

Abstract
Heart failure (HF) has been singled out as an epidemic and is a staggering clinical and public health problem, associated with significant mortality, morbidity, and healthcare expenditures, particularly among those aged 65 and older. The case mix of HF is changing over time with a growing proportion of cases presenting with preserved ejection fraction for which there is no specific treatment. Despite progress in reducing HF-related mortality, hospitalizations for HF remain very frequent and rates of readmissions continuing to rise. To prevent hospitalizations, a comprehensive characterization of predictors of readmission in patients with HF is imperative and must integrate the impact of multimorbidity related to coexisting conditions. New models of patient-centered care that draw upon community-based resources to support HF patients with complex coexisting conditions are needed to decrease hospitalizations.
Keywords: epidemiology, heart failure, population studies
Heart Failure: Investigation of an Epidemic
Heart failure (HF) is a major public health problem, with a prevalence of over 5.8 million in the USA, and over 23 million worldwide. In 1997, HF was singled out as an emerging epidemic1. An epidemic can reflect increased incidence, increased survival leading to increased prevalence or both factors combined. Delineating the respective responsibility of each of these factors is essential to understand the determinants of the HF epidemic. The conceptual framework that guides the investigation is illustrated schematically in Figure 1. As shown, progress in the primary prevention of HF would lead to decreasing incidence of the disease while improvement in medical care would result in improved survival, in turn increasing the prevalence of HF. Both incidence and survival in turn play a major role in the genesis of the burden of hospitalization among patients living with HF. An in-depth understanding of the data relevant to this conceptual framework is required to understand the HF epidemic and to design policies and strategies to prevent and manage HF. This review uses this conceptual framework to discuss incidence, mortality and hospitalizations in HF. To identify relevant studies, the Medline database was searched for publications with the subject headings “heart failure, epidemiology prevalence, incidence, trends” between 2005 and present. This review focuses on publications relevant to epidemiology and population sciences after reviewing the abstracts for relevance to these topics.
Figure 1.
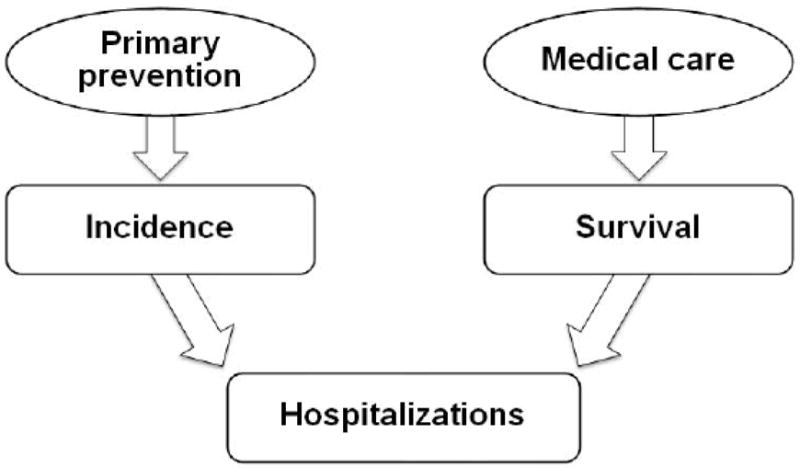
Investigating the HF Epidemic-Conceptual Framework
Definition and Classifications
Definition
In the American Heart Association/American College of Cardiology guidelines2, 3 HF is defined as “a complex clinical syndrome that can result from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill or eject blood”. The guidelines underscore that “it is largely a clinical diagnosis that is based on a careful history and physical examination”. As HF is a syndrome and not a disease, its diagnosis relies on a clinical examination and can be challenging. To assess the burden of HF in populations and study its epidemiology, standardized criteria that can be used on a large scale for ascertainment from medical records are needed.
Standardized criteria for HF diagnosis
Several criteria have been proposed to diagnose HF (Table 1). These include in particular the Framingham criteria,4 the Boston criteria,5 the Gothenburg criteria6 and the European Society of Cardiology criteria.7 All rely on similar indicators of symptoms and elevated filling pressures and combine data from the medical history, physical examination and chest X-ray.
Table 1.
Heart failure diagnostic criteria
| Framingham | Boston | European Society of Cardiology | Gothenburg Score Item and method of assessment | |
|---|---|---|---|---|
|
| ||||
|
|
|
CARDIAC SCORE
|
|
| History of heart disease (1-2pts) | Self-report | |||
|
| ||||
| Angina (1-2pts) | Self-report | |||
|
| ||||
| Edema (1pt) | Self-report | |||
|
| ||||
| Nocturnal Dyspnea (1pt) | Self-report | |||
|
| ||||
| Rales (1pt) | Physical exam | |||
|
| ||||
| Atrial fibrillation (1pt) | ECG | |||
|
| ||||
|
PULMONARY SCORE
| ||||
| History of Chronic bronchitis/asthma(1-2pts) | Self-report | |||
|
| ||||
| Cough, phlegm, or wheezing (1pt) | Self-report | |||
|
| ||||
| Rhonchi (2pts) | Physical exam | |||
|
| ||||
| Cardiac and pulmonary score are calculated and used to differentiate | ||||
| Cardiac form pulmonary dyspnea | ||||
The European Society of Cardiology criteria7 require objective evidence of cardiac dysfunction. For population sciences studies, this implies that, to apply these criteria, cardiac function must be uniformly evaluated by appropriate tests. This is not always the case in practice.8-12
When the Boston and Framingham criteria were compared against the masked assessment of a cardiologist,13 their sensitivity was excellent at 100%. The specificity of the Framingham criteria and their positive predictive value were lower than those of the Boston score for definite HF, but it provided greater sensitivity to diagnose possible HF. Altogether, five of the six scores studied by Mosterd et al.13 had a similar performance for the detection of HF but the sample size was small thereby limiting the ability to detect differences across criteria. The Boston criteria have been recommended over other diagnostic criteria in older adults due to their construct validity and improved prediction of adverse outcomes.14
The Cardiovascular Health Study criteria rely on a panel of physicians that assign a diagnosis of HF by reviewing data on history, physical examination, chest radiograms and medications. The comparison of the Framingham criteria to the Cardiovascular Health Study criteria yielded similar results.15 As the Framingham criteria offer good performance and are unaffected by time and use of diagnostic tests, they are well suited for studies of secular trends. Clinical cases of HF not meeting validation criteria are also important to capture in populations studies as they are captured in Vital Statistics and thus contribute to the epidemic and the use of health care resources.
Acute decompensated HF
HF is a chronic disease characterized by acute exacerbation. Acute decompensated HF has been defined as “gradual or rapid change in heart failure signs and symptoms resulting in a need for urgent therapy”.16 This definition comprises 3 clinical situations: worsening chronic HF, new onset HF and advanced HF. As acute decompensated HF is treated in the hospital, it constitutes one cause among several causes of hospitalization in patients living with HF. Identifying acute decompensated HF is crucial to accurately measure the burden of hospitalizations truly related to HF versus those related to comorbidity. Studies that rely on hospital dismissal codes may overestimate the true burden of acute decompensated HF by “counting” all cases ever diagnosed as HF.
In this context, one important question is whether existing criteria can accurately identify acute decompensated HF. The Atherosclerosis Risk in Communities (ARIC) study developed a classification, relying on manual adjudication to identify acute decompensated HF and compared it with other HF classifications including the Framingham criteria, the Boston criteria and the Gothenburg criteria (Table 1). The performance of these comparison criteria to the ARIC approach to identify acute decompensated HF was quite variable underscoring the importance of considering which set of criteria is applied to validate HF.17 Further work conducted in the ARIC study examined the accuracy of an automated algorithm for the classification of acute decompensated HF.18 Compared to a physician reviewer panel, the automated algorithm was more efficient and less costly but its accuracy was modest. These results delineate a domain where more work is urgently needed as the ability to accurately identify acute decompensated HF is critical to fully comprehend the burden of HF in populations.
Systolic and Diastolic Heart Failure
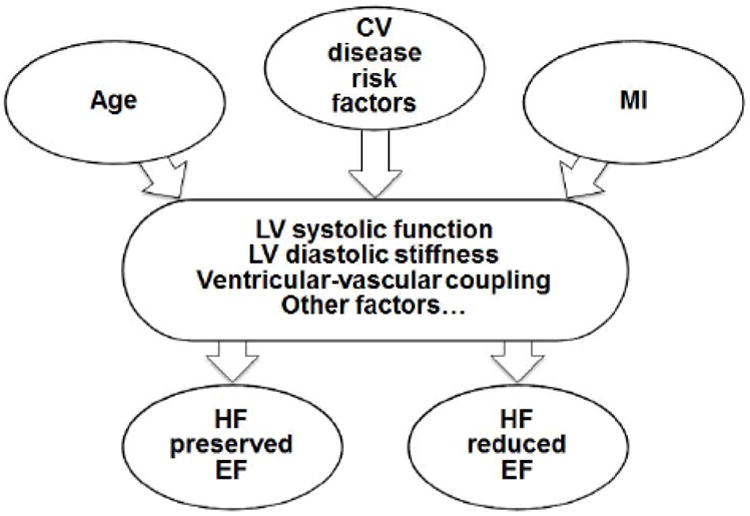
Further classification of HF requires knowledge of the parameters of left ventricular function. The left ventricular ejection fraction (EF) enables classifying HF as preserved or reduced EF (Figure 2).19 Different thresholds for EF have been recommended, all arbitrary in nature and derived from imaging studies with intrinsic variability.20 The threshold of 55% was recommended in the American Society of Echocardiography guidelines.21 The Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) registry used 40% as the cutpoint,12 as did the Acute Decompensated Heart Failure National Registry (ADHERE) Database.22 The American Heart Association and American College of Cardiology guidelines23 recommend 50% as a cut-off, which is used in the Framingham Heart Study19 and Olmsted County Study.24-28 The variations in threshold notwithstanding, EF is preserved approximately half of HF cases in the community.29, 30 To further classify subjects with HF and preserved EF, several criteria have been proposed,19, 31, 32 relying on the direct assessment of diastolic function which can be achieved with catheterization or echocardiography-Doppler.19, 32-36 Invasive measurements with conductance catheters have historically been considered the gold standard to measure filling pressures.37 However, it carries risks inherent to invasive studies, is seldom used in practice11 and is not feasible for population studies. While magnetic resonance imaging (MRI) is an excellent tool to assess cardiac volumes and mass38 and is gaining more ground in the evaluation of HF,39 its use to evaluate diastolic function is presently not established.40, 41 Echocardiography-Doppler is thus the approach of choice to assess diastolic function in routine practice. Echocardiography-Doppler examination is indicated for the evaluation of HF and categorized as a Class I indication (“conditions for which there is evidence and/or general agreement that a given procedure or treatment is beneficial…”) in the heart failure guidelines2, 3 Further, left ventricular function assessment is a core performance measure for heart failure under the Joint Commission on Accreditation of Health Care Organizations (JCAHO).42 Early Doppler indices for diastolic function have been criticized for their complexity, dependency on loading conditions and limited reproducibility.34, 43, 44 Tissue Doppler Imaging (TDI) combined with mitral inflow measurements, now provides a feasible approach to assess filling pressures.34, 45-51 Doppler measurements enable classifying diastolic function into mutually exclusive categories, indicative of progressive elevation of filling pressures.30 Several algorithms have been proposed including by the American Society of Echocardiography.52 The distinction between the existing sets of criteria should not obscure the fact that the basic measurements are similar such that it is important for the user to select the algorithm that he/she is most comfortable with based on the performance of the laboratory where the measurements are to be performed. Finally, as the field is rapidly evolving, it is likely that new measurements will enable characterizing left ventricular relaxation and be suitable for routine clinical use in the near future.39
Figure 2.
Heart Failure Risk Factors and Putative Mechanisms
Regardless of measurements issues, the mechanistic link between the elevation of filling pressures and the disease process is complex (Figure 2) and remains the subject of debate. Indeed, the causal role of intrinsic diastolic dysfunction (impaired relaxation and increased diastolic stiffness)33 was challenged against that of altered ventricular-vascular coupling.53-55 The altered ventricular-vascular coupling hypothesis needs to be considered cautiously as HF with normal EF is likely itself a heterogeneous entity within the HF syndrome.54, 56 Further, evaluating the putative role of other mechanisms requires complex measures that cannot be easily implemented in large scale epidemiology studies. One additional matter that must be discussed is pulmonary hypertension, which is frequent and often severe in HF with preserved EF. Although pulmonary venous hypertension contributes to pulmonary arterial hypertension, it does not always fully account for its severity, suggesting that a superimposed component of pulmonary arterial hypertension also plays a role.57 Finally, these mechanisms are not exclusive of one another and measuring diastolic function as can be done by echocardiography-Doppler is an important step towards a better understanding of the HF syndrome.58
Incidence and Prevalence of Heart Failure
In the U.S., prevalent cases of HF now exceed 5.8 million and each year more than 550,000 new cases are diagnosed.59, 60 Selected data on the incidence of HF are tabulated (Table 2) organized according to the criteria used to ascertain HF. Several estimates are derived from hospital discharges, which are not always validated by standardized criteria, and shifts in hospital discharge diagnoses preferences after the introduction of the Diagnosis-Related Groups payment systems have been documented.61, 62 For HF in particular, the potential for “upcoding” of discharge diagnoses due to reimbursement incentives is wellknown. Hospitalization statistics are event-based, not person-based and allow multiple hospitalizations for the same individual to be counted without distinguishing between first and subsequent admission such that incidence cannot be derived from such data. Thus, national statistics and claims data are not well suited to inform on the incidence of HF. Inpatient data may not capture all cases of HF as care is increasingly delivered in the outpatient setting.63 Studies using surveys of physicians or self-report are by design more inclusive in their ascertainment. They reported relatively broad ranges of prevalence without validation. When validation was carried out, approaches have ranged from medical record review and adjudication as in the Cardiovascular Health Study64 to the use of criteria such as the Framingham, Boston, or European Society of Cardiology criteria.4, 5, 65 Using standardized criteria, the incidence of HF in an earlier study from Framingham was between 1.4 and 2.3 per 1000/year among persons 29 to 79 years old.4 However, the size of the cohort inherently limits power to analyze secular trends in this report. Among the studies of secular trends,66-73 few included outpatient data. Others used hospitalized cases without validation, and are thus subject to secular changes in hospitalization practices and coding patterns, which likely confound time trends in incidence. It should not be surprising therefore that their results differ. Croft,67 comparing the rates of initial hospitalization for HF using Medicare hospital claims in 1986 and 1993, reported an increase in the initial hospitalization for HF, while acknowledging limitations related to the lack of validation and possible incomplete ascertainment of incidence. Data from the Henry Ford Health system, a managed care organization,71 indicated that the prevalence of HF was increasing over time but did not detect any secular change in incidence or mortality. In the Framingham Heart Study73 and the Olmsted County Study72 which include outpatient HF, the incidence of HF failure remained stable over time72 or even declined in women.73 It should be noted that, while the interpretation and informal comparison of trends across studies is appropriate, as adjustment approaches differ, the absolute numbers cannot be compared. Importantly, the trends noted among the elderly are different and data from the Kaiser Permanente system comparing the incidence of HF in 1970 to 1974 and 1990 to 1994 among persons 65 years old or greater indicated that the age-adjusted incidence increased by 14% over time and was greater for older persons and for men.74 The Framingham and Olmsted County studies also reported trends toward increasing HF incidence among older persons, which are concerning given the aging of the population.
Table 2.
Selected studies reporting on the incidence and prevalence of heart failure
| Diagnostic criteria | Author | Years | Incidence | Prevalence | Population source | Mortality |
|---|---|---|---|---|---|---|
|
| ||||||
|
NON VALIDATED CRITERIA
| ||||||
| Self-report | Schocken145 | 1971-75 | --- | 1-2% | NHANES I – Survey | At 10 years 43% |
| Ages 1-74 years, not adjusted | ||||||
|
| ||||||
| Self-report | Go146 | 2007- 2010 | --- | 2% | NHANES 2007-2010 | --- |
| Age ≥20 | ||||||
|
| ||||||
| First hospitalization for heart failure | Croft*67 | 1986 | White: 22.4/1000 person-yr | --- | Medicare beneficiaries (age ≥65) | In-hospital |
| Black: 22.4/1000 person-yr | Age adjusted | 1986: | ||||
| White: 13% | ||||||
| -------- | Black: 11% | |||||
| 1993 | --------- | |||||
| White: 24.6/1000 person-yr | 1993: | |||||
| White: 10% | ||||||
| Black: 26.1/1000 person-yr | Black: 9% | |||||
|
| ||||||
| First hospitalization for heart failure | Jhund76 | 1986 | Men: 1.2/1000 persons | --- | Scotland | 1-year age-adjusted |
| Women: 1.3/1000 persons | Age-adjusted | 1986 | ||||
| Men: 33% | ||||||
| ---------- | --------------- | Women: 31% | ||||
| 2003 | Men: 1.1/1000 persons | --------------------- | ||||
| 2003 | ||||||
| Women: 1.0/1000 persons | Men: 28% | |||||
| Women: 27% | ||||||
|
| ||||||
| Hospital discharge or death certificate with ICD code for HF | Loehr77 | 1987-2002 | White Women: 3.4/1000 person-yr | --- | Atherosclerosis Risk in Communities Study | Overall 1-year mortality: 22% (Similar for Blacks and Whites) |
| White Men: 6.0/1000 person-yr | Age-adjusted | |||||
| Black Women: 8.1/1000 person-yr | ||||||
| Black Men: 9.1/1000 person-yr | ||||||
|
| ||||||
| Hospital discharge diagnosis | Stewart*68, 69 | 1990-96 | Women: 1.3-1.9 /1000 persons | --- | Scotland | At 1 year |
| 1990: ~40% | ||||||
| Men: 1.3-2.2/1000 persons | All ages, not adjusted | 1996: ~36% | ||||
|
| ||||||
| Administrative database: CMS | Curtis90 | 1994 | 32/1000/person-yr | 9% | Medicare beneficiaries (age ≥65) | 1-year risk-adjusted |
| --------- | ------------- | ------------- | ||||
| 2003 | 29/1000/person-yr | 12% | Age-adjusted | 1994: 29% | ||
| 2002: 28% | ||||||
|
| ||||||
| Administrative database | Yeung75 | 1997 | 4.5/1000 persons | --- | Ontario, Canada | 1-year risk-adjusted |
| ---------- | ---------------------- | |||||
| 2007 | 3.1/1000 persons | Age and sex standardized | 1997 | |||
| Outpatients: 18% | ||||||
| Inpatients: 36% | ||||||
| 2007 | ||||||
| Outpatients: 16% | ||||||
| Inpatients: 34% | ||||||
|
| ||||||
|
STANDARDIZED CRITERIA
| ||||||
| Framingham criteria | Levy* 73 | 1950-99 | ~5/1000 person-yr | --- | Framingham Heart Study | At 1 year age- adjusted |
| All ages, age adjusted, mostly whites | ||||||
| 1950-1969 | ||||||
| Men: 30% | ||||||
| Women: 28% | ||||||
| 1990-1999 | ||||||
| Men: 28% | ||||||
| Women: 24% | ||||||
|
| ||||||
| Framingham criteria | Barker74 | 1970-1974 | Women: 8.6 /1000 person-yr | --- | Kaiser Permanente | 1-year age-adjusted mortality |
| Men: 11.7/1000 person-yr | Age adjusted, mostly whites | |||||
| ---------- | ------------------------- | 1970-1974: | ||||
| 1990-1994 | Women: 11.8 /1000 person-yr | Men: 47% | ||||
| Women: 27% | ||||||
| Men: 12.7/1000 person-yr | ||||||
| 1990-1994: | ||||||
| Men: 33% | ||||||
| Women: 28% | ||||||
|
| ||||||
| Framingham criteria | Roger* 72 | 1979-2000 | ~3/1000 persons | --- | Olmsted County | At 1-year (75-year- olds) |
| Age adjusted, mostly whites | ||||||
| 1979-1984: | ||||||
| Men: 30% | ||||||
| Women: 20% | ||||||
| 1996-2000: | ||||||
| Men: 21% | ||||||
| Women: 17% | ||||||
|
| ||||||
| Framingham criteria | McCullough*71 | 1989-99 | Women: 3.7-4.2 /1000 persons | Women 0.4%-1.4% | REACH Study | Per year: 17% |
| Men: 4.0-3.7/1000 persons | Henry Ford Health System | |||||
| Men 0.4-1.5% | 50% Whites; Age adjusted | |||||
|
| ||||||
| Framingham criteria | Goldberg147 | 2000 | ~2/1000 persons | --- | Worcester, MA hospitals | Hospital case fatality rate: 5% |
| Not age-adjusted | ||||||
|
| ||||||
| Boston criteria | Remes148 | 1986-88 | Women: 1.0/1000 persons | --- | Eastern Finland | --- |
| Men: 4.0/1000 persons | In and out patient national registries | |||||
| Age adjusted | ||||||
|
| ||||||
| Boston criteria | Nielsen 149 | 1993-95 | --- | 0.5-12% | Denmark | --- |
| General practice population | ||||||
| Ages ≥ 50, not adjusted | ||||||
|
| ||||||
| European Society of Cardiology criteria | Bleumink84 | 1989-2000 | Women: 12.5/1000 person-yr | 1998: 7% | The Rotterdam Study | At 1 year: 37% |
| Men: 17.6/1000 person-yr | Not age adjusted | |||||
|
| ||||||
| European Society of Cardiology criteria | Cowie121 | 1995-96 | Women: 1.2/1000 persons/yr | --- | Geographically defined in UK | --- |
| Men: 1.4/1000 persons/yr | In-and out-patient | |||||
| All ages, not adjusted | ||||||
|
| ||||||
| European Society of Cardiology criteria | Davies 150 | 1995-99 | --- | 2-3% | UK population | --- |
| Random sample | ||||||
| Ages ≥ 45, not adjusted | ||||||
|
| ||||||
| Cardiovascular Health Study criteria | Gottdiener123 | 1990-96 | Non-black: 19/1000 person-yr | Cardiovascular Health Study | --- | |
| Black: 19/1000 person-yr | Age 65-100, age adjusted | |||||
| Women: 15/1000 person-yr | ||||||
| Men: 26/1000 person-yr | ||||||
|
| ||||||
| Multi-Ethnic Study of Atherosclerosis criteria | Bahrami78 | Enrolled from 2000-2002; Median follow-up 4.0 yrs | African Americans: 4.6/1000 person- yr | --- | Multi-Ethnic Study of Atherosclerosis | --- |
| Hispanic: 3.5/1000 person-yr | Not age-adjusted | |||||
| White: 2.4/1000 person-yr | ||||||
| Chinese Americans: 1.0/1000 person- yr | ||||||
Denotes studies reporting on time trends
The data discussed up to this point reflect largely the USA experience. In Scotland, Stewart69 suggested that trends in HF hospitalization in the 1990s, had “leveled off”. These results are limited by the lack of validation and sole use of inpatient data but prompt the question of whether the stabilization of the HF hospitalization rates could be offset by increasing out-patient care practice. Data on temporal trends in incidence of HF from Ontario75 and Scotland76 are informative in this regard as they indicate that the incidence of HF started to decline since the late 1990’s. This finding is important, as it further highlights the fact that the continuing burden of HF hospitalizations reflects persisting difficulties in managing existing disease, rather than an increasing number of new cases developing HF.
Most of the aforementioned studies pertain to white subjects, and data on the burden of HF in diverse populations are scarce. In ARIC and in the Multi-Ethnic Study of Atherosclerosis (MESA), HF incidence was higher in African-Americans than in Caucasians. In both studies, the difference between African- Americans and Caucasians was attenuated after adjustment and overall the greater HF incidence in African-Americans was related to their greater burden of atherosclerotic risk factors as well as to socioeconomic status.77, 78 This underscores the imperative for continued community surveillance of cardiovascular disease in diverse populations.79, 80 Data on the incidence and prevalence of HF according to EF and how it may have changed over time are very limited. The available evidence suggests that the prevalence of HF with preserved EF increased over time.24
Measures of lifetime risk are anchored in a robust methodological framework, provide more complete information than shorter term risk and are useful to identify patients at risk and communicate with them for the purpose of risk modification.81
For HF, the reported lifetime risk of developing the disease ranged from 20% to 33% in predominantly white cohorts.82 Recently, lifetime risks for developing HF were reported among a diverse large group of 39,578 participants in several cohorts, including the Chicago Heart Association Detection Project in Industry, the ARIC study and the Cardiovascular Health Study.83 At age 45 years, lifetime risks for HF through age 75 or 95 years were 30% to 42% in white men, 20% to 29% in black men, 32% to 39% in white women, and 24% to 46% in black women. Higher blood pressure and body mass index at all ages in both blacks and whites, led to higher lifetime risks.
In the Rotterdam Heart Study, the lifetime risk of HF at the age of 55 was 33% for men and 29% for women.84 These numbers are commensurate with the data from the USA.
In summary, the overall prevalence of HF ranges from 1 to 12% based on available data from the USA and Europe. The incidence of HF varies across studies largely reflecting differences in ascertainment and adjustment approaches. These methodological differences however do not affect the interpretation of secular trends in incidence where the focus is on the evolution over time. Temporal trends are congruent across studies and quite informative for the investigation of the HF epidemic as they indicate that the incidence of HF is stable or perhaps even decreasing over time. Available data indicate that lifetime risks are very high regardless of gender, race, and geography underscoring the importance of population-wide efforts to contain the burden of HF.
Mortality of Heart Failure
After the diagnosis of HF, survival estimates are 50% and 10% at 5 and 10 years, respectively,85-87 and left ventricular dysfunction is associated with an increase in the risk of sudden death.88 Improvement in the survival of hospitalized HF among the Scottish population was reported85 with notable age and sex differences in the magnitude of the secular trends. These data may reflect in part the effectiveness of angiotensin converting enzyme inhibitors. However, the median survival improved relatively modestly from 1.2 to 1.6 years such that, while the large sample size (66,547 patients) results in high statistical significance, the clinical significance of this improvement in survival is more modest. Further, the analyses relied solely on hospitalized cases, not validated, such that the improvement in outcome may be confounded by trends in coding practice and shifting of hospitalization thresholds. Regardless, these data resonate with clinical trials that indicated that angiotensin converting enzyme inhibitors, while associated with large reductions in the relative risk of mortality, resulted in more modest absolute event-rate difference.89 Administrative data however convey somewhat of a different message. In the Henry Ford Health system, which include outpatient encounters, the median survival was 4.2 years without any discernible improvement over time.71 Similar, among more than 2 million elderly Medicare beneficiaries, early and long term mortality remained quite high (115 at 30 days and 37% at one year).90
These discrepancies in survival estimates underscore the challenges in investigating the HF epidemic and help delineate key requirements for such evaluation. This investigation should include all cases of HF in a geographically defined population and use standardized validation criteria in order to generate valid longitudinal trends. The analyses should examine trends in hospital admission as an additional outcome as high hospital admission rates after diagnosis provide insights into the outcome of HF, independently of disease severity,91-95 and are an important component of its public health burden. Data from Framingham73 and Olmsted County72 underscored the persistently high mortality of HF in these populations, despite improvements over time: indeed, after age adjustment, estimated 5-year mortality rates were 59% in men and 45% in women during the time period 1990–1999 in Framingham and 50% in men and 46% in women during the time period 1996–2000 in Olmsted County. Improvements in survival were noted more specifically within an elderly population as shown by data from the Kaiser Permanente system. Indeed, over the two decades between the mid 1970’s and mid 1990’s after adjustment for age and comorbidities, survival after the diagnosis of HF improved by 33% in men and 24% in women.74 Importantly, in the Kaiser Permanente study, improvement in survival was primarily associated with beta blocker treatment. Data from Ontario75 and Scotland76 also support the observation that while survival after HF diagnosis remains quite poor, improvements have been detected since the late 1990’s. Altogether, these trends in mortality coincide temporally with major changes in the treatment of HF and thus suggest that HF treatment is effective in the community but that much progress remains to be accomplished. As the proportion of HF with preserved EF for which there is no specific treatment is increasing over time its prevalence will likely increase, underscoring the urgent need for new therapeutic approaches of this entity.24
The causes of death in HF can be challenging to ascertain. In the community, cardiovascular deaths are less frequent among subjects with preserved EF. Indeed, in Olmsted County, Minnesota, among 1063 persons with HF, the leading cause of death in subjects with preserved EF was non-cardiovascular (49%) versus coronary disease (43%) for subjects with reduced EF. The proportion of cardiovascular deaths decreased from 69% in 1979-1984 to 40% in 1997–2002 (p = 0.007) among subjects with preserved EF contrasting with a modest change among those with reduced EF (77% to 64%, p = 0.08).96 The shift in the distribution of the causes of death towards less cardiovascular causes is congruent with the major burden of comorbid conditions in HF and is of crucial importance for the management of HF and the interpretation of its outcomes.
In summary, survival after the diagnosis of HF remains quite poor but has improved substantially over time. The results are consistent across studies and, combined with the aforementioned trends in incidence, indicated that the epidemic of HF is an epidemic of hospitalizations among survivors who now live longer with the disease.
Hospitalizations in Heart Failure
As the incidence of HF has remained stable over the past 2 decades while survival has improved,71-73 the HF epidemic is a large chronic disease epidemic reflecting an increase in the prevalence of HF in an aging population and the improved survival of patients with HF.71 HF is characterized by periodic exacerbations that require treatment intensification most often in the hospital and is the single most frequent cause of hospitalization in persons 65 years and above. Nearly 1 million hospitalizations for HF occur each year with rates of hospitalization continuing to rise. This trend, coupled with the forecasting of a major increase in the prevalence of HF by the American Heart Association,97 underscores the persisting severity of the burden that HF creates on health care systems and the need for continued surveillance of HF trends to delineate strategies for management. Importantly, such strategies can be expected to change over time as the case mix of the disease evolves. Examples of the importance of such population surveillance can be found in several recent publications. Using data from the Centers for Medicare and Medicaid services (CMS) data, Chen reported an encouraging decline in admission rates for HF between 1998 and 2007.98 This decline appeared largely related to a reduction in the number of unique individuals hospitalized for HF. Over the same time period, however CMS data indicate that readmission rates after an index admission for HF have remained unchanged or have even increased.99 A subsequent analysis of CMS data indicates that after an initial hospitalization, 25% of HF patients are readmitted within 30 days with 35% of readmissions also attributed to HF.100 Data from the Veteran’s Affairs Health Care System also support the note that as mortality was decreasing, readmission rates have in fact increased over time.101 Taken collectively, these important reports suggest that that threshold for admitting patients with HF to the hospital might be evolving. However, once patients have been hospitalized with HF, their risk of readmission is not decreasing over time but they will be readmitted rather infrequently because of HF. Hospital readmissions are now a quality indicator under the Hospital Readmissions Reduction Program of the Patient Protection and Affordable Care Act with downward adjustment of Medicare payment for hospitals with “excess” 30-day readmission rates.102 This program has been controversial specifically raising concerns for HF that the driver of readmission is not the disease per se but rather the associated comorbidity burden poorly addressed by disease-specific disease management programs. Hence, the need to inform policy by an understanding of the root causes of hospitalizations is urgent.103 Doing so effectively requires consideration of several methodological issues, particularly related to data sources.104 Administrative datasets provide extensive population coverage but hospital admission data are most often event-based, counting multiple hospitalizations for the same individual. Diagnoses are not validated and discharge diagnoses choices are sensitive to changes in payment systems.61, 62, 79 Clinical data are lacking, which limits case mix adjustment. Clinical registries provide rich clinical information on HF and are critical to gain insight into real life clinical practice. Several large scale registries are specifically dedicated to HF. The Organized Program to Initiate Life-Saving Treatment in Hospitalized patients with Heart Failure (OPTIMIZE-HF) registry includes 259 hospitals that have enrolled more than 50,000 hospitalized patients with HF.105 Initially supported by industry, OPTIMIZE-HF is now integrated to the American Heart Association (AHA) Get with the Guidelines (GTWG) program, which includes 558 hospitals and more than 530,000 hospitalized patients with HF.106 The Acute Decompensated Heart Failure National Registry (ADHERE), sponsored by industry (Scios Inc California), enrolled more than 150,000 patients from 300 community and academic centers to evaluate characteristics, management, and outcomes of patients hospitalized with acute decompensated HF107 Participation to registries is voluntary, creating an unavoidable selection bias and registries are seldom positioned to ascertain the incident status of HF such that the ensuing incidence prevalence bias also limits validity. Registries typically include only in-patient data on clinical presentation, care and outcomes. These limitations are important to consider while interpreting registry data.
Data on the cause of hospitalizations among HF patients suggest that HF-specific hospitalizations may be noticeably less frequent than all-cause hospitalizations. This observation is critically important as intense treatment efforts (medications, device and disease management-based) are intrinsically diseasecentric and directed at reducing HF exacerbation. Thus, HF-specific hospitalizations are a key indicator of the effectiveness of HF-specific treatments but disease-specific interventions cannot be expected to appreciably reduce all hospitalizations among persons living with HF, given the high prevalence of comorbidity in these patients. National Hospital Discharge Survey data from 1979 to 2004 indicate that whereas HF was the first-listed diagnosis for 30% to 35% of these hospitalizations, the proportion with respiratory diseases and noncardiovascular, nonrespiratory diseases as the first-listed diagnoses increased over time.108
In the community of Olmsted County, among incident HF cases diagnosed between1987 to 2006, hospitalizations were common after HF diagnosis, with 83% of the patients hospitalized at least once but the reason for hospitalization was HF in only 17% of hospitalizations whereas 62% were attributed to non-cardiovascular causes.109 Using the Nationwide Inpatient Sample, Blecker et al reported on trends in HF hospitalizations between 2001 and 2009. Primary HF hospitalizations declined but hospitalizations with a secondary diagnosis of HF remained stable.
In summary, these data underscore the major role of comorbidity in HF110, 111 and that, to reduce the burden of hospitalizations in HF, strategies must consider both cardiac disease and non-cardiac conditions. While initial hospitalizations are seemingly decreasing, readmissions after an initial hospitalization are not declining such that, with the increased survival of patients living with HF, the overall burden of hospitalizations in HF remains very large.
Etiology of Heart Failure—An Evolving Picture
Assigning a cause to HF should be envisioned while focusing on clinically ascertained risk factors and acknowledging that multiple causes for HF often co-exist and interact in a given patient. From a public health and prevention perspective, the determination of the prevalence of each respective cause as ascertained clinically is important because of the public health implications. To this end, the prevalence of a given risk factor combined to the risk of HF that it confers enables computing the attributable risk of a given factor for HF. This in turn provides an indication of what proportion of the cases of HF would be avoided if the risk factor in questions was eliminated.
Such analyses also have mechanistic implications. For example, demonstrating an increase in the attributable risk of diabetes mellitus independently of clinical coronary disease would then prompt investigations about the mechanisms whereby diabetes leads to HF in the absence of overt coronary disease. Such mechanisms may include occult coronary disease, but within the appropriate analytical framework, this would be distinct from clinically established coronary disease. The importance of defining the respective contribution of these two entities contrasts with the lack of knowledge in this regard. Moreover, the reported data are conflicting and secular trends have infrequently been examined. Yet, the population burden of putative risk factors for HF is changing in the population, such that the attributable risk of these factors for HF may be evolving as well. Examples of the prevalence and attributable risk of selected factors are presented in Figures 3 and 4 using data from the Framingham112 and Olmsted County113 studies, selected as the similarities of the presentation of the results enabled creating these plots (Figures 3 and 4). These illustrate that, for example, for hypertension, while the prevalence is very high exceeding 50% in all groups, the attributable risk is lower and varies across groups reflecting differences in the relative risk of HF associated with hypertension.
Figure 3.
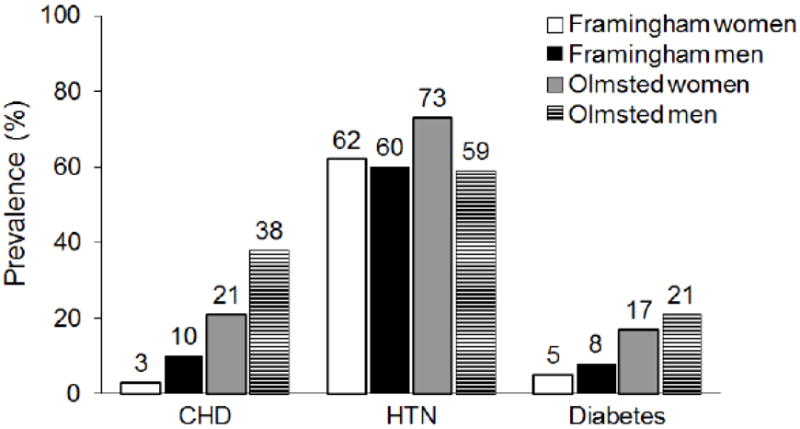
Prevalence of Risk Factors in Heart Failure
Figure 4.
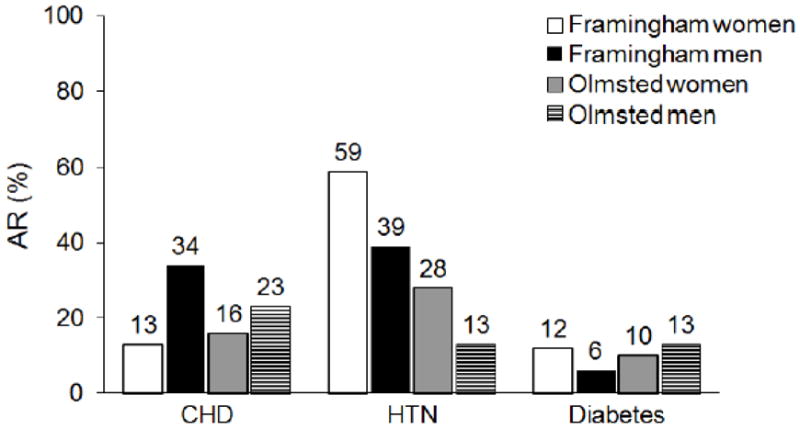
Attributable Risk of Select Risk Factors for Heart Failure
For coronary disease, estimates of the prevalence among patients with HF vary considerably across studies. Fox,114 using angiography, concluded that coronary disease was causal in 52% of new HF cases under age 75 in a geographically defined population and that clinical assessment without angiography under-estimates the contribution of coronary disease to HF. However, few patients were over 75 years of age and only 73% underwent angiography, reflecting substantial selection bias. Reviewing randomized trial data, Gheorgiade concluded the prevalence of coronary disease in HF was 68%.115 However, important methodological considerations limit the inference that can be drawn from these data. Indeed, the limitations in external validity inherent to clinical trials may be even more apparent in HF trials, which typically include younger patients and more men than the general population of HF.116, 117 Furthermore, entry criteria in HF trials are heterogeneous and seldom validated.118 Finally, HF trials often require systolic left ventricular dysfunction,116 thereby excluding a substantial proportion of HF cases.25, 119 An observational report of patients with HF suggest that the prevalence of coronary disease in HF is 50%,120 while a population-based study in England reported that coronary disease was the etiology of HF in 36% of the cases.121 This is commensurate with what was noted among men in the Olmsted County study113 but higher than that reported in the Framingham Heart Study112 (Figure 3). These large discrepancies likely reflect differences in populations, study design and ascertainment approaches. They also underscore our limited knowledge with regards to the etiology of HF, which hinders prevention. In the first National Health and Nutrition Examination Survey (NHANES I), coronary disease had the largest population attributable risk for HF at 62% compared to the other risk factors analyzed (hypertension, obesity, diabetes and smoking).122 The attributable risk of hypertension was 10% and that of diabetes was 3% due to its low prevalence. This likely underestimates, as acknowledged by the authors, the role of diabetes which was ascertained by self-report among patients enrolled more than 20 years ago with the incidence of diabetes increasing over time. In the Cardiovascular Health Study, the attributable risk of coronary disease for HF was similar to that of hypertension, around 12%, with a notable attributable risk of 8% for diabetes.123 The Framingham Heart Study historically underscored a large contribution of hypertension to HF.112, 124-126 (Figures 3 and 4) Over time, however, it suggested a 41% increase in the prevalence of coronary disease and a 10% decrease in that of hypertension in HF.127 Whether the results of Framingham are generalizable to larger populations, thereby suggesting that the etiology of HF shifted from hypertension to coronary disease remains to be determined, particularly given unfavorable hypertension trends in the US and in Olmsted County discussed below. To this end, when the contribution of coronary disease to HF and its hypothetical change over time is examined by analyzing population trends in coronary disease, the data are difficult to reconcile with the aforementioned hypothesis of an increasing contribution of coronary disease to HF. Secular trends in the incidence of myocardial infarction (MI) indicating that the epidemiology of MI is changing that, the burden of incident hospitalized MI, while displaced towards older age groups, is decreasing and that the severity of myocardial infarction is decreasing128-130 These findings indicate that the incidence of HF after MI can be expected to be declining over time. There have been few community-based or population investigations of the long-term trends in the incidence of HF after MI. Among residents of Olmsted County with an incident MI and no previous history of HF, a decline in the incidence of HF post MI was observed and the relative risk of HF post MI in 1994 versus 1979 was 0.72 (95% CI 0.55 to 0.93)27 However, data from the Framingham Heart Study pertaining to 676 participants who experienced a first MI between 1970 and 1999 indicate that the 30-day incidence of HF after MI rose from 10% in 1970 to 1979 to 23.1% in 1990 to 1999 as 30-day mortality after MI declined over the same period.131 More recent data from the national Swedish hospital discharge and death registries, among 175,216 patients with a first MI between 1993 and 2004, decreasing trends in the incidence of HF post MI were observed with a 4 percent/year decrease in the adjusted risk of HF.132 In the Worcester Heart Attack Study, the incidence of HF post MI decreased over time between 1986 and 2005.133 The discrepancies across studies likely reflect the different periods under observation during a time of profound changes in the epidemiology of MI. This in turn underscores the importance of continued surveillance of HF post MI and of the evolving causes of HF. Finally, while it is conceivable that more chronic forms of coronary disease could lead to HF without myocardial infarction, the role of chronic coronary disease in the genesis of HF is not defined.
With regards to hypertension, conversely, unfavorable trends in awareness, treatment and control of hypertension have been documented.134, 135 Thus, coronary disease and hypertension trends in population studies both suggest that the attributable risk of hypertension for HF should remain high. To this end, in Olmsted County, there was no evidence for a temporal change until 2002 in the population attributable risk for HF of coronary disease, diabetes, and smoking. By contrast, the population attributable risk of hypertension increased from 15% (1979–1984) to 29% (1979–2002), and that of obesity from 8% (1979–1984) to 17% (1997–2002).113
Finally, the rising tide of diabetes mellitus136 and obesity137 raise the concern of an increasing role of these two entities in the genesis of HF. Notwithstanding uncertainties with regards to the exact cellular and molecular mechanisms by which obesity and diabetes impact both systolic and diastolic left ventricular function, there is mounting evidence for their causal link to HF independently of clinical coronary disease and hypertension.138-142 To this end, the population burden of HF attributable to obesity and diabetes was recently examined in the ARIC study 143, 144 For obesity, while complete elimination of obesity/overweight could prevent almost one third (28%) of new HF cases, a more realistic 30% reduction in obesity/overweight could prevent 8.5% of incident HF cases.144 For diabetes, a relatively modest 5% reduction in its prevalence would lead to approximately 53 and 33 fewer incident HF hospitalizations per 100,000 person-years in African-American and Caucasian persons, respectively.143 These results indicate that even modest modification of these risk factors would favorably impact the burden of HF.
Conclusion
HF is a staggering clinical and public health problem. The study of the epidemiology of HF demonstrated that while HF is associated with significant mortality, morbidity, and healthcare expenditures, particularly among those aged 65 and older, this burden is not related to an increase in the incidence of the disease. Rather, it reflects the chronic clinical course of patients living with HF, whereby progress in reducing HF-related mortality translates to nearly 1 million hospitalizations for HF occurring each year with frequent readmissions. To improve outcomes for patients and prevent hospitalizations, an in-depth understanding of the causes of hospitalizations in patients living with HF is imperative.
Over time, the case mix of HF is changing with a growing proportion of cases presenting with preserved ejection fraction and the causes of HF are evolving. These secular trends underscore the importance of continued disease surveillance to plan prevention and care programs
Despite progress in reducing HF-related mortality, hospitalizations for HF remain very frequent and rates of readmissions continuing to rise. To prevent hospitalizations, a comprehensive characterization of predictors of readmission in patients with HF is imperative and must integrate the impact of multimorbidity related to coexisting conditions.
Acknowledgments
Sources of Funding
Supported in part by grants from the Public Health Service and the National Institutes of Health (RO1 HL 59205 and RO1 HL 72435).
Nonstandard Abbreviations and Acronyms
- ADHERE
Acute Decompensated Heart Failure National Registry
- AHA
American Heart Association
- ARIC
Atherosclerosis Risk in Communities
- CMS
Centers for Medicare and Medicaid Services
- EF
Ejection fraction
- GTWG
Get with the Guidelines
- HF
Heart Failure
- JCAHO
Joint Commission on Accreditation of Health Care Organizations
- MESA
Multi-Ethnic Study of Atherosclerosis
- MRI
Magnetic resonance imaging
- NHANES I
National Health and Nutrition Examination Survey
- OPTIMIZE-HF
Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure
- TDI
Tissue Doppler Imaging
Footnotes
Disclosures
None
References
- 1.Braunwald E. Shattuck lecture--cardiovascular medicine at the turn of the millennium: Triumphs, concerns, and opportunities. N Engl J Med. 1997;337:1360–1369. doi: 10.1056/NEJM199711063371906. [DOI] [PubMed] [Google Scholar]
- 2.Hunt SA. Acc/aha 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: A report of the american college of cardiology/american heart association task force on practice guidelines (writing committee to update the 2001 guidelines for the evaluation and management of heart failure) J Am Coll Cardiol. 2005;46:e1–82. doi: 10.1016/j.jacc.2005.08.022. [DOI] [PubMed] [Google Scholar]
- 3.Jessup M, Abraham WT, Casey DE, Feldman AM, Francis GS, Ganiats TG, Konstam MA, Mancini DM, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 focused update: Accf/aha guidelines for the diagnosis and management of heart failure in adults: A report of the american college of cardiology foundation/american heart association task force on practice guidelines: Developed in collaboration with the international society for heart and lung transplantation. Circulation. 2009;119:1977–2016. doi: 10.1161/CIRCULATIONAHA.109.192064. [DOI] [PubMed] [Google Scholar]
- 4.McKee PA, Castelli WP, McNamara PM, Kannel WB. The natural history of congestive heart failure: The framingham study. N Engl J Med. 1971;285:1441–1446. doi: 10.1056/NEJM197112232852601. [DOI] [PubMed] [Google Scholar]
- 5.Carlson KJ, Lee DC, Goroll AH, Leahy M, Johnson RA. An analysis of physicians’ reasons for prescribing long-term digitalis therapy in outpatients. J Chronic Dis. 1985;38:733–739. doi: 10.1016/0021-9681(85)90115-8. [DOI] [PubMed] [Google Scholar]
- 6.Eriksson H, Caidahl K, Larsson B, Ohlson LO, Welin L, Wilhelmsen L, Svardsudd K. Cardiac and pulmonary causes of dyspnoea--validation of a scoring test for clinical-epidemiological use: The study of men born in 1913. Eur Heart J. 1987;8:1007–1014. doi: 10.1093/oxfordjournals.eurheartj.a062365. [DOI] [PubMed] [Google Scholar]
- 7.Swedberg K, Cleland J, Dargie H, et al. Guidelines for the diagnosis and treatment of chronic heart failure: Executive summary (update 2005): The task force for the diagnosis and treatment of chronic heart failure of the european society of cardiology. Eur Heart J. 2005;26:1115–1140. doi: 10.1093/eurheartj/ehi204. [DOI] [PubMed] [Google Scholar]
- 8.Krumholz HM, Vaccarino V, Ellerbeck EF, Kiefe C, Hennen J, Kresowik TF, Gold JA, Jencks SF, Radford MJ. Determinants of appropriate use of angiotensin-converting enzyme inhibitors after acute myocardial infarction in persons > or = 65 years of age. Am J Cardiol. 1997;79:581–586. doi: 10.1016/s0002-9149(96)00819-3. [DOI] [PubMed] [Google Scholar]
- 9.Krumholz HM, Chen J, Chen YT, Wang Y, Radford MJ. Predicting one-year mortality among elderly survivors of hospitalization for an acute myocardial infarction: Results from the cooperative cardiovascular project. J Am Coll Cardiol. 2001;38:453–459. doi: 10.1016/s0735-1097(01)01395-x. [DOI] [PubMed] [Google Scholar]
- 10.Senni M, Rodeheffer RJ, Tribouilloy CM, Evans JM, Jacobsen SJ, Bailey KR, Redfield MM. Use of echocardiography in the management of congestive heart failure in the community. J Am Coll Cardiol. 1999;33:164–170. doi: 10.1016/s0735-1097(98)00523-3. [DOI] [PubMed] [Google Scholar]
- 11.Kurtz CE, Gerber Y, Weston SA, Redfield MM, Jacobsen SJ, Roger VL. Use of ejection fraction tests and coronary angiography in patients with heart failure. Mayo Clin Proc. 2006;81:906–913. doi: 10.4065/81.7.906. [DOI] [PubMed] [Google Scholar]
- 12.Gheorghiade M, Abraham WT, Albert NM, Greenberg BH, O’Connor CM, She L, Stough WG, Yancy CW, Young JB, Fonarow GC. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA : the journal of the American Medical Association. 2006;296:2217–2226. doi: 10.1001/jama.296.18.2217. [DOI] [PubMed] [Google Scholar]
- 13.Mosterd A, Deckers JW, Hoes AW, Nederpel A, Smeets A, Linker DT, Grobbee DE. Classification of heart failure in population based research: An assessment of six heart failure scores. Eur J Epidemiol. 1997;13:491–502. doi: 10.1023/a:1007383914444. [DOI] [PubMed] [Google Scholar]
- 14.Di Bari M, Pozzi C, Cavallini MC, Innocenti F, Baldereschi G, De Alfieri W, Antonini E, Pini R, Masotti G, Marchionni N. The diagnosis of heart failure in the community. Comparative validation of four sets of criteria in unselected older adults: The icare dicomano study. J Am Coll Cardiol. 2004;44:1601–1608. doi: 10.1016/j.jacc.2004.07.022. [DOI] [PubMed] [Google Scholar]
- 15.Schellenbaum GD, Rea TD, Heckbert SR, Smith NL, Lumley T, Roger VL, Kitzman DW, Taylor HA, Levy D, Psaty BM. Survival associated with two sets of diagnostic criteria for congestive heart failure. Am J Epidemiol. 2004;160:628–635. doi: 10.1093/aje/kwh268. [DOI] [PubMed] [Google Scholar]
- 16.Gheorghiade M, Zannad F, Sopko G, Klein L, Piña IL, Konstam MA, Massie BM, Roland E, Targum S, Collins SP, Filippatos G, Tavazzi L Syndromes ftIWGoAHF. Acute heart failure syndromes. Circulation. 2005;112:3958–3968. doi: 10.1161/CIRCULATIONAHA.105.590091. [DOI] [PubMed] [Google Scholar]
- 17.Rosamond WD, Chang PP, Baggett C, Johnson A, Bertoni AG, Shahar E, Deswal A, Heiss G, Chambless LE. Classification of heart failure in the atherosclerosis risk in communities (aric) study: A comparison of diagnostic criteria. Circ Heart Fail. 2012;5:152–159. doi: 10.1161/CIRCHEARTFAILURE.111.963199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Loehr LR, Agarwal SK, Baggett C, Wruck LM, Chang PP, Solomon SD, Shahar E, Ni H, Rosamond WD, Heiss G. Classification of acute decompensated heart failure (adhf): An automated algorithm compared to a physician reviewer panel: The aric study. Circ Heart Fail. 2013 doi: 10.1161/CIRCHEARTFAILURE.112.000195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vasan RS, Levy D. Defining diastolic heart failure: A call for standardized diagnostic criteria. Circulation. 2000;101:2118–2121. doi: 10.1161/01.cir.101.17.2118. [DOI] [PubMed] [Google Scholar]
- 20.Gottdiener JS, Livengood SV, Meyer PS, Chase GA. Should echocardiography be performed to assess effects of antihypertensive therapy? Test-retest reliability of echocardiography for measurement of left ventricular mass and function. J Am Coll Cardiol. 1995;25:424–430. doi: 10.1016/0735-1097(94)00375-z. [DOI] [PubMed] [Google Scholar]
- 21.Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD, Spencer KT, Sutton MS, Stewart WJ. Recommendations for chamber quantification: A report from the american society of echocardiography’s guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the european association of echocardiography, a branch of the european society of cardiology. J Am Soc Echocardiogr. 2005;18:1440–1463. doi: 10.1016/j.echo.2005.10.005. [DOI] [PubMed] [Google Scholar]
- 22.Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC. Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: A report from the acute decompensated heart failure national registry (adhere) database. J Am Coll Cardiol. 2006;47:76–84. doi: 10.1016/j.jacc.2005.09.022. [DOI] [PubMed] [Google Scholar]
- 23.Radford MJ, Arnold JM, Bennett SJ, et al. Acc/aha key data elements and definitions for measuring the clinical management and outcomes of patients with chronic heart failure: A report of the american college of cardiology/american heart association task force on clinical data standards (writing committee to develop heart failure clinical data standards): Developed in collaboration with the american college of chest physicians and the international society for heart and lung transplantation: Endorsed by the heart failure society of america. Circulation. 2005;112:1888–1916. doi: 10.1161/CIRCULATIONAHA.105.170073. [DOI] [PubMed] [Google Scholar]
- 24.Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. doi: 10.1056/NEJMoa052256. [DOI] [PubMed] [Google Scholar]
- 25.Senni M, Tribouilloy CM, Rodeheffer RJ, Jacobsen SJ, Evans JM, Bailey KR, Redfield MM. Congestive heart failure in the community: A study of all incident cases in olmsted county, minnesota, in 1991. Circulation. 1998;98:2282–2289. doi: 10.1161/01.cir.98.21.2282. [DOI] [PubMed] [Google Scholar]
- 26.Redfield MM, Jacobsen SJ, Burnett JC, Jr, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: Appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202. doi: 10.1001/jama.289.2.194. [DOI] [PubMed] [Google Scholar]
- 27.Hellermann JP, Goraya TY, Jacobsen SJ, Weston S, Reeder GS, Gersh BJ, Redfield MM, Rodeheffer R, Yawn BP, Roger VL. Incidence of heart failure after myocardial infarction: Is it changing over time? Am J Epidemiol. 2003;157:1101–1107. doi: 10.1093/aje/kwg078. [DOI] [PubMed] [Google Scholar]
- 28.Hellermann JP, Jacobsen SJ, Reeder GS, Lopez-Jimenez F, Weston SA, Roger VL. Heart failure after myocardial infarction: Prevalence of preserved left ventricular systolic function in the community. Am Heart J. 2003;145:742–748. doi: 10.1067/mhj.2003.187. [DOI] [PubMed] [Google Scholar]
- 29.Kitzman DW, Little WC, Brubaker PH, Anderson RT, Hundley WG, Marburger CT, Brosnihan B, Morgan TM, Stewart KP. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA. 2002;288:2144–2150. doi: 10.1001/jama.288.17.2144. [DOI] [PubMed] [Google Scholar]
- 30.Bursi F, Weston SA, Redfield MM, Jacobsen SJ, Pakhomov S, Nkomo VT, Meverden RA, Roger VL. Systolic and diastolic heart failure in the community. JAMA. 2006;296:2209–2216. doi: 10.1001/jama.296.18.2209. [DOI] [PubMed] [Google Scholar]
- 31.Vanderheyden M, Kersschot E, Paulus WJ. Pro-inflammatory cytokines and endothelium-dependent vasodilation in the forearm. Serial assessment in patients with congestive heart failure. Eur Heart J. 1998;19:747–752. doi: 10.1053/euhj.1997.0828. [DOI] [PubMed] [Google Scholar]
- 32.Yturralde RF, Gaasch WH. Diagnostic criteria for diastolic heart failure. Prog Cardiovasc Dis. 2005;47:314–319. doi: 10.1016/j.pcad.2005.02.007. [DOI] [PubMed] [Google Scholar]
- 33.Zile MR, Baicu CF, Gaasch WH. Diastolic heart failure--abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med. 2004;350:1953–1959. doi: 10.1056/NEJMoa032566. [DOI] [PubMed] [Google Scholar]
- 34.Aurigemma GP, Zile MR, Gaasch WH. Lack of relationship between doppler indices of diastolic function and left ventricular pressure transients in patients with definite diastolic heart failure. Am Heart J. 2004;148:E12. doi: 10.1016/j.ahj.2004.01.022. [DOI] [PubMed] [Google Scholar]
- 35.Little WC, Oh JK. Echocardiographic evaluation of diastolic function can be used to guide clinical care. Circulation. 2009;120:802–809. doi: 10.1161/CIRCULATIONAHA.109.869602. [DOI] [PubMed] [Google Scholar]
- 36.Tschope C, Paulus WJ. Is echocardiographic evaluation of diastolic function useful in determining clinical care? Doppler echocardiography yields dubious estimates of left ventricular diastolic pressures. Circulation. 2009;120:810–820. doi: 10.1161/CIRCULATIONAHA.109.869628. discussion 820. [DOI] [PubMed] [Google Scholar]
- 37.Tschope C, Kasner M, Westermann D, Gaub R, Poller WC, Schultheiss HP. The role of nt-probnp in the diagnostics of isolated diastolic dysfunction: Correlation with echocardiographic and invasive measurements. Eur Heart J. 2005;26:2277–2284. doi: 10.1093/eurheartj/ehi406. [DOI] [PubMed] [Google Scholar]
- 38.Rosen BD, Edvardsen T, Lai S, Castillo E, Pan L, Jerosch-Herold M, Sinha S, Kronmal R, Arnett D, Crouse JR, 3rd, Heckbert SR, Bluemke DA, Lima JA. Left ventricular concentric remodeling is associated with decreased global and regional systolic function: The multi-ethnic study of atherosclerosis. Circulation. 2005;112:984–991. doi: 10.1161/CIRCULATIONAHA104.500488. [DOI] [PubMed] [Google Scholar]
- 39.Steeds RP. Multimodality imaging in heart failure patients. Curr Opin Cardiol. 2013;28:209–215. doi: 10.1097/HCO.0b013e32835bc1b5. [DOI] [PubMed] [Google Scholar]
- 40.Lorenz CH, Flacke S, Fischer SE. Noninvasive modalities. Cardiac mr imaging. Cardiol Clin. 2000;18:557–570. doi: 10.1016/s0733-8651(05)70161-2. [DOI] [PubMed] [Google Scholar]
- 41.Prasad SK, Kotwinski P, Assomul R. The role of cardiovascular magnetic resonance in the evaluation of patients with heart failure. Expert Rev Cardiovasc Ther. 2004;2:53–59. doi: 10.1586/14779072.2.1.53. [DOI] [PubMed] [Google Scholar]
- 42.Joint commission on accreditation of health care organizations. Specification manual for national implementation of hospital core measures: Version 2.0-implementation to begin with july 2004 discharges. 2004;2005 [Google Scholar]
- 43.Cahill JM, Horan M, Quigley P, Maurer B, McDonald K. Doppler-echocardiographic indices of diastolic function in heart failure admissions with preserved left ventricular systolic function. Eur J Heart Fail. 2002;4:473–478. doi: 10.1016/s1388-9842(02)00023-5. [DOI] [PubMed] [Google Scholar]
- 44.Petrie MC, Hogg K, Caruana L, McMurray JJ. Poor concordance of commonly used echocardiographic measures of left ventricular diastolic function in patients with suspected heart failure but preserved systolic function: Is there a reliable echocardiographic measure of diastolic dysfunction? Heart. 2004;90:511–517. doi: 10.1136/hrt.2003.011403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Sohn DW, Chai IH, Lee DJ, Kim HC, Kim HS, Oh BH, Lee MM, Park YB, Choi YS, Seo JD, Lee YW. Assessment of mitral annulus velocity by doppler tissue imaging in the evaluation of left ventricular diastolic function. J Am Coll Cardiol. 1997;30:474–480. doi: 10.1016/s0735-1097(97)88335-0. [DOI] [PubMed] [Google Scholar]
- 46.Garcia MJ, Thomas JD, Klein AL. New doppler echocardiographic applications for the study of diastolic function. J Am Coll Cardiol. 1998;32:865–875. doi: 10.1016/s0735-1097(98)00345-3. [DOI] [PubMed] [Google Scholar]
- 47.Ommen SR, Nishimura RA, Appleton CP, Miller FA, Oh JK, Redfield MM, Tajik AJ. Clinical utility of doppler echocardiography and tissue doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous doppler-catheterization study. Circulation. 2000;102:1788–1794. doi: 10.1161/01.cir.102.15.1788. [DOI] [PubMed] [Google Scholar]
- 48.Dokainish H, Zoghbi WA, Lakkis NM, Al-Bakshy F, Dhir M, Quinones MA, Nagueh SF. Optimal noninvasive assessment of left ventricular filling pressures: A comparison of tissue doppler echocardiography and b-type natriuretic peptide in patients with pulmonary artery catheters. Circulation. 2004;109:2432–2439. doi: 10.1161/01.CIR.0000127882.58426.7A. [DOI] [PubMed] [Google Scholar]
- 49.Dokainish H. Tissue doppler imaging in the evaluation of left ventricular diastolic function. Curr Opin Cardiol. 2004;19:437–441. doi: 10.1097/01.hco.0000131538.55528.8f. [DOI] [PubMed] [Google Scholar]
- 50.Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA. Doppler tissue imaging: A noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol. 1997;30:1527–1533. doi: 10.1016/s0735-1097(97)00344-6. [DOI] [PubMed] [Google Scholar]
- 51.Quinones MA. Assessment of diastolic function. Prog Cardiovasc Dis. 2005;47:340–355. doi: 10.1016/j.pcad.2005.02.009. [DOI] [PubMed] [Google Scholar]
- 52.Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, Evangelisa A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. Eur J Echocardiogr. 2009;10:165–193. doi: 10.1093/ejechocard/jep007. [DOI] [PubMed] [Google Scholar]
- 53.Kawaguchi M, Hay I, Fetics B, Kass DA. Combined ventricular systolic and arterial stiffening in patients with heart failure and preserved ejection fraction: Implications for systolic and diastolic reserve limitations. Circulation. 2003;107:714–720. doi: 10.1161/01.cir.0000048123.22359.a0. [DOI] [PubMed] [Google Scholar]
- 54.Burkhoff D, Maurer MS, Packer M. Heart failure with a normal ejection fraction: Is it really a disorder of diastolic function? Circulation. 2003;107:656–658. doi: 10.1161/01.cir.0000053947.82595.03. [DOI] [PubMed] [Google Scholar]
- 55.Hundley WG, Kitzman DW, Morgan TM, Hamilton CA, Darty SN, Stewart KP, Herrington DM, Link KM, Little WC. Cardiac cycle-dependent changes in aortic area and distensibility are reduced in older patients with isolated diastolic heart failure and correlate with exercise intolerance. J Am Coll Cardiol. 2001;38:796–802. doi: 10.1016/s0735-1097(01)01447-4. [DOI] [PubMed] [Google Scholar]
- 56.Maurer MS, King DL, El-Khoury Rumbarger L, Packer M, Burkhoff D. Left heart failure with a normal ejection fraction: Identification of different pathophysiologic mechanisms. J Card Fail. 2005;11:177–187. doi: 10.1016/j.cardfail.2004.10.006. [DOI] [PubMed] [Google Scholar]
- 57.Lam CS, Roger VL, Rodeheffer RJ, Borlaug BA, Enders FT, Redfield MM. Pulmonary hypertension in heart failure with preserved ejection fraction: A community-based study. J Am Coll Cardiol. 2009;53:1119–1126. doi: 10.1016/j.jacc.2008.11.051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Kass DA, Bronzwaer JG, Paulus WJ. What mechanisms underlie diastolic dysfunction in heart failure? Circ Res. 2004;94:1533–1542. doi: 10.1161/01.RES.0000129254.25507.d6. [DOI] [PubMed] [Google Scholar]
- 59.Hunt SA, Abraham WT, Chin MH, et al. Acc/aha 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: A report of the american college of cardiology/american heart association task force on practice guidelines (writing committee to update the 2001 guidelines for the evaluation and management of heart failure): Developed in collaboration with the american college of chest physicians and the international society for heart and lung transplantation: Endorsed by the heart rhythm society. Circulation. 2005;112:e154–235. doi: 10.1161/CIRCULATIONAHA.105.167586. [DOI] [PubMed] [Google Scholar]
- 60.Hunt SA, Abraham WT, Chin MH, et al. 2009 focused update incorporated into the acc/aha 2005 guidelines for the diagnosis and management of heart failure in adults a report of the american college of cardiology foundation/american heart association task force on practice guidelines developed in collaboration with the international society for heart and lung transplantation. J Am Coll Cardiol. 2009;53:e1–e90. doi: 10.1016/j.jacc.2008.11.013. [DOI] [PubMed] [Google Scholar]
- 61.Assaf AR, Lapane KL, McKenney JL, Carleton RA. Possible influence of the prospective payment system on the assignment of discharge diagnoses for coronary heart disease. N Engl J Med. 1993;329:931–935. doi: 10.1056/NEJM199309233291307. [DOI] [PubMed] [Google Scholar]
- 62.Jollis JG, Ancukiewicz M, DeLong ER, Pryor DB, Muhlbaier LH, Mark DB. Discordance of databases designed for claims payment versus clinical information systems. Implications for outcomes research. Ann Intern Med. 1993;119:844–850. doi: 10.7326/0003-4819-119-8-199310150-00011. [DOI] [PubMed] [Google Scholar]
- 63.Carleton R. Trends and determinants in coronary heart disease mortality: Future prospects and projections. In: Higgins MW, Luepker RV, editors. Trends in coronary heart disease mortality: The influence of medical care. New York, NY: Oxford University Press; 1988. pp. 270–275. [Google Scholar]
- 64.Psaty BM, Kuller LH, Bild D, Burke GL, Kittner SJ, Mittelmark M, Price TR, Rautaharju PM, Robbins J. Methods of assessing prevalent cardiovascular disease in the cardiovascular health study. Ann Epidemiol. 1995;5:270–277. doi: 10.1016/1047-2797(94)00092-8. [DOI] [PubMed] [Google Scholar]
- 65.Guidelines for the diagnosis of heart failure. The task force on heart failure of the european society of cardiology. Eur Heart J. 1995;16:741–751. [PubMed] [Google Scholar]
- 66.Senni M, Tribouilloy CM, Rodeheffer RJ, Jacobsen SJ, Evans JM, Bailey KR, Redfield MM. Congestive heart failure in the community: Trends in incidence and survival in a 10-year period. Arch Intern Med. 1999;159:29–34. doi: 10.1001/archinte.159.1.29. [DOI] [PubMed] [Google Scholar]
- 67.Croft JB, Giles WH, Pollard RA, Casper ML, Anda RF, Livengood JR. National trends in the initial hospitalization for heart failure. J Am Geriatr Soc. 1997;45:270–275. doi: 10.1111/j.1532-5415.1997.tb00939.x. [DOI] [PubMed] [Google Scholar]
- 68.Stewart S, MacIntyre K, MacLeod MM, Bailey AE, Capewell S, McMurray JJ. Trends in hospital activity, morbidity and case fatality related to atrial fibrillation in scotland, 1986--1996. Eur Heart J. 2001;22:693–701. doi: 10.1053/euhj.2000.2511. [DOI] [PubMed] [Google Scholar]
- 69.Stewart S, MacIntyre K, MacLeod MM, Bailey AE, Capewell S, McMurray JJ. Trends in hospitalization for heart failure in scotland, 1990-1996. An epidemic that has reached its peak? Eur Heart J. 2001;22:209–217. doi: 10.1053/euhj.2000.2291. [DOI] [PubMed] [Google Scholar]
- 70.Stewart WJ, Currie PJ, Salcedo EE, Lytle BW, Gill CC, Schiavone WA, Agler DA, Cosgrove DM. Intraoperative doppler color flow mapping for decision-making in valve repair for mitral regurgitation. Technique and results in 100 patients. Circulation. 1990;81:556–566. doi: 10.1161/01.cir.81.2.556. [DOI] [PubMed] [Google Scholar]
- 71.McCullough PA, Philbin EF, Spertus JA, Kaatz S, Sandberg KR, Weaver WD. Confirmation of a heart failure epidemic: Findings from the resource utilization among congestive heart failure (reach) study. J Am Coll Cardiol. 2002;39:60–69. doi: 10.1016/s0735-1097(01)01700-4. [DOI] [PubMed] [Google Scholar]
- 72.Roger VL, Weston SA, Redfield MM, Hellermann-Homan JP, Killian J, Yawn BP, Jacobsen SJ. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292:344–350. doi: 10.1001/jama.292.3.344. [DOI] [PubMed] [Google Scholar]
- 73.Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, Murabito JM, Vasan RS. Long-term trends in the incidence of and survival with heart failure. N Engl J Med. 2002;347:1397–1402. doi: 10.1056/NEJMoa020265. [DOI] [PubMed] [Google Scholar]
- 74.Barker WH, Mullooly JP, Getchell W. Changing incidence and survival for heart failure in a well-defined older population, 1970-1974 and 1990-1994. Circulation. 2006;113:799–805. doi: 10.1161/CIRCULATIONAHA.104.492033. [DOI] [PubMed] [Google Scholar]
- 75.Yeung DF, Boom NK, Guo H, Lee DS, Schultz SE, Tu JV. Trends in the incidence and outcomes of heart failure in ontario, canada: 1997 to 2007. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne. 2012;184:E765–773. doi: 10.1503/cmaj.111958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Jhund PS, Macintyre K, Simpson CR, Lewsey JD, Stewart S, Redpath A, Chalmers JW, Capewell S, McMurray JJ. Long-term trends in first hospitalization for heart failure and subsequent survival between 1986 and 2003: A population study of 5.1 million people. Circulation. 2009;119:515–523. doi: 10.1161/CIRCULATIONAHA.108.812172. [DOI] [PubMed] [Google Scholar]
- 77.Loehr LR, Rosamond WD, Chang PP, Folsom AR, Chambless LE. Heart failure incidence and survival (from the atherosclerosis risk in communities study) Am J Cardiol. 2008;101:1016–1022. doi: 10.1016/j.amjcard.2007.11.061. [DOI] [PubMed] [Google Scholar]
- 78.Bahrami H, Kronmal R, Bluemke DA, Olson J, Shea S, Liu K, Burke GL, Lima JA. Differences in the incidence of congestive heart failure by ethnicity: The multi-ethnic study of atherosclerosis. Arch Intern Med. 2008;168:2138–2145. doi: 10.1001/archinte.168.19.2138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Psaty BM, Boineau R, Kuller LH, Luepker RV. The potential costs of upcoding for heart failure in the united states. Am J Cardiol. 1999;84:108–109. A109. doi: 10.1016/s0002-9149(99)00205-2. [DOI] [PubMed] [Google Scholar]
- 80.Goldberg RJ, Konstam MA. Assessing the population burden from heart failure: Need for sentinel population-based surveillance systems. Arch Intern Med. 1999;159:15–17. doi: 10.1001/archinte.159.1.15. [DOI] [PubMed] [Google Scholar]
- 81.Lloyd-Jones DM, Leip EP, Larson MG, D’Agostino RB, Beiser A, Wilson PW, Wolf PA, Levy D. Prediction of lifetime risk for cardiovascular disease by risk factor burden at 50 years of age. Circulation. 2006;113:791–798. doi: 10.1161/CIRCULATIONAHA.105.548206. [DOI] [PubMed] [Google Scholar]
- 82.Lloyd-Jones DM, Larson MG, Leip EP, Beiser A, D’Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ, Levy D. Lifetime risk for developing congestive heart failure: The framingham heart study. Circulation. 2002;106:3068–3072. doi: 10.1161/01.cir.0000039105.49749.6f. [DOI] [PubMed] [Google Scholar]
- 83.Huffman MD, Berry JD, Ning H, Dyer AR, Garside DB, Cai X, Daviglus ML, Lloyd-Jones DM. Lifetime risk for heart failure among white and black americans: Cardiovascular lifetime risk pooling project. J Am Col Cardiol. 2013;61:1510–1517. doi: 10.1016/j.jacc.2013.01.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Bleumink GS, Knetsch AM, Sturkenboom MC, Straus SM, Hofman A, Deckers JW, Witteman JC, Stricker BH. Quantifying the heart failure epidemic: Prevalence, incidence rate, lifetime risk and prognosis of heart failure the rotterdam study. Eur Heart J. 2004;25:1614–1619. doi: 10.1016/j.ehj.2004.06.038. [DOI] [PubMed] [Google Scholar]
- 85.MacIntyre K, Capewell S, Stewart S, Chalmers JW, Boyd J, Finlayson A, Redpath A, Pell JP, McMurray JJ. Evidence of improving prognosis in heart failure: Trends in case fatality in 66 547 patients hospitalized between 1986 and 1995. Circulation. 2000;102:1126–1131. doi: 10.1161/01.cir.102.10.1126. [DOI] [PubMed] [Google Scholar]
- 86.Mosterd A, Cost B, Hoes AW, de Bruijne MC, Deckers JW, Hofman A, Grobbee DE. The prognosis of heart failure in the general population: The rotterdam study. Eur Heart J. 2001;22:1318–1327. doi: 10.1053/euhj.2000.2533. [DOI] [PubMed] [Google Scholar]
- 87.Cowie MR, Wood DA, Coats AJ, Thompson SG, Suresh V, Poole-Wilson PA, Sutton GC. Survival of patients with a new diagnosis of heart failure: A population based study. Heart. 2000;83:505–510. doi: 10.1136/heart.83.5.505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Chugh SS, Reinier K, Teodorescu C, Evanado A, Kehr E, Al Samara M, Mariani R, Gunson K, Jui J. Epidemiology of sudden cardiac death: Clinical and research implications. Prog Cardiovasc Dis. 2008;51:213–228. doi: 10.1016/j.pcad.2008.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Flather MD, Yusuf S, Kober L, Pfeffer M, Hall A, Murray G, Torp-Pedersen C, Ball S, Pogue J, Moye L, Braunwald E. Long-term ace-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: A systematic overview of data from individual patients. Ace-inhibitor myocardial infarction collaborative group. Lancet. 2000;355:1575–1581. doi: 10.1016/s0140-6736(00)02212-1. [DOI] [PubMed] [Google Scholar]
- 90.Curtis LH, Whellan DJ, Hammill BG, Hernandez AF, Anstrom KJ, Shea AM, Schulman KA. Incidence and prevalence of heart failure in elderly persons, 1994-2003. Arch Intern Med. 2008;168:418–424. doi: 10.1001/archinternmed.2007.80. [DOI] [PubMed] [Google Scholar]
- 91.Chin MH, Goldman L. Correlates of early hospital readmission or death in patients with congestive heart failure. Am J Cardiol. 1997;79:1640–1644. doi: 10.1016/s0002-9149(97)00214-2. [DOI] [PubMed] [Google Scholar]
- 92.Krumholz HM, Parent EM, Tu N, Vaccarino V, Wang Y, Radford MJ, Hennen J. Readmission after hospitalization for congestive heart failure among medicare beneficiaries. Arch Intern Med. 1997;157:99–104. [PubMed] [Google Scholar]
- 93.Krumholz HM, Wang Y, Parent EM, Mockalis J, Petrillo M, Radford MJ. Quality of care for elderly patients hospitalized with heart failure. Arch Intern Med. 1997;157:2242–2247. [PubMed] [Google Scholar]
- 94.Struthers AD. The diagnosis of heart failure. Heart. 2000;84:334–338. doi: 10.1136/heart.84.3.334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Struthers AD, Anderson G, Donnan PT, MacDonald T. Social deprivation increases cardiac hospitalisations in chronic heart failure independent of disease severity and diuretic non-adherence. Heart. 2000;83:12–16. doi: 10.1136/heart.83.1.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Henkel DM, Redfield MM, Weston SA, Gerber Y, Roger VL. Death in heart failure: A community perspective. Circ Heart Fail. 2008;1:91–97. doi: 10.1161/CIRCHEARTFAILURE.107.743146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics--2012 update: A report from the american heart association. Circulation. 2012;125:e2–e220. doi: 10.1161/CIR.0b013e31823ac046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Chen J, Normand SL, Wang Y, Krumholz HM. National and regional trends in heart failure hospitalization and mortality rates for medicare beneficiaries, 1998-2008. JAMA. 2011;306:1669–1678. doi: 10.1001/jama.2011.1474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Bueno H, Ross JS, Wang Y, Chen J, Vidan MT, Normand SL, Curtis JP, Drye EE, Lichtman JH, Keenan PS, Kosiborod M, Krumholz HM. Trends in length of stay and short-term outcomes among medicare patients hospitalized for heart failure, 1993-2006. JAMA. 2010;303:2141–2147. doi: 10.1001/jama.2010.748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Dharmarajan K, Hsieh AF, Lin Z, Bueno H, Ross JS, Horwitz LI, Barreto-Filho JA, Kim N, Bernheim SM, Suter LG, Drye EE, Krumholz HM. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA : the journal of the American Medical Association. 2013;309:355–363. doi: 10.1001/jama.2012.216476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Heidenreich PA, Sahay A, Kapoor JR, Pham MX, Massie B. Divergent trends in survival and readmission following a hospitalization for heart failure in the veterans affairs health care system 2002 to 2006. J Am Coll Cardiol. 2010;56:362–368. doi: 10.1016/j.jacc.2010.02.053. [DOI] [PubMed] [Google Scholar]
- 102.Joynt KE, Jha AK. A path forward on medicare readmissions. N Engl J Med. 2013 doi: 10.1056/NEJMp1300122. In press. [DOI] [PubMed] [Google Scholar]
- 103.Joynt KE, Jha AK. Thirty-day readmissions--truth and consequences. N Engl J Med. 2012;366:1366–1369. doi: 10.1056/NEJMp1201598. [DOI] [PubMed] [Google Scholar]
- 104.Xian Y, Hammill BG, Curtis LH. Data sources for heart failure comparative effectiveness research. Heart Fail Clin. 2013;9:1–13. doi: 10.1016/j.hfc.2012.09.001. [DOI] [PubMed] [Google Scholar]
- 105.Fonarow GC, Abraham WT, Albert NM, Gattis WA, Gheorghiade M, Greenberg B, O’Connor CM, Yancy CW, Young J. Organized program to initiate lifesaving treatment in hospitalized patients with heart failure (optimize-hf): Rationale and design. Am Heart J. 2004;148:43–51. doi: 10.1016/j.ahj.2004.03.004. [DOI] [PubMed] [Google Scholar]
- 106.Hong Y, LaBresh KA. Overview of the american heart association “get with the guidelines” programs: Coronary heart disease, stroke, and heart failure. Crit Pathw Cardiol. 2006;5:179–186. doi: 10.1097/01.hpc.0000243588.00012.79. [DOI] [PubMed] [Google Scholar]
- 107.West R, Liang L, Fonarow GC, Kociol R, Mills RM, O’Connor CM, Hernandez AF. Characterization of heart failure patients with preserved ejection fraction: A comparison between adhere-us registry and adhere-international registry. Eur J Heart Fail. 2011;13:945–952. doi: 10.1093/eurjhf/hfr064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the u.S., 1979 to 2004. J Am Coll Cardiol. 2008;52:428–434. doi: 10.1016/j.jacc.2008.03.061. [DOI] [PubMed] [Google Scholar]
- 109.Dunlay SM, Redfield MM, Weston SA, Therneau TM, Hall Long K, Shah ND, Roger VL. Hospitalizations after heart failure diagnosis a community perspective. J Am Coll Cardiol. 2009;54:1695–1702. doi: 10.1016/j.jacc.2009.08.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Roger VL. The changing landscape of heart failure hospitalizations. J Am Coll Cardiol. 2013;61:1268–1270. doi: 10.1016/j.jacc.2013.01.011. [DOI] [PubMed] [Google Scholar]
- 111.Blecker S, Paul M, Taksler G, Ogedegbe G, Katz S. Heart failure associated hospitalizations in the united states. J Am Coll Cardiol. 2013;61:1259–1267. doi: 10.1016/j.jacc.2012.12.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK. The progression from hypertension to congestive heart failure. JAMA. 1996;275:1557–1562. [PubMed] [Google Scholar]
- 113.Dunlay SM, Weston SA, Jacobsen SJ, Roger VL. Risk factors for heart failure: A population-based case-control study. Am J Med. 2009;122:1023–1028. doi: 10.1016/j.amjmed.2009.04.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Fox KF, Cowie MR, Wood DA, Coats AJ, Gibbs JS, Underwood SR, Turner RM, Poole-Wilson PA, Davies SW, Sutton GC. Coronary artery disease as the cause of incident heart failure in the population. Eur Heart J. 2001;22:228–236. doi: 10.1053/euhj.2000.2289. [DOI] [PubMed] [Google Scholar]
- 115.Gheorghiade M, Bonow RO. Chronic heart failure in the united states: A manifestation of coronary artery disease. Circulation. 1998;97:282–289. doi: 10.1161/01.cir.97.3.282. [DOI] [PubMed] [Google Scholar]
- 116.McMurray JJ, Stewart S. Epidemiology, aetiology, and prognosis of heart failure. Heart. 2000;83:596–602. doi: 10.1136/heart.83.5.596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Lindenfeld J, Krause-Steinrauf H, Salerno J. Where are all the women with heart failure? J Am Coll Cardiol. 1997;30:1417–1419. doi: 10.1016/s0735-1097(97)00343-4. [DOI] [PubMed] [Google Scholar]
- 118.Marantz PR, Alderman MH, Tobin JN. Diagnostic heterogeneity in clinical trials for congestive heart failure. Ann Intern Med. 1988;109:55–61. doi: 10.7326/0003-4819-109-1-55. [DOI] [PubMed] [Google Scholar]
- 119.Devereux RB, Roman MJ, Liu JE, Welty TK, Lee ET, Rodeheffer R, Fabsitz RR, Howard BV. Congestive heart failure despite normal left ventricular systolic function in a population-based sample: The strong heart study. Am J Cardiol. 2000;86:1090–1096. doi: 10.1016/s0002-9149(00)01165-6. [DOI] [PubMed] [Google Scholar]
- 120.Teerlink JR, Goldhaber SZ, Pfeffer MA. An overview of contemporary etiologies of congestive heart failure. Am Heart J. 1991;121:1852–1853. doi: 10.1016/0002-8703(91)90072-p. [DOI] [PubMed] [Google Scholar]
- 121.Cowie MR, Wood DA, Coats AJ, Thompson SG, Poole-Wilson PA, Suresh V, Sutton GC. Incidence and aetiology of heart failure; a population-based study. Eur Heart J. 1999;20:421–428. doi: 10.1053/euhj.1998.1280. [DOI] [PubMed] [Google Scholar]
- 122.He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in us men and women: Nhanes i epidemiologic follow-up study. Arch Intern Med. 2001;161:996–1002. doi: 10.1001/archinte.161.7.996. [DOI] [PubMed] [Google Scholar]
- 123.Gottdiener JS, Arnold AM, Aurigemma GP, Polak JF, Tracy RP, Kitzman DW, Gardin JM, Rutledge JE, Boineau RC. Predictors of congestive heart failure in the elderly: The cardiovascular health study. J Am Coll Cardiol. 2000;35:1628–1637. doi: 10.1016/s0735-1097(00)00582-9. [DOI] [PubMed] [Google Scholar]
- 124.Levy JA. Surrogate markers in aids research. Is there truth in numbers? JAMA. 1996;276:161–162. [PubMed] [Google Scholar]
- 125.Levy EM, Viscoli CM, Horwitz RI. The effect of acute renal failure on mortality. A cohort analysis. JAMA. 1996;275:1489–1494. [PubMed] [Google Scholar]
- 126.Levy CE, Clinchot DM, Bowyer BL, Pease WS. A 50-year-old woman with spinal stenosis. JAMA. 1996;275:1400–1401. doi: 10.1001/jama.1996.03530420028025. discussion 1401-1402. [DOI] [PubMed] [Google Scholar]
- 127.Kannel WB, Ho K, Thom T. Changing epidemiological features of cardiac failure. Br Heart J. 1994;72:S3–9. doi: 10.1136/hrt.72.2_suppl.s3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 128.Yeh RW, Sidney S, Chandra M, Sorel M, Selby JV, Go AS. Population trends in the incidence and outcomes of acute myocardial infarction. N Engl J Med. 2010;362:2155–2165. doi: 10.1056/NEJMoa0908610. [DOI] [PubMed] [Google Scholar]
- 129.Roger VL, Weston SA, Gerber Y, Killian JM, Dunlay SM, Jaffe AS, Bell MR, Kors J, Yawn BP, Jacobsen SJ. Trends in incidence, severity, and outcome of hospitalized myocardial infarction. Circulation. 2010;121:863–869. doi: 10.1161/CIRCULATIONAHA.109.897249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Rosamond WD, Chambless LE, Heiss G, Mosley TH, Coresh J, Whitsel E, Wagenknecht L, Ni H, Folsom AR. Twenty-two-year trends in incidence of myocardial infarction, coronary heart disease mortality, and case fatality in 4 us communities, 1987-2008. Circulation. 2012;125:1848–1857. doi: 10.1161/CIRCULATIONAHA.111.047480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Velagaleti RS, Pencina MJ, Murabito JM, Wang TJ, Parikh NI, D’Agostino RB, Levy D, Kannel WB, Vasan RS. Long-term trends in the incidence of heart failure after myocardial infarction. Circulation. 2008;118:2057–2062. doi: 10.1161/CIRCULATIONAHA.108.784215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132.Shafazand M, Rosengren A, Lappas G, Swedberg K, Schaufelberger M. Decreasing trends in the incidence of heart failure after acute myocardial infarction from 1993-2004: A study of 175,216 patients with a first acute myocardial infarction in sweden. Eur J Heart Fail. 2011;13:135–141. doi: 10.1093/eurjhf/hfq205. [DOI] [PubMed] [Google Scholar]
- 133.Nguyen HL, Saczynski JS, Gore JM, Waring ME, Lessard D, Yarzebski J, Reed G, Spencer FA, Li SX, Goldberg RJ. Long-term trends in short-term outcomes in acute myocardial infarction. Am J Med. 2011;124:939–946. doi: 10.1016/j.amjmed.2011.05.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.The sixth report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med. 1997;157:2413–2446. doi: 10.1001/archinte.157.21.2413. [DOI] [PubMed] [Google Scholar]
- 135.Meissner I, Whisnant JP, Sheps SG, Schwartz GL, O’Fallon WM, Covalt JL, Sicks JD, Bailey KR, Wiebers DO. Detection and control of high blood pressure in the community : Do we need a wake-up call? Hypertension. 1999;34:466–471. doi: 10.1161/01.hyp.34.3.466. [DOI] [PubMed] [Google Scholar]
- 136.Leibson CL, O’Brien PC, Atkinson E, Palumbo PJ, Melton LJ., 3rd Relative contributions of incidence and survival to increasing prevalence of adult-onset diabetes mellitus: A population-based study. Am J Epidemiol. 1997;146:12–22. doi: 10.1093/oxfordjournals.aje.a009187. [DOI] [PubMed] [Google Scholar]
- 137.Mokdad AH, Bowman BA, Ford ES, Vinicor F, Marks JS, Koplan JP. The continuing epidemics of obesity and diabetes in the united states. JAMA. 2001;286:1195–1200. doi: 10.1001/jama.286.10.1195. [DOI] [PubMed] [Google Scholar]
- 138.Eckel RH. Obesity and heart disease: A statement for healthcare professionals from the nutrition committee, american heart association. Circulation. 1997;96:3248–3250. doi: 10.1161/01.cir.96.9.3248. [DOI] [PubMed] [Google Scholar]
- 139.Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: A 26- year follow-up of participants in the framingham heart study. Circulation. 1983;67:968–977. doi: 10.1161/01.cir.67.5.968. [DOI] [PubMed] [Google Scholar]
- 140.Iribarren C, Karter AJ, Go AS, Ferrara A, Liu JY, Sidney S, Selby JV. Glycemic control and heart failure among adult patients with diabetes. Circulation. 2001;103:2668–2673. doi: 10.1161/01.cir.103.22.2668. [DOI] [PubMed] [Google Scholar]
- 141.Bell DS. Diabetic cardiomyopathy. A unique entity or a complication of coronary artery disease? Diabetes Care. 1995;18:708–714. doi: 10.2337/diacare.18.5.708. [DOI] [PubMed] [Google Scholar]
- 142.Nichols GA, Hillier TA, Erbey JR, Brown JB. Congestive heart failure in type 2 diabetes: Prevalence, incidence, and risk factors. Diabetes Care. 2001;24:1614–1619. doi: 10.2337/diacare.24.9.1614. [DOI] [PubMed] [Google Scholar]
- 143.Avery CL, Loehr LR, Baggett C, Chang PP, Kucharska-Newton AM, Matsushita K, Rosamond WD, Heiss G. The population burden of heart failure attributable to modifiable risk factors: The aric (atherosclerosis risk in communities) study. J Am Coll Cardiol. 2012;60:1640–1646. doi: 10.1016/j.jacc.2012.07.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Loehr LR, Rosamond WD, Poole C, McNeill AM, Chang PP, Deswal A, Folsom AR, Heiss G. The potentially modifiable burden of incident heart failure due to obesity: The atherosclerosis risk in communities study. Am J Epidemiol. 2010;172:781–789. doi: 10.1093/aje/kwq213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 145.Schocken DD, Arrieta MI, Leaverton PE, Ross EA. Prevalence and mortality rate of congestive heart failure in the united states. J Am Coll Cardiol. 1992;20:301–306. doi: 10.1016/0735-1097(92)90094-4. [DOI] [PubMed] [Google Scholar]
- 146.Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics--2013 update: A report from the american heart association. Circulation. 2013;127:e6–e245. doi: 10.1161/CIR.0b013e31828124ad. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Goldberg RJ, Spencer FA, Farmer C, Meyer TE, Pezzella S. Incidence and hospital death rates associated with heart failure: A community-wide perspective. Am J Med. 2005;118:728–734. doi: 10.1016/j.amjmed.2005.04.013. [DOI] [PubMed] [Google Scholar]
- 148.Remes J, Reunanen A, Aromaa A, Pyorala K. Incidence of heart failure in eastern finland: A population-based surveillance study. Eur Heart J. 1992;13:588–593. doi: 10.1093/oxfordjournals.eurheartj.a060220. [DOI] [PubMed] [Google Scholar]
- 149.Nielsen OW, Hilden J, Larsen CT, Hansen JF. Cross sectional study estimating prevalence of heart failure and left ventricular systolic dysfunction in community patients at risk. Heart. 2001;86:172–178. doi: 10.1136/heart.86.2.172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Davies M, Hobbs F, Davis R, Kenkre J, Roalfe AK, Hare R, Wosornu D, Lancashire RJ. Prevalence of left-ventricular systolic dysfunction and heart failure in the echocardiographic heart of england screening study: A population based study. Lancet. 2001;358:439–444. doi: 10.1016/s0140-6736(01)05620-3. [DOI] [PubMed] [Google Scholar]