

Abstract
The prevalence of drug addiction is increasing globally. Drug abuse damages many parts of the body such as oral cavity, lungs, liver, brain, heart etc., Addicts suffer from physical, psychological, emotional and behavioral problems. Their nutrition is also compromised. There is certainly an impact of all these factors on the health of periodontium. Dentists should be aware of the effects of drugs while treating the drug addicts. This article correlates the studies done on the impact of abused drugs such as alcohol, tobacco, opiates, cannabis, amphetamines etc., on general and periodontal health.
Keywords: Drug addicts, periodontal diseases, substance abuse
INTRODUCTION
Use of substances such as alcohol, tobacco and other illicit drugs is a health-care problem of growing concern. Illicit substance abuse is on a rising trend globally. It is more common in males than in females. World Health Organization estimated that 2 billion people across the world consume alcohol and 76.3 million have some alcohol induced complications.[1] Substance Abuse and Mental Health Services Administration year 2000 survey reported that heavy alcohol drinking, tobacco and illicit drug use is increasing and causing serious health problems.[2,3] Addicts are physically and psychologically dependent on drugs and neglect their oral hygiene, nutrition and systemic health, which are directly related to dental and periodontal diseases. These drugs can have local and systemic harmful effects.
DRUG ABUSE AND DRUG DEPENDENCE
Drug abuse
When drugs are used in a manner or amount inconsistent with the medical or social pattern or culture it is called drug abuse.
Drug dependence
Most controlled substances are capable of producing dependence either physical, psychological or both after repeated use of the drug that necessitates continued administration of the drug to prevent withdrawal symptoms.
Drug addiction
It is defined as physical and psychological dependence on psychotic substances (e.g., Alcohol, tobacco, heroine and other drugs), which cross the blood brain barrier once ingested, temporarily altering the chemical milieu of the brain.[2]
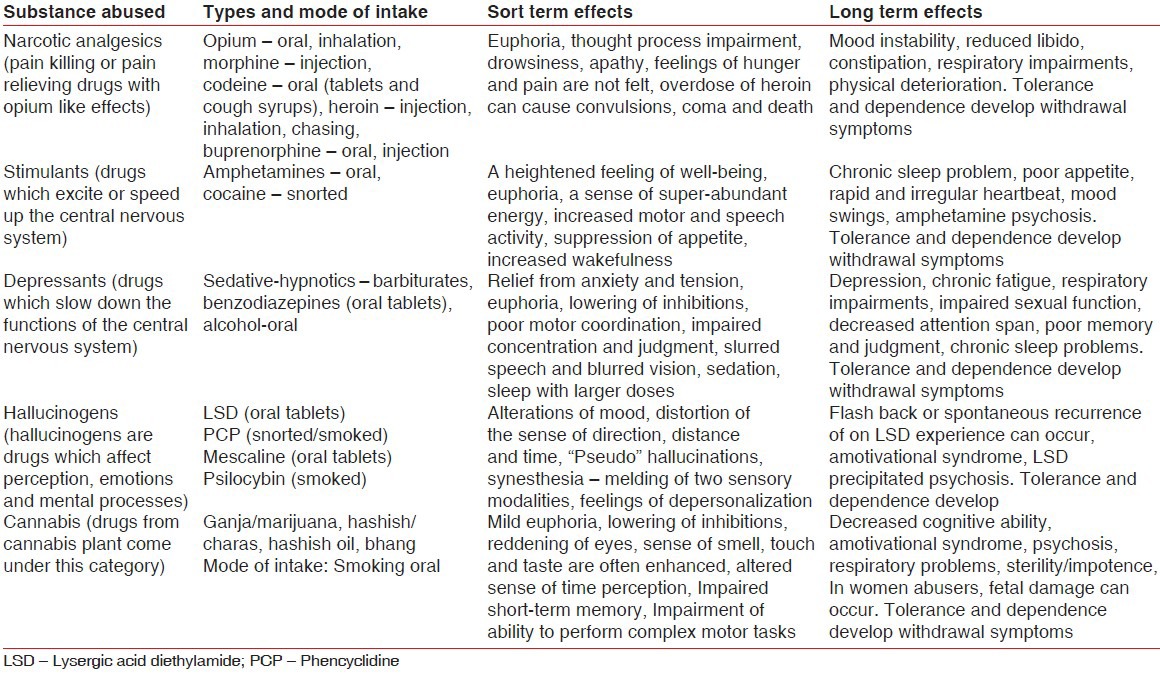
The illicit drugs have high addiction potential. The user becomes dependent on these drugs both physically and psychologically. Users become dependent or get addicted to drugs he needs it at regular intervals and gradually the quantity of the drug also increases. If an addict does not get his/her dose of drug, he/she starts having withdrawal symptoms and that forces him/her to take the next dose of the drug. An addict may use one drug or a combination of many drugs. Commonly abused drugs are summarized in Table 1.
