

Abstract
[Purpose] In this study, combined training with breathing resistance and sustained physical exertion was carried out to evaluate its physiological effects and its effect on improve endurance capacity. [Subjects and Methods] The subjects were nine healthy adults (mean age 20.4, SD ± 1.7 years). The combined training group (n = 5) carried out 6 weeks of combined training using a cycle ergometer, with exercise load tests and respiratory function tests performed before and after the training. The results of the training were compared to a control group (n = 4) that only performed the cycling exercise without the combined training with breathing resistance. [Results] In the combined training group, ventilatory threshold, maximal load of the cycle ergometer in exercise load tests, and maximal voluntary ventilation increased after training. These increases after training were all significant, but none of these variables changed significantly in the control group. [Conclusion] The results imply that in comparison to conventional training methods, combined training with breathing resistance and sustained physical exertion is beneficial for increasing endurance capacity and respiratory muscle function. This result provides important information regarding the effects of the new training method for improving endurance capacity.
Key words: Respiratory muscle training, Exercise tolerance, Cardiorespiratory endurance
INTRODUCTION
Peak oxygen uptake (VO2peak) and ventilatory threshold (VT) reflect the capacity for endurance1,2,3), and improving them is beneficial for health4,5,6). To date, many different methods of training have been recommended for effectively improving endurance capacity, and the effectiveness of these methods has been examined. Rhythmic physical exercise such as running or cycling leads to improved VO2peak and VT3).
Endurance capacity depends on respiratory function in addition to circulatory and muscular function, and for this reason, there has recently been considerable interest in the relationship between respiratory muscle training, which aims to improve respiratory muscle function, and cardiorespiratory endurance. Some studies have reported that inspiratory muscle training during rest improves the cardiorespiratory endurance of patients with weakened respiratory muscles and that of healthy adults7,8,9,10,11), whereas other studies have reported no effect12,13,14,15). Thus, there is no consensus of opinion. In addition, with inspiratory muscle training during rest, it is difficult to combine an increased ventilation requirement brought about by an increase in required oxygen intake with respiratory load. Therefore it is difficult to continually carry out inspiratory muscle training during rest by applying resistance to deep breathing. Physical exercise under hypoxic conditions has been shown to be very effective at increasing endurance capacity16), but it is not possible to apply resistance to the respiratory muscles during this type of training. The subject needs to go to a location at a high altitude or use an apparatus to control the partial pressure of oxygen; thus, the training is difficult from the point of view of time and the financial costs involved. A training method that resolves these problems and effectively increases endurance capacity and respiratory muscle function would be beneficial not only for healthy adults, but also for elderly people and patients suffering from certain diseases. However, to date, there has been no examination of combined training with breathing resistance and sustained physical exertion in which rhythmic physical exercise is combined with the application of a respiratory load.
In this study, attempting to effectively improve endurance capacity and respiratory muscle function, we carried out combined training with breathing resistance and sustained physical exertion (CBS) and examined its effectiveness by comparing the results with those of a control group without breathing restrictions.
SUBJECTS AND METHODS
Subjects
The subjects were nine healthy adults (3 men, 6 women) who were randomly divided into two groups: the CBS group, which carried out CBS training on a cycle ergometer wearing a mask that provided resistance to breathing (2 men, 3 women); and the control group, which carried out training on a cycle ergometer with no mask (1 man, 3 women). The subjects performed the training over 6 weeks, and body measurements, respiratory function tests, and exercise load tests were carried out before and after the training period. The study was approved by the Ethics Committee of Saitama Prefectural University (no. 21042), and the subjects consented to participate after receiving a written explanation of the details of the study.
Methods
Both groups carried out three 2-week courses of training, for a total of 6 weeks. The training intensity was set using the heart rate reserve (HRR) method17). HRR value is calculated by subtracting heart rate at rest (HRrest) from maximum heart rate (HRmax). Target heart rate during exercise was calculated according to the formula:
| Target HR = [(HRmax − HRrest) × % intensity] + HRrest |
Target HR was 75% HRR during the first course, 80% HRR during the second course, and 85% HRR during the third course. HRmax was estimated by the formula HRmax = 220 − age3). Frequency of exercise was three times per week, and the control group performed cycle ergometer exercise for 30 min at a load that maintained the target heart rate. The pedaling cadence was 60 rpm. The CBS group wore a ReBNA (Patent Works Inc.; Fig. 1) and exercised at the same target heart rate as the control group. The ReBNA is a mask-type device with valves arranged such that inhalation is only through the nose and exhalation only through the mouth, and ventilation through two inspiratory valves and two expiratory valves produces respiratory load18). Cycle ergometer load and rating of perceived exertion (RPE) were recorded immediately before the end of training. An amended Borg scale19) was used for RPE. On completion of the third course of training, difficulty in breathing and fatigue in the legs were investigated using a questionnaire.
Fig. 1.
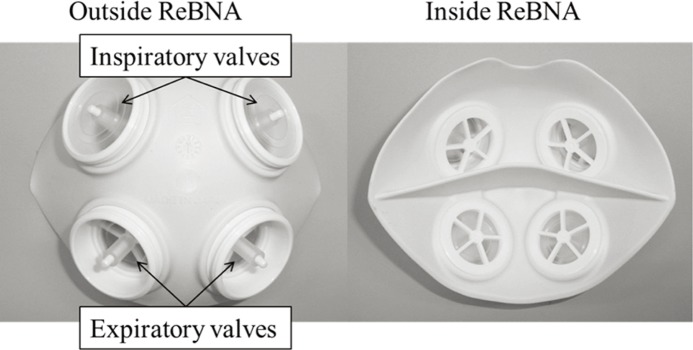
Appearance of the ReBNA. There are separate spaces inside the mask for the nose and mouth.
Height, weight, body fat percentage, muscle mass, and abdominal circumference were measured. Weight, body fat percentage, and muscle mass were measured using an InnerScan 50V (Tanita Co.).
Ramp load maximal exercise tests were carried out using a 232C xL cycle ergometer (Combi Co.). Measurements were taken using a Vmax respiratory metabolism measuring device (Nihon Kohden Co.). For exercise load measurement, subjects rested for 3 min and then warmed up for 3 min (men, 25 W; women, 15 W); this was followed by ramp load exercise (men, 25 W/min; women, 15 W/min) until either no further increase in oxygen extraction fraction was seen or the subject reached total exhaustion and was unable to continue. The criteria for discontinuing exercise tests were in line with the “General Indications for Stopping an Exercise Test in Low-Risk Adults,” according to the guidelines of the American College of Sports Medicine. After the exercise test, subjects cooled down for 3 min (men, 25 W; women, 15 W). The pedaling cadence was 60 rpm. VT was determined using the V-slope method20).
Vital capacity of the lungs (VC), forced vital capacity (FVC), and maximal voluntary ventilation (MVV12) were measured using a FUDAC-70 spirometer (Fukuda Denshi Co., Ltd). VC and FVC were measured twice each, the values were checked to ensure less than 10% measurement error between the two, and the larger value was adopted. If the measurement error exceeded 10%, measurements were repeated until the error came within 10%. MVV12 was measured three times, and the largest value was adopted. Maximum inspiratory mouth pressure (PImax) and maximum expiratory mouth pressure (PEmax) were measured using a HI-801 spirometer (Chest M.I., Inc). Each measurement was taken three times, and the largest value was adopted.
All statistical analyses were performed using SPSS software (SPSS Statistics version 19). Data were tested for normality using the Shapiro-Wilk test. The paired t-test, or Wilcoxon’s signed-rank test in cases of non-normality, was used to compare baseline (BL) values of all measures before training with their values after 6 weeks (6W) within each group. The unpaired t-test, or Wilcoxon’s test in cases of non-normality, was used to compare the results of the CBS and control groups.
RESULTS
All subjects completed the study (Table 1), and the exercise performance rate was 100%. Mean load during training for the three courses was 120.9 ± 3.1 W in the control group and 117.7 ± 3.6 W in the CBS group. Mean RPE was 7.0 ± 0.2 W in the control group and 8.4 ± 0.1 W in the CBS group (Table 2). The measured items at baseline (BL) and after training (6W) are shown in Table 3.
Table 1. Characteristics of all subjects at baseline.
| Control Group (n = 4) | CBS Group (n = 5) | |
| Age (y) | 21±2.1 | 20±1.1 |
| Male/Female | 1/3 | 2/3 |
| Body height (cm) | 161.8±7.7 | 163.3±10.8 |
| Body weight (kg) | 56.4±5.9 | 56.7±9.3 |
| BMI (kg/m2) | 21.5±0.6 | 21.2±1.7 |
| Body fat percentage (%) | 20.8±5.3 | 21.5±9.4 |
| Muscle mass (kg) | 42.4±6.9 | 42.6±10.7 |
| Abdominal circumference (cm) | 70.5±3.3 | 70.8±4.7 |
| Number of exercises per week (times) | 2.5±2.6 | 1.2±1.9 |
| Initial VO2peak (ml/kg/min) | 33.4±4.1 | 35.6±6.7 |
| Initial ventilatory threshold (ml/kg/min) | 20.2±4.6 | 20.1±3.4 |
mean ± SD
Table 2. Load of bicycle ergometer and RPE for the training.
| Control Group (n = 4) | CBS Group (n = 5) | |||
| Load (watts) | RPE | Load (watts) | RPE | |
| 1st course | 119.0±6.3 | 6.2±0.2 | 106.5±6.8 | 7.2±0.2 |
| 2nd course | 120.3±5.4 | 6.9±0.3 | 114.3±4.8 | 8.3±0.2 |
| 3rd course | 123.4±4.2 | 7.9±0.2 | 132.5±7.0 | 8.9±0.2 |
| Mean of 1st–3rd courses | 120.9±3.1 | 7.0±0.2 | 117.7±3.6 | 8.4±0.1 |
mean ± SE
RPE: rating of perceived exertion. Load for each training course is the value immediately before the end of training. RPE: perceived exertion was rated using a modified Borg scale (0–10).
Table 3. Body composition and cardiorespiratory variables at baseline (BL) and 6 weeks (6W).
| Control Group (n = 4) | CBS Group (n = 5) | |||
| BL | 6W | BL | 6W | |
| BMI (kg/m2) | 21.5±0.3 | 21.2±0.2 | 21.2±0.8 | 21.1±0.7 |
| Body weight (kg) | 56.4±2.9 | 55.8±2.8 | 56.7±4.2 | 56.3±3.6 |
| Body fat percentage (%) | 20.8±2.6 | 20.2±4.1 | 21.5±4.2 | 18.4±4.0 |
| Muscle mass (kg) | 42.4±3.5 | 42.3±4.4 | 42.6±4.8 | 43.7±4.3 |
| Waist circumference (cm) | 70.5±1.6 | 70.4±2.9 | 70.8±2.1 | 69.7±2.2b |
| VC (l) | 4.0±0.5 | 4.1±0.5 | 4.2±0.5 | 4.3±0.5 |
| %VC (%) | 109.3±8.2 | 117.9±5.0 | 114.0±4.9 | 116.7±4.5 |
| FVC (l) | 4.0±0.5 | 4.1±0.5 | 4.2±0.5 | 4.1±0.4 |
| %FVC (%) | 109.7±8.6 | 117.2±5.1 | 113.9±4.3 | 113.9±3.9 |
| FEV1(l) | 3.5±0.5 | 3.6±0.5 | 3.7±0.4 | 3.7±0.4 |
| FEV1% (%) | 86.5±1.5 | 87.3±0.5 | 88.5±2.2 | 89.3±2.0 |
| MVV12 (l/min) | 142.6±25.1 | 131.5±20.2 | 113.8±17.1 | 133.2±15.2a |
| PImax (cmH2O) | 92.0±11.7 | 94.7±12.6 | 86.8±5.3 | 96.0±5.2 |
| PEmax (cmH2O) | 110.7±13.4 | 110.2±8.8 | 109.8±15.1 | 114.3±12.0 |
| Maximal load (W) | 183.0±27.1 | 203.3±23.3 | 199.0±31.7 | 221.8±30.8d |
| VO2peak (ml/min/kg) | 33.4±2.0 | 37.3±2.6a | 35.6±3.0 | 42.2±3.1a |
| VCO2peak (ml/min/kg) | 43.9±4.2 | 50.3±5.2a | 47.3±5.4 | 56.0±5.3a |
| VEpeak (l/min) | 90.2±14.2 | 104.2±19.2 | 104.8±22.6 | 116.0±20.7 |
| HRpeak (bpm) | 182.0±7.5 | 186.3±4.5 | 186.6±2.2 | 188.6±2.8 |
| RRpeak (breaths/min) | 43.0±2.6 | 46.5±3.0 | 41.4±4.1 | 42.8±4.8 |
| Tvpeak (l) | 1.93±0.31 | 2.04±0.31 | 2.12±0.27 | 2.36±0.26 |
| VE/VO2peak | 46.6±1.9 | 48.3±2.5 | 49.1±5.3 | 47.1±3.6 |
| VE/VCO2peak | 35.7±1.5 | 35.9±1.3 | 36.8±3.0 | 35.4±2.1 |
| VT (ml/min/kg) | 20.2±2.3 | 20.6±1.6 | 20.1±1.5 | 27.3±1.2b,c |
| RRVT (breaths/min) | 30.0±1.5 | 32.0±3.0 | 24.4±2.5 | 27.2±1.7 |
| TvVT (l) | 1.17±0.20 | 1.20±0.22 | 1.33±0.16 | 1.59±0.14 |
| VE/VO2VT | 31.3±0.8 | 32.0±1.5 | 28.0±1.6 | 28.4±2.2 |
| VE/VCO2VT | 31.8±1.1 | 31.5±1.4 | 29.6±2.1 | 27.8±1.6 |
mean ± SE
a Comparison of BL and 6W within groups (Paired t test p < 0.05), b Comparison of BL and 6W within groups (Paired t test p < 0.01), c Comparison between groups at 6W (Student’s t-test p < 0.05), d Comparison of BL and 6W within groups (Wilcoxon’s Signed-Rank test p < 0.05). Italic variables were tested non-parametrically.
VC: vital capacity; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 second; MVV12: maximal voluntary ventilation; PImax: maximum inspiratory mouth pressure; PEmax: maximum expiratory mouth pressure; Maximal load: load at the end of exercise load experiment; HR: heart rate; RR: respiratory rate; Tv: tidal volume; VT: ventilatory threshold
Abdominal circumference in the CBS group was 70.8 ± 2.1 cm at BL and 69.7 ± 2.2 cm at 6W, showing a significant reduction at 6W (p < 0.01).
VO2peak in the control group was 33.4 ± 2.0 mL/min/kg at BL and increased significantly (p < 0.05) to 37.3 ± 2.6 mL/min/kg at 6W. VO2peak in the CBS group was 35.6 ± 3.0 mL/min/kg at BL and increased significantly (p < 0.05) to 42.2 ± 3.1 mL/min/kg at 6W. VCO2peak in the control group was 43.9 ± 4.2 mL/min/kg at BL and increased significantly (p < 0.05) to 50.3 ± 5.2 mL/min/kg at 6W. VCO2peak in the CBS group was 47.3 ± 5.4 mL/min/kg at BL and increased significantly (p < 0.05) to 56.0 ± 5.3 mL/min/kg at 6W. VT in the CBS group was 20.1 ± 1.5 mL/min/kg at BL and increased significantly (p < 0.01) to 27.3 ± 1.2 mL/min/kg at 6W. VT at 6W was 20.6 ± 1.6 mL/min/kg in the control group and 27.3 ± 1.2 mL/min/kg in the CBS group, a significantly higher value in the CBS group (p < 0.05). Ergometer maximal load at VO2peak in the CBS group was 199.0 ± 31.7W at BL and increased significantly (p < 0.05) to 221.8 ± 30.8 at 6W. Tidal volume at the ventilatory threshold (TVVT) in the control group was 1.17 ± 0.20 l at BL and 1.20 ± 0.22 l at 6W, an increase of 3%. TVVT in the CBS group was 1.33 ± 0.16 l at BL and 1.59 ± 0.14 l at 6W, an increase of 20% (p = 0.06).
In the questionnaire about fatigue after the third training course (Table 4), in the control group, three subjects reported greater fatigue in their legs than in their breathing, and one subject reported the same level of fatigue in their breathing and legs. In the CBS group, three subjects reported greater fatigue in their legs than in their breathing, and two subjects reported greater fatigue in their breathing than in their legs (Table 5).
Table 4. Questionnaire about fatigue.
| Please select the statement from 1 to 6 that best describes your fatigue during the three training courses |
| 1. My breathing feels more fatigued than my legs. |
| 2. My breathing feels much more fatigued than my legs. |
| 3. My breathing and my legs feel the same level of fatigue. |
| 4. My legs feel more fatigued than my breathing. |
| 5. My legs feel much more fatigued than my breathing. |
| 6. I don’t know. |
Table 5. Responses to questionnaire about fatigue.
| Control Group | Subject A | 3 |
| Subject B | 4 | |
| Subject C | 4 | |
| Subject D | 4 | |
| CBS Group | Subject E | 2 |
| Subject F | 4 | |
| Subject G | 1 | |
| Subject H | 5 | |
| Subject I | 4 |
MVV12 in the CBS group was 113.8 ± 17.1 l/min at BL and increased significantly (p < 0.05) to 133.2 ± 15.2 l/min at 6W.
DISCUSSION
The present study aimed to achieve an effective increase in endurance capacity and respiratory muscle function through CBS, in which rhythmic physical exercise was combined with respiratory load. To clarify the effectiveness of this training, a comparison was made with a control group that exercised with no respiratory load. The results yielded two major findings.
First, the results imply that CBS is more beneficial at improving endurance capacity than conventional training. VO2peak in both groups was significantly greater after the training, indicating that the amount of training performed in the present study was sufficient to increase endurance capacity. Maximal load and VT did not show any significant changes after the training in the control group, but these variables were both significantly greater after training in the CBS group. In the CBS group, valves provided resistance to inhalation and exhalation, thus exerting a load on the respiratory muscles during exercise. It is likely that the combined training involves physiological mechanisms different from those involved in exercise with no breathing resistance, and that this different mechanism influences the increase in maximal load and VT. Also, when the tidal volume increases, there is a decrease in the dead space ventilation, and ventilation efficiency increases, so that this breathing pattern reduces the oxygen consumption required for breathing movement. In the present study, although TVVT in the control group was almost unchanged after training, it increased by 20% in the CBS group (p = 0.06). CBS therefore tended to aid deep breathing. In studies to date of healthy adults, one report indicated that inspiratory training at rest increased endurance capacity7), and other studies reported that it did not produce an increase14, 15). Thus, there is no consensus of opinion. The CBS carried out in the present study differs from the respiratory training of previous studies in that a load was applied to both inhalation and exhalation. Furthermore, it was carried out under the increased ventilation requirement brought on by physical exercise, and there was no decline in the dust cleaning or humidifying effects on the air that accompanies inhalation through the nose. Thus, it appears that one of these training loads, or a combination of two or more factors, contributed to the improvement of maximal performance and cardiorespiratory endurance. The training effectiveness of CBS has not been reported in prior studies, and this new finding that a combination of respiratory load and physical exercise can contribute to an increase in endurance capacity is likely to be important when selecting training methods for sports or therapeutic exercise. However, the subject sample in the present study was small, which could possibly have influenced the result. Studies examining a greater number of subjects are needed to verify the effectiveness of CBS.
The second major finding of the present study is the implication that CBS improves respiratory muscle function. MVV did not change significantly after training in the control group, but in the CBS group, it showed a 17% increase (p < 0.05) after training. Increases in MVV of about 10% in healthy subjects as a result of respiratory training at rest have previously been reported7, 21), but no increases as a result of CBS have been reported. The present results show that CBS increased MVV, and to a greater degree than respiratory training at rest. Therefore this result suggest that CBS effectively increases MVV. Neither PImax nor PEmax changed significantly in the CBS group; thus, it is possible that factors other than maximum respiratory muscle strength are involved in the increase in MVV. Both MVV and endurance capacity improved in the present training, suggesting that respiratory muscle function and endurance capacity are related.
Although the results of the present study suggest that CBS yields superior improvements in endurance capacity and respiratory muscle function, there are many points regarding the mechanisms involved that are unclear. In the responses to the fatigue questionnaire, many subjects in the CBS group reported greater fatigue in breathing than in the legs, indicating the possibility that CBS brings about changes in load on the respiratory muscles and the leg muscles. It will be necessary to investigate muscle activity during training to test this possibility. In addition, there is also a need to measure the actual resistance to breathing experienced by subjects to clarify the exact load.
In conclusion, the present study yielded results suggesting that CBS achieves greater improvements in maximal performance, cardiorespiratory endurance, and maximal voluntary ventilation than conventional methods. These results provide important information regarding the effectiveness of the new training method aiming to improve endurance capacity. The degree to which these results can be generalized to training for subjects other than healthy young adults is unclear. Therefore, further studies are needed to clarify the rationale and mechanism through which the training improves endurance capacity and respiratory muscle function.
Acknowledgments
This study was partially subsidized by a Grant-in Aid for Product Development for Small and Medium Enterprises (Project to Support Testing, no. T211010006) and a subsidy by a Grant-in-Aid for Scientific Research (Grant-in-Aid for Young Scientists [B], no. 22700542). We thank Patent Works Inc. for supplying the mask-type device.
REFERENCES
- 1.Tanaka K, Matsuura Y, Kumagai S, et al. : Relationships of anaerobic threshold and onset of blood lactate accumulation with endurance performance. Eur J Appl Physiol Occup Physiol, 1983, 52: 51–56 [DOI] [PubMed] [Google Scholar]
- 2.Tanaka K, Watanabe H, Konishi Y, et al. : Longitudinal associations between anaerobic threshold and distance running performance. Eur J Appl Physiol Occup Physiol, 1986, 55: 248–252 [DOI] [PubMed] [Google Scholar]
- 3.Medicine ACoS: ACSM’s Guidelines for Exercise Testing and Prescription. New York: Lippincott Williams and Wilkins, 2011 [Google Scholar]
- 4.Sesso HD, Paffenbarger RS, Jr, Lee IM: Physical activity and coronary heart disease in men: the Harvard Alumni Health Study. Circulation, 2000, 102: 975–980 [DOI] [PubMed] [Google Scholar]
- 5.Blair SN, Kohl HW, 3rd, Paffenbarger RS, Jr, et al. : Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA, 1989, 262: 2395–2401 [DOI] [PubMed] [Google Scholar]
- 6.Blair SN, Kohl HW, 3rd, Barlow CE, et al. : Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy men. JAMA, 1995, 273: 1093–1098 [PubMed] [Google Scholar]
- 7.McMahon ME, Boutellier U, Smith RM, et al. : Hyperpnea training attenuates peripheral chemosensitivity and improves cycling endurance. J Exp Biol, 2002, 205: 3937–3943 [DOI] [PubMed] [Google Scholar]
- 8.Enright SJ, Unnithan VB: Effect of inspiratory muscle training intensities on pulmonary function and work capacity in people who are healthy: a randomized controlled trial. Phys Ther, 2011, 91: 894–905 [DOI] [PubMed] [Google Scholar]
- 9.Sturdy G, Hillman D, Green D, et al. : Feasibility of high-intensity, interval-based respiratory muscle training in COPD. Chest, 2003, 123: 142–150 [DOI] [PubMed] [Google Scholar]
- 10.Shahin B, Germain M, Kazem A, et al. : Benefits of short inspiratory muscle training on exercise capacity, dyspnea, and inspiratory fraction in COPD patients. Int J Chron Obstruct Pulmon Dis, 2008, 3: 423–427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sutbeyaz ST, Koseoglu F, Inan L, et al. : Respiratory muscle training improves cardiopulmonary function and exercise tolerance in subjects with subacute stroke: a randomized controlled trial. Clin Rehabil, 2010, 24: 240–250 [DOI] [PubMed] [Google Scholar]
- 12.Britto RR, Rezende NR, Marinho KC, et al. : Inspiratory muscular training in chronic stroke survivors: a randomized controlled trial. Arch Phys Med Rehabil, 2011, 92: 184–190 [DOI] [PubMed] [Google Scholar]
- 13.Litchke LG, Russian CJ, Lloyd LK, et al. : Effects of respiratory resistance training with a concurrent flow device on wheelchair athletes. J Spinal Cord Med, 2008, 31: 65–71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Williams JS, Wongsathikun J, Boon SM, et al. : Inspiratory muscle training fails to improve endurance capacity in athletes. Med Sci Sports Exerc, 2002, 34: 1194–1198 [DOI] [PubMed] [Google Scholar]
- 15.Inbar O, Weiner P, Azgad Y, et al. : Specific inspiratory muscle training in well-trained endurance athletes. Med Sci Sports Exerc, 2000, 32: 1233–1237 [DOI] [PubMed] [Google Scholar]
- 16.Daniels J, Oldridge N: The effects of alternate exposure to altitude and sea level on world-class middle-distance runners. Med Sci Sports, 1970, 2: 107–112 [PubMed] [Google Scholar]
- 17.Karvonen MJ, Kentala E, Mustala O: The effects of training on heart rate; a longitudinal study. Ann Med Exp Biol Fenn, 1957, 35: 307–315 [PubMed] [Google Scholar]
- 18.Nakajima Y, Oikawa M, Kuwano K, et al. : Determination of respiratory metabolism with a mask enhancing aerobic benefit. Annual Conference of Hokkaido Industrial Research Institute, 2007: 54.
- 19.Borg GA: Psychophysical bases of perceived exertion. Med Sci Sports Exerc, 1982, 14: 377–381 [PubMed] [Google Scholar]
- 20.Beaver WL, Wasserman K, Whipp BJ: A new method for detecting anaerobic threshold by gas exchange. J Appl Physiol, 1986, 60: 2020–2027 [DOI] [PubMed] [Google Scholar]
- 21.Leddy JJ, Limprasertkul A, Patel S, et al. : Isocapnic hyperpnea training improves performance in competitive male runners. Eur J Appl Physiol, 2007, 99: 665–676 [DOI] [PubMed] [Google Scholar]