

Abstract
Objective:
The present study intends to evaluate the relationship between Sthaulya (obesity) and Kṛcchra Vyavāya (sexual dysfunction) with respect to different phases of sexual intercourse through a single-centered, observational study in male patients of obesity.
Materials and Methods:
The study involved 33 obese males from the outpatient department of the Institution whose sexual functioning was assessed using an International Index of Erectile Function questionnaire, which was meant to assess five specific areas of sexual functioning.
Results:
A varying degree of sexual dysfunction was observed in four out of five areas of sexual functioning viz. erectile function (P < 0.02), orgasmic function (P < 0.02), sexual desire (P < 0.08), and overall satisfaction (P < 0.000) in obese individuals. Statistically significant dysfunction was not observed in intercourse satisfaction.
Conclusions:
Varying degree of sexual dysfunction is present in obese males, suggesting that obesity has a possible role in reducing the quality of sexual functioning in males as indicated in the classical ayurvedic literature.
KEY WORDS: Erectile dysfunction, Kṛcchra Vyavāya, obesity, Sthaulya, Vyavāya
INTRODUCTION
Obesity has increased at an alarming rate in recent years and has become one of the major health hazards globally. The increasing prevalence of obesity is currently viewed as one of the serious health problems of 21st century.[3] Obesity is significantly associated with erectile dysfunction (ED) and this has been neither in the focus of medical practitioners nor researchers. Studies show that obese males have a 30% higher chance of developing sexual dysfunction than the people of normal weight. It is also noteworthy that there is significant information available in the classical literature of āyurveda regarding the relationship between obesity and sexual functioning. Obesity is described as ‘Sthaulya” and difficulty in performing sexual act is termed as “Kṛcchra Vyavāya.” Caraka saṃhita clearly states the relationship between “Sthaulya” and “Kṛcchra Vyavāya.”[1]
Sthaulya is a medical condition characterized by excessive accumulation of medas (fat) in the body, especially in the areas of sphik (buttocks), stana (breasts), and udara (abdomen).[2] Overweight and obesity are the two medical conditions described in biomedical science which are equivalent to “Sthaulya.” Quite a number of clinical and research studies are being conducted over the past 2 to 3 decades to understand the role of obesity as a risk factor in various disorders.
The relation between obesity and sexual dysfunction is not understood completely till date. Though some studies suggest that obesity is associated with low androgen levels in men with ED, researches in this direction are few and far between.[4] ED is one of the most common chronic disorders affecting more than 100 million men worldwide.[5] The prevalence of overweight or obesity in men reporting symptoms of ED is as high as 79%.[6] Changing cultural attitudes and demographic shifts in the population have highlighted the pervasiveness of sexual concerns in all ethnic and age groups.[7]
Interestingly, the link between obesity and sexual dysfunction has been emphasized in the classical text of ayurveda “Caraka saṃhitā.”[1]
“Ati sthūlasya tāvadāyuṣo hrāso javoparodhaḥ kṛcchravyavāyatā …”
An obese individual will have a short span of life, slow in initiating activities, and is prone to sexual difficulties.
Not only the relation between the two but also the probable pathophysiology has also been hypothesized. With this as the background, the current study was undertaken to analyze the association of obesity and sexual dysfunction through an observational study.
Source of data
Thirty-three male patients diagnosed as obese, irrespective of religion and occupations were assigned for the study from the outpatient department and inpatient department of Government Ayurveda Medical College and Hospital, Mysore.
Inclusion criteria
Male patients between the age group of 30 and 60 years, diagnosed as having primary obesity and who were willing for the study were selected after obtaining written consent. This is the age group where in sexual difficulties associated with obesity are more prevalent and evident.
Diagnostic criteria
Patients with body mass index (BMI) 30 and above, along with waist-hip ratio >1.0 were considered for the study.[8] BMI was taken as a diagnostic criterion as it takes into account both height and weight of an individual. Waist-hip ratio is also considered, because BMI alone does not account for weight distribution.
Exclusion criteria
Patients with other systemic disorders that interfere with the study and individuals with congenital anomalies of urogenital tract
Obesity secondary to other endocrinal disorders
Patients who have undergone other surgical interventions which interfere with sexual activity/performance
Individuals having infection or anomalies of genital organs.
MATERIALS AND METHODS
Measurement of weight
Patients were asked to remove their footwear and were asked to stand on the weighing machine with minimum clothing devoid of any accessories (handbag, mobile phone). The reading was observed and recorded in kilograms.
Measurement of waist and hip
Measurements were taken in centimeters using a measuring tape at different levels like:
Waist-at the level of umbilicus
Hip-at the level of maximum prominence.
Measurement of height
Heights were measured by asking the patient to stand bare foot with their heel, back, and head touching the wall. In that position, a metal scale was placed over the head perpendicular to the wall and the corresponding reading on the wall was recorded in centimeters.
Assessment tool
A multidimensional scale, International Index of Erectile Function Questionnaire (IIEF) was used to assess sexual function of the individuals. The scale was developed and standardized by Raymond et al.[9] It helps in assessing the overall sexual function of an individual, which includes erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction.
In the beginning of the questionnaire, instructions were given regarding how the questions are to be answered, and the terminologies used in the questionnaire were defined. IIEF questionnaire contains 15 questions and each question has five options.
Method to assess erectile function through the IIEF scale
The questionnaire was translated to the regional language Kannada by the researcher. Each question was carefully translated and care was taken to convey the same meaning as in the original questionnaire. The individuals were informed about the questionnaire and the purpose of administering it to them. Instructions were given to mark whichever appropriately suits them among the five options of answers. It was also suggested to answer all the questions compulsorily. In some undereducated individuals, each question was read and explained and the answer given by the patient was scored against the options given in the answer.
Scoring was done based on the standardized methods of the scale in all the five domains of sexual functioning as described in Tables 1 and 2.
Table 1.
Describing the scoring algorithm for IIEF
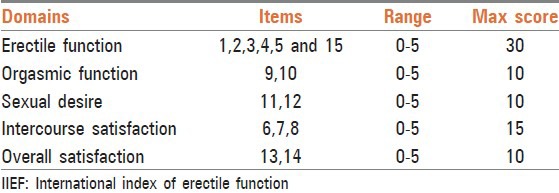
Table 2.
Describing clinical interpretation of the scores of IIEF

Statistical analysis
Statistical analysis to assess individual and comparative effects of the data was done using descriptive statistics, frequencies and percentages, Chi-square test, and Pearson's product moment correlation. All the statistical methods were carried out using the SPSS software suite (version 16.0)
Criteria for assessment
The scoring algorithm for IIEF which was used to assess the five domains of sexual functioning is given in Table 1.
Clinical interpretation
The scores in all the five domains of sexual functioning are interpreted based on the scoring pattern are listed in Table 2.
OBSERVATIONS AND RESULTS
In the present study, all the 33 individuals completely answered the questionnaire that was given for the study and the results were statistically analyzed.
Erectile functions
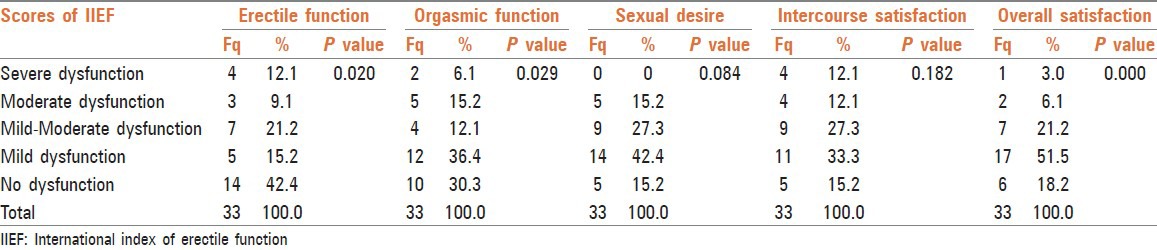
In the present study, out of 33 individuals, 19 (57.6%) obese males had some degree of erectile dysfunction varying from mild to severe which was statistically significant (P <0.02).
Orgasmic function
In the present study, 23 (69.7%) obese males had varying degrees of orgasmic dysfunction which was statistically significant (P < 0.02).
Sexual desire
Out of 33 individuals, 84.8% of individuals had problems with sexual desire which varied from severe to mild degrees though none had severe sexual desire dysfunction which was statistically insignificant (P<0.08).
Intercourse satisfaction
Out of 33 individuals, 84.8% of individuals had problems with intercourse satisfaction though most of the subjects had only mild to moderate degree of impairment (60.6%) hence statistically insignificant (P< 0.18).
Overall satisfaction
Out of 33 individuals, 27 (81.8%) had varying degree of dysfunction in the parameter overall satisfaction which was statistically significant (P < 0.000).
Correlations of BMI and waist-hip ratio with erectile functions
There was significant relation observed between waist-hip ratio and erectile function with significant P value 0.01. There was no significant relation observed between BMI and erectile function.
Scores of IIEF related to erectile functions, orgasmic functions, sexual desire, intercourse satisfaction, and overall satisfaction in individuals of obesity are given in Table 3.
Table 3.
The scores of IIEF related to erectile functions, orgasmic functions, sexual desire, intercourse satisfaction, and overall satisfaction in the individuals of Sthaulya
Correlations of BMI and waist-hip ratio with erectile functions in the individuals of obesity are given in Table 4.
Table 4.
Showing the correlations of BMI and waist-hip ratio with erectile functions in the individuals of Sthaulya

DISCUSSION
Kṛcchra Vyavāya (sexual dysfunction)
The literal meaning of the term “Kṛcchra Vyavāya” is “difficulty in sexual intercourse.” Caraka saṃhita gives a clear statement regarding the relationship that exists between the difficulty experienced during sexual intercourse and the weight of the body.[1]
The different phases of sexual intercourse include Saṅkalpa, Ceṣṭā, Niśpīḍana and Śukracyuti. Sexual dysfunction may be understood/appreciated at different phases of Vyavāya as follows.
“Desire” is the prerequisite for sexual intercourse. This is explained under the heading ‘Saṅkalpa.” Loss of desire toward sexual act is the foremost cause for Kṛcchra Vyavāya.
‘Ceṣṭā” is the second phase in sexual intercourse. Tactile stimulation is the main object of sexual arousal without which proper arousal is not possible though the person has desire for sex.
‘Niśpīḍana” is the third phase in the act of vyavaya. It is nothing but sexual intercourse. Vyavaya depends on the position of male and female partners during the act. Improper position leads to difficulty in sexual intercourse which is also considered as Kṛcchra Vyavāya.
“Śukracyuti” is the fourth phase in the act of vyavāya. Proper Cheṣṭa, Saṅkalpa, and Niṣpīḍana are essential for Śukracyuti. Delayed or premature Śukracyuti is because of improper Ceṣṭā, Saṅkalpa, and Niśpīḍana which is also considered as Kṛcchra Vyavāya.
There are eight specific factors which influence Śukracyuti viz. Harṣa, Tarṣa, Sāratva, Paicchilya, Gaurava, Anu bhāva, Pravana bhāva, and Drutatva of Maruta. Among them, the former two factors viz Harṣa and Tarṣa represent the psychological factors which are responsible for Saṅkalpa.
Harṣa
Saṅkalpa results in Harṣa. By Harṣa, dhvajocchraya (erection) occurs. Improper or absence of proper erection is a chief cause for Kṛcchra Vyavāya.
Tarṣa
It is nothing but vāanitābhilāṣā (desire to have a female partner). Lack of this desire is one of the cause for Kṛcchra Vyavāya.
The latter six factors namely Sāratva, Paicchilya, Gaurava, Anu bhāva, Pravana bhāva, depend on the quality of the Śukra formed. If the Śukra produced does not possess all the requisite qualities (śuddha Śukra lakṣaṇas), then it lacks in above-mentioned factors which invariably becomes a cause for sexual dysfunction. Apart from these, sexual dysfunction in obesity may also result from medasāvṛtamārga (obstruction to the channels of Śukra by medas alone or medas and kapha together). In obesity, there will be impaired lipid metabolism (medodhātvagnimāndya) resulting in excessive production of medas which is abaddha (free) in nature. This abaddha medas obstructs different channels of the body including the channels of Śukra. The obstruction to the channels may also aggravate vāta particularly the apānavāta (which regulates reproductive and excretory functions) being situated in śhroni (pelvis) and meḍhra (reproductive organ). Śukraniṣkramaṇakriyā (ejaculation of Śukra) is one of the normal functions of apāna vāta which is disturbed because of obstruction (avarana) resulting in sexual dysfunction. Thus, normalcy of apana vata is necessary for Śukracyuti. Any abnormality in its function can result in Kṛcchra Vyavāya.
The normal functions of Śukra include dhairya, cyavana, prīti, harṣa, deha bala, and garbhotpādana.[10] Among them, dhairya, prīti, and harṣa represent the psychological factors. “Dhairya” is a factor which is essential for cyavana and maithuna. “Prīti” is affection toward opposite sex and “harṣa” is the stage of excitement. These factors all together help in Śukracyuti.
Difficulties experienced at different stages of Vyāvaya in obesity
Saṅkalpa
It is the stage of mental preparation for sexual act. The cardinal features of Sthaulya such as cala sphik, udara, stana, ayathopacaya (disproportionate growth of body), ayathotsāha (lack of enthusiasm), daurbalya (weakness), sveda bādhā-daurgandhya (excess sweating and bad odor), ati kṣut (excess hunger), and ati pipāsā (excess thirst) will hamper the routine of the individual resulting in depression, stress, anxiety, and other psychological disturbances. These disturbances may cause apprehension about the sexual act and subsequently decrease the sexual libido which is evident in the present study as 84.8% of individuals had problems with sexual desire which varied from severe to mild degrees.
Cheṣṭā
Ceṣṭhā composes of activities which happen during Vyavāya (sexual intercourse). In obesity, there will be javoparodha (sluggish movements) and daurbalya (weakness) because of this, an obese individual finds difficulty in performing activities during the sexual act. Hence, a positive correlation is found between waist-hip ratio and erectile dysfunction in the present study. Measures of slimness (smaller waist and/or hips) are associated with greater frequency of penile-vaginal intercourse by both men and women and lesser masturbation frequency,[11] which suggests the fact that the erectile functions are dependent on the waist-hip ratio.
Erectile disorders manifest during this phase. In the present study, 57.6% of individuals had some degree of erectile dysfunction. The reason attributed for ED in obese individuals is defective nitric oxide activity. Satisfactory erection and orgasm are linked to nitric oxide availability. There will be impairment in neurogenic and endothelium-dependent relaxation which is demonstrated in isolated corpus cavernosum strips from patients with ED,[12] suggesting the presence of a possible vascular pathway underlying both obesity and ED. Even the recent studies suggest that one-third of obese men with ED regain their sexual activity after reducing weight.[7] In obesity, ED may occur both due to psychological and physical factors.
Erection (dhvajocchrāya) is a process, which occurs mainly due to harṣa. Harṣa is a psychological factor, which is impaired in obese individuals. Because of this, ED can occur. Also in obesity, there will be medasāvṛta mārga because of which dilatation of Śukra vāha srotas is not proper. This āvarana by medas results in ED as vasodilatation is invariably needed for erection, which is considered as the physical factor, which is evident in the erectile and orgasmic function reduction in the present study.
Śukracyuti and Niṣpīḍana
A total of 84.8% of individuals in the study had problems with intercourse satisfaction and 81.8% had varying degree of dysfunction in overall satisfaction. These results are due to impairment in the stages “Nishpeedana” and “Shukra cyuti” during intercourse. The difficulties experienced by obese individuals during the stage of Niṣpīḍana and Śukra cyuti may be in the form of premature ejaculation, delayed ejaculation, and painful orgasm. All these difficulties are again the impact of either decreased volume or obstruction to the passage. The position of male and female is one of the important key factors for sexual pleasure. In obese individuals, sexual pleasure may be reduced because of their inability to perform in different postures. The restricted movement of the body acts as a blocking factor for a comfortable sexual act. Premature ejaculation and delayed ejaculation are also the difficulties faced during orgasmic phase, as a result of apāna vāta impairment caused by obstruction/blockage (mārgāvarodha). This concept is supported by a strong epidemiological evidence which links the subsequent risk of ED to the presence of well-recognized risk factors for Coronary Heart Disease (CHD), such as smoking, diabetes, hypertension, and dyslipidemia.[13–15] Erectile dysfunction, which is associated with abnormal endothelial function, has four out of the five components of metabolic syndrome as risk factors.[16]
Reduced quantity of Śukra and obstruction to the channels of Śukra by medas leading to impaired apāna vāta functioning could be the possible cause for sexual dysfunction in patients of obesity and that future studies should be done in this direction in order to get objective findings to support the hypothesis. Pain and other discomforts experienced during intercourse in obese individuals may be because of the decreased volume or impaired apāna vāta. Most of the times, it may be a combination of both.
From the above analysis, it can be inferred that the people who are obese are more prone to have sexual difficulties during the different phases of Vyavāya.
Limitations of the study
Though the IIEF questionnaire was carefully translated after consulting language and subject experts, it was not back translated.
CONCLUSION
The present study was aimed at understanding the relationship between obesity and sexual dysfunction with respect to the different stages of normal sexual response cycle. For assessment, parameters like IIEF were used and results were analyzed.
Sexual dysfunction in obesity can be considered as the difficulty encountered in various stages of Vyavāya and there is a definite relationship between obesity and sexual dysfunction. The difficulty in sexual act experienced in obesity may be due to a combination of psychological and physical causes.
Erectile functions, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction are impaired in obesity. Correlation studies suggested that there was no relation between BMI and erectile functions. However, the studies suggested that erectile dysfunction increases proportionately with increase in waist-hip ratio. The rest of the components in IIEF had no relationship with waist-hip ratio. In obesity, there will be varying degrees of sexual dysfunction which is evident from the present observational study.
Sexual dysfunction was assessed functionally in the present study. Ayurveda points out that there could be a structural and quantifiable basis for the same. Further studies are needed to explore the hypothetical assumptions derived from ayurvedic texts pointing to quantitative and qualitative degradation of Śukra as well as blockage of the channels of Śukra by medas as the basis for erectile dysfunction and impotency in obese individuals.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Charaka . Varanasi: Choukhambha Prakashana; 2007. Charaka Samhita Sootra Sthana 21/4; p. 116. [Google Scholar]
- 2.Charaka . Varanasi: Choukhambha Prakashana; 2007. Charaka Samhita Sootra Sthana 21/9; p. 117. [Google Scholar]
- 3.Haslam DW, James WP. Obesity. Lancet. 2005;366:1197–209. doi: 10.1016/S0140-6736(05)67483-1. [DOI] [PubMed] [Google Scholar]
- 4.Corona G, Mannucci E, Fisher AD, Lotti F, Petrone L, Balercia G, et al. Low levels of androgens in men with erectile dysfunction and obesity. J Sex Med. 2008;5:2454–63. doi: 10.1111/j.1743-6109.2008.00856.x. [DOI] [PubMed] [Google Scholar]
- 5.Braun M, Wassmer G, Klotz T, Reifenrath B, Mathers M, Engelmann U. Epidemiology of erectile dysfunction: Results of the Cologne Male Survey. Int J Impot Res. 2000;12:305–11. doi: 10.1038/sj.ijir.3900622. [DOI] [PubMed] [Google Scholar]
- 6.Walczak MK, Lokhandwala N, Hodge MB, Guay AT. Prevalence of cardiovascular risk factors in erectile dysfunction. J Gend Specif Med. 2002;5:19–24. [PubMed] [Google Scholar]
- 7.Esposito K, Giugliano D. Obesity, the metabolic syndrome, and sexual dysfunction. Int J Impot Res. 2005;17:391–8. doi: 10.1038/sj.ijir.3901333. [DOI] [PubMed] [Google Scholar]
- 8.Lawrence M, Tierney DM, McPhee SJ, Papadakis MA. International edition. 42nd ed. New York: Lange Medical Books McGraw-Hill/Medical Publishing Division; 2003. Current Medical Diagnosis and Treatment; pp. 1224–5. [Google Scholar]
- 9.Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49:822–30. doi: 10.1016/s0090-4295(97)00238-0. [DOI] [PubMed] [Google Scholar]
- 10.Sushruta . Varanasi: Choukhambha Orientalia; 2003. ’Sushruta Samhita Sootra Sthana 15/37; p. 73. [Google Scholar]
- 11.Brody S. Slimness is associated with greater intercourse and lesser masturbation frequency. J Sex Marital Ther. 2004;30:251–61. doi: 10.1080/00926230490422368. [DOI] [PubMed] [Google Scholar]
- 12.de Tejada Saenz I, Goldstein I, Azadzoi K, Krane RJ, Cohen RA. Impaired neurogenic and endothelium-mediated relaxation of penile smooth muscle from diabetic men with impotence. N Engl J Med. 1989;320:1025–30. doi: 10.1056/NEJM198904203201601. [DOI] [PubMed] [Google Scholar]
- 13.Feldman HA, Johannes CB, Derby CA, Kleinman KP, Mohr BA, Araujo AB, et al. Erectile dysfunction and coronary risk factors: Prospective results from the Massachusetts male aging study. Prev Med. 2000;30:328–38. doi: 10.1006/pmed.2000.0643. [DOI] [PubMed] [Google Scholar]
- 14.Fung MM, Bettencourt R, Barrett-Connor H. Heart disease risk factors predict erectile dysfunction 25 years later: Yhe Rancho Bernardo Study. J Am Coll Cardiol. 2004;43:1405–11. doi: 10.1016/j.jacc.2003.11.041. [DOI] [PubMed] [Google Scholar]
- 15.Feldman HA. Erectile dysfunction, cardiovascular disease and cardiovascular risk factors: Prospective results in a large random sample of Massachusetts men. J Urol. 1998;159:91. [Google Scholar]
- 16.Celermajer DS, Sorensen KE, Bull C, Robinson J, Deanfield JE. Endothelium-dependent dilation in the systemic arteries of asymptomatic subjects relates to coronary risk factors and their interaction. J Am Coll Cardiol. 1994;24:1468–74. doi: 10.1016/0735-1097(94)90141-4. [DOI] [PubMed] [Google Scholar]