med Phys. 2001;28(12):2441–2449. doi: 10.1118/1.1418018. [DOI] [PubMed] [Google Scholar]
- 2.Langer M, Leong J. Optimization of beam weight under dose-volume restrictions. Int J Radiat Oncol Biol Phys. 1987;13(8):1255–1260. doi: 10.1016/0360-3016(87)90203-3. [DOI] [PubMed] [Google Scholar]
- 3.Ezzell GA. Genetic and geometric optimization of three-dimensional radiation therapy treatment planning. Med Phys. 1996;23(3):293–305. doi: 10.1118/1.597660. [DOI] [PubMed] [Google Scholar]
- 4.Spirou SV, Chui CS. A gradient inverse planning algorithm with dosevolume constrains. Med Phys. 1998;25(3):321–333. doi: 10.1118/1.598202. [DOI] [PubMed] [Google Scholar]
- 5.Jackson A, Skwarchuk M, Leibel SA. Clinical experience with intensity modulated radiation therapy in prostate cancer. Radiother Oncol. 2000;55(3):241–249. doi: 10.1016/s0167-8140(99)00100-0. [DOI] [PubMed] [Google Scholar]
- 6.Galvin JM, Chen XG, Smith RM. Combining multileaf fields to modulate fluence distribution. Int J Radiat Oncol Biol Phys. 1993;27(3):697–705. doi: 10.1016/0360-3016(93)90399-g. [DOI] [PubMed] [Google Scholar]
- 7.Verhey LJ. Comparison of three-dimensional conformal radiation therapy and intensity-modulated radiation therapy systems. Semin Radiat Oncol. 1999;9(1):78–98. doi: 10.1016/s1053-4296(99)80056-3. [DOI] [PubMed] [Google Scholar]