Table 1.
Commonly abused drugs
ORAL MANIFESTATIONS OF SUBSTANCE ABUSE
Many of the abused substances have devastating consequences on oral health. Cocaine can result in movement disorder and manifest itself as transient chorea. In addition, buccolingual dyskinesia, which is commonly known as “crack dancing” or boca torcida (twisted mouth), can also be present. In the case of heroin abuse, increased numbers of decayed, missing and filled teeth can be detected in the mouth. This can result from chronic malnutrition, poor oral hygiene due to impaired motor function and neuropathology secondary to infection, vasculitis, septic emboli, thromboembolism, prolonged heroin-induced respiratory depression, hypotension, positional vascular compression, acute Parkinsonism and spongiform leukoencephalopathy. Marijuana abuse can lead to acidic erosion of enamel due to cannabinoid hyperemesis, in which frequent episodes of vomiting occurs. In addition, these patients develop dental caries, inflammation and hyperplasia of gingival, uvulitis, leukoplakia, oral papillomas and tongue carcinoma. In chronic abuse of methamphetamine which leads to “Meth mouth,” which is characterized by large carious lesions in buccal smooth surface areas and fractured teeth due to increased motor activity. It is important to note that a significant level of osteoporosis has also been reported in a high percentage of methamphetamine abusers. Therefore, it is possible that such structural weakness can occur in the dentition as well.
EFFECTS OF DRUGS ON PERIODONTIUM
Periodontal disease is characterized by inflammation of tooth supporting tissues. Main etiological agent is dental plaque. Whenever there is an imbalance between potentially pathogenic microorganisms and efficacy of host response, the disease results. Dental caries and periodontal diseases are more prevalent in addicts than in the general population.[3,4] Addicts have more cervical plaque on one or more teeth. It has been reported that gingival bleeding is frequently present in addicts. Only 36% of the addicts visited the dentist in 1 year and 18% brush their teeth less than once a day as seen in Dutch community.[5] High incidence of periodontal diseases were observed with heavy calculus deposits and diagnosed as adult periodontitis, which is characterized by loss of attachment. Majority of addicts have a high rate of plaque accumulation and calculus deposits resulting from oral hygiene neglect, xerostomia and alteration in microbial profile.[6]
Periodontal diseases in alcoholics are primarily associated with poor oral hygiene and lack dental care.[7] Alcohol has effects on the oral cavity causing oropharynx cancer, caries, missing/loss of teeth and greater risk of developing periodontal problems including gingival infection, increased pocket depth and loss of attachment have been identified in alcoholics[8,9,10] due to decreased resistance to infection by Gram-negative organisms during the acute alcohol intoxication.[11] Positive correlation has been shown between gamma glutamyl transpeptidase, a liver enzyme, which is an indicator of alcohol drinking and loss of periodontal attachment. This study showed that attachment loss in alcoholics occurs by greater increase in loss of the gingival margin level than non-alcoholics, whereas in cