

Abstract
Renal medullary carcinoma (RMC) is rare, accounting for less than 1% of all renal neoplasms. Case reports suggest RMC is highly aggressive, poorly responsive to chemotherapy, often metastatic at diagnosis, affects young men with sickle cell trait, and median overall survival (mOS) is less than 12 months. We report the epidemiological characteristics, treatments performed, response rate to each treatment and mOS of five patients with RMC. All patients had sickle cell trait, four were male, three had metastatic disease at diagnosis and mean age at diagnosis was 25 years. Non-metastatic patients were submitted to nephrectomy. Two patients had partial response to first line chemotherapy including cisplatin and gemcitabine. There was no response to sunitinib or second line chemo - therapy; mOS was 6 months. Due to its rarity, case series are the only evidence available to discuss the treatment for RMC. In our experience, only cisplatin and gemcitabine based regimen offered response.
Key words: kidney neoplasms, renal medullary carcinoma, carcinoma, renal cell, sickle cell trait
Introduction
Renal medullary carcinoma is a rare disease, accounting for less than 1% of the renal neoplasms. It is highly aggressive and more common among young men between ten and forty years. There is strong association with sickle cell trait, described in 98% of the cases.1-3 In several texts, renal medullary carcinoma is classified as a subtype of collecting duct carcinoma. However, collecting duct carcinoma typically occurs in older patients without sickle cell trait.2 Clinical features of renal medullary carcinoma include hematuria, abdominal pain, abdominal mass and weight loss.2,3 Usually, the disease is metastatic at diagnosis and is associated with a poor prognosis and overall survival of less than 12 months.1,3,4 The largest case series included only 9 patients and 6 of them received chemotherapy.1
Considering the lack of data in the literature concerning this entity, we reported our experience with patients diagnosed with renal medullary carcinoma, who received chemotherapy at Instituto do Câncer do Estado de São Paulo (Brazil). We evaluated the epidemiological characteristics, the association with sickle cell trait or sickle cell anemia, the main treatment performed, the response rate with chemotherapy, the time to progression of the disease and the overall survival of this small group of patients.
Case Report #1
A 23 year-old black man with sickle cell trait had a six-month history of right back pain associated with dyspnea and weight loss. An ultrasound revealed a six centimeters renal mass. One month later, he was referred to our service for investigation. Computed tomography (CT) scan showed a renal mass measuring eleven centimeters (cm) associated with pleural effusion and signs of lymphangitic carcinomatosis. He was empirically treated with sunitinib 50 mg per day for one week, until the result of the biopsy. The renal mass biopsy revealed renal medullary carcinoma. Owing to the worsening of the dyspnea and the biopsy results, sunitinib was discontinued and chemotherapy with cisplatin 35 mg per square meter plus gemcitabine 1000 mg per square meter both administered on D1 and D8 on a 21 day cycle was introduced. The patient died just one day after the beginning of the chemotherapy and two weeks after renal biopsy (a brief summary of patients epidemiological characteristics, therapies, response and survival rates are presented in Supplementary Table 1).
Case Report #2
A 24 year-old black man, medical student, with sickle cell trait, was submitted to an ultrasound due to abdominal pain, which revealed a 5 cm renal mass. Subsequently, a renal biopsy was performed and demonstrated a renal medullary carcinoma (Figure 1). Few weeks later, he was submitted to radical nephrectomy and regional lymphadenectomy. During the surgery, an extensive 13 cm tumor mass was removed with positive regional lymph nodes, with rapid disease progression compared to the sonographic findings. One month after surgery, the patient was hospitalized with dyspnea and pulmonary infection and thoracic CT scan revealed pulmonary metastasis and mediastinal lymphadenopathy. Chemotherapy was introduced with cisplatin 35 mg per square meter, paclitaxel 80 mg per square meter and gemcitabine 1000 mg per square meter on D1 and D8 every 21 days. The patient initially had clinical and radiological partial response (Figure 2), however had disease progression after six cycles of chemotherapy. This patient survived for eight months after renal biopsy and six months after diagnostic of metastatic disease.
Figure 1.
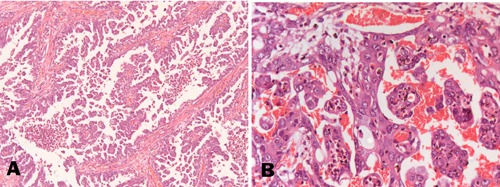
A) Sheets of cells with reticular growth pattern and a more compact adenoid cystic morphology (Hematoxylin & Eosin stain, Zeiss Axioshop 40, magnification×100). B) Sickled erythrocytes (Hematoxylin & Eosin stain, Zeiss Axioshop 40, magnification×400).
Figure 2.
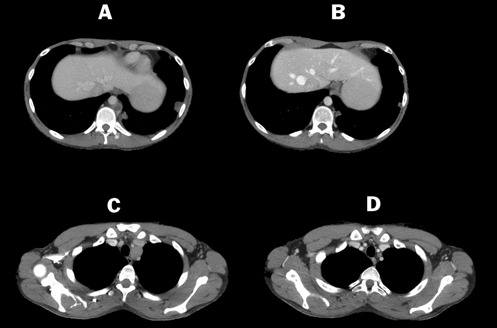
A) Paraaortic lymphadenopathy, patient case #2. B) Response after platin-based chemotherapy. C) Mediastinal lymphadenopathy, patient case #2. D) Response after platin-based chemotherapy.
Case Report #3
A 24 year-old black woman with sickle cell trait with a history of abdominal pain associated with 30 kilos weight loss in 6 months. CT scan showed an 11 cm tumor mass in the kidney, interaortocaval lymphadenopathy and liver metastasis. One month later she underwent a radical nephrectomy, which revealed renal medullary carcinoma. A month after surgery, she progressed with pulmonary and pleural disease progression and chemotherapy with cisplatin 70 mg per square meter on D1 and gemcitabine 1000 mg per square meter on D1 and D8 on a 21 day-cycle was initiated. Initial clinical and radiological response was observed (Figure 3), however she experienced disease progression after the fifth cycle and died five months after beginning chemotherapy.
Figure 3.
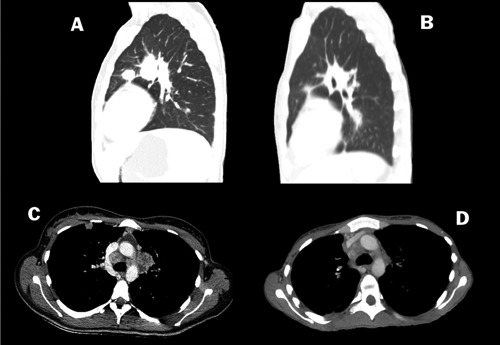
A) Lung metastasis, patient case #3. B) Response after platin-based chemotherapy. C) Mediastinal lymphadenopathy, patient case #3. D) Response after platin-based chemotherapy.
Case Report #4
A 30 year-old black man with sickle cell trait presented with a two month history of gross hematuria and abdominal pain. A CT scan showed a 6 cm tumor mass in the kidney and interaortocaval lymphadenopathy. Soon after diagnosis, he was submitted to a radical nephrectomy. He remained with small residual retroperitoneal lymph nodes and chemotherapy was introduced with cisplatin 70 mg per square meter on D1 and gemcitabine 1000 mg per square meter on D1 and D8 every 21 days for four cycles. During follow up, seven months after chemotherapy was completed, he presented with weight loss and interaortocaval lymphadenopathy on CT scan. Chemotherapy with doxorubicin 75 mg per square meter each 21 days was initiated. Nevertheless, the patient had disease progression after two cycles. Sunitinib 50 mg daily for 28 days each six weeks was performed for 2 cycles, but was fruitless. Cisplatin 25 mg per square meter and gemcitabine 700 mg per square meter both on D1 and D8 each 21 days was given for 3 cycles, but progression was observed and two months later the patient died, twenty six months after diagnosis.
Case Report #5
A 24 year-old white man with sickle cell trait had a 5 month history of abdominal pain and weight loss of 20 kilos. CT scan showed renal mass, retroperitoneal lymphadenopathy, bone and liver metastasis. Biopsy of the renal mass revealed renal medullary carcinoma. Chemotherapy with carboplatin AUC 2.5 D1 and D8 and gemcitabine 1000 mg per square meter D1 and D8 each 21 days was introduced, with initial clinical benefit and radiological stable disease, but disease progression occurred after 5 cycles. The patient died one month after the last cycle of chemotherapy, five months after the beginning of chemotherapy and six months after diagnosis.
Discussion
Owing to its rarity, there is little evidence in the literature about the best treatment for renal medullary carcinoma. It is well known for its poor prognosis, with an overall survival usually of less than 12 months.1,3 The main metastasis sites are lung, adrenal, liver and lymph nodes.
The treatment modalities are poorly studied and include surgery, chemotherapy, radiotherapy and biological agents. The most commonly used chemotherapy has low response rates and is based on urothelial carcinoma regimen.5 There are few reports of response with regimens based on platins,4,6 anthracyclines,7 and bortezomib.8
Three reports of successful treatment with platinum-based chemotherapeutic agents can be mentioned. Two patients aged 15 and 17 were treated with cisplatin or carboplatin, gemcitabine and paclitaxel. The first patient had disease progression after 7 cycles of chemo therapy and died 10 months after diagnosis. The second patient received 8 cycles of chemotherapy and had a 12-month overall survival.4 An eleven year-old patient had complete radiologic response after three cycles of carboplatin, gemcitabine and paclitaxel. He received a total of nine cycles of chemotherapy, remained disease-free for 11 months off therapy and had an overall survival of 24 months.6
In our report, overall survival varied between 2 weeks and 26 months, and median overall survival was 6 months. The patient who had the longest survival was submitted initially to nephrectomy following chemotherapy for low metastatic burden with cisplatin plus gemcitabine (case #4).
Time to progression after first line therapy in metastatic context varied between 1 week and 10 months, and median time to progression was 15 weeks. The longest time to progression was associated with the use of platin-based chemotherapy (case #4). Sunitinib was administered to two patients with no response.
Hematuria in patients with sickle cell trait or anemia should lead to the suspicion of renal medullary carcinoma. These cases should always be investigated. Early diagnosis is the key to achieving complete tumor resection, which is very important since renal medullary carcinoma is highly aggressive and presents low response rate to chemotherapy. The late diagnosis is the probably the reason why median overall survival in our service was worse than described in literature.
Conclusions
Renal medullary carcinoma has low response rates to conventional chemotherapy. However, in our case series, the best response was achieved using platin-based chemotherapy. Although molecular targeting agents may be promising, both patients treated with sunitinib in our case series had no response.
This small retrospective collection of patients from a high volume cancer institute also illustrates and reinforces two important points. The first is the implacable nature of this tumor, leading to death in virtually all patients, even when treated with platin-based chemotherapy. The second point is the limitations of cases reports regarding decision-making in oncology.
Reports of case series are the only piece of information available on this disease, considering the rarity of the disease and the difficulty to enroll a sufficient number of patients in a prospective randomized study, and are clearly insufficient to give us a better guideline as to how to approach those patients. In the modern era of targeted therapy and new technology in DNA analysis, probably the best strategy will be to embark in genetic analysis of individual cases, in order to better the pathologic pathways involved in the progression of this so lethal disease and come up with better drugs able to target those pathways in the future.
Acknowledgment
the authors would like to thank all the physicians and nurses involved in the treatment of each patient included in this article.
References
- 1.Hakimi AA, Koi PT, Milhoua PM, et al. Renal medullary carcinoma: the Bronx experience. Urology 2007;70:878-82 [DOI] [PubMed] [Google Scholar]
- 2.Davis CJ, Jr, Mostofi FK, Sesterhenn IA.Renal medullary carcinoma. The seventh sickle cell nephropathy. Am J Surg Pathol 1995;19:1-11 [DOI] [PubMed] [Google Scholar]
- 3.Swartz MA, Karth J, Schneider DT, et al. Renal medullary carcinoma: clinical, pathologic, immunohistochemical, and genetic analysis with pathogenetic implications. Urology 2002;60:1083-9 [DOI] [PubMed] [Google Scholar]
- 4.Strouse JJ, Spevak M, Mack AK, et al. Significant responses to platinum-based chemotherapy in renal medullary carcinoma. Pediatr Blood Cancer 2005;44:407-11 [DOI] [PubMed] [Google Scholar]
- 5.Baig MA, Lin YS, Rasheed J, Mittman N.Renal medullary carcinoma. J Natl Med Assoc 2006;98:1171-4 [PMC free article] [PubMed] [Google Scholar]
- 6.Walsh A, Kelly DR, Vaid YN, et al. Complete response to carboplatin, gemcitabine, and paclitaxel in a patient with advanced metastatic renal medullary carcinoma. Pediatr Blood Cancer 2010;55:1217-20 [DOI] [PubMed] [Google Scholar]
- 7.Schaeffer EM, Guzzo TJ, Furge KA, et al. Renal medullary carcinoma: molecular, pathological and clinical evidence for treatment with topoisomerase-inhibiting therapy. BJU Int 2010;106:62-5 [DOI] [PubMed] [Google Scholar]
- 8.Ronnen EA, Kondagunta GV, Motzer RJ.Medullary renal cell carcinoma and response to therapy with bortezomib. J Clin Oncol 2006;24:e14. [DOI] [PubMed] [Google Scholar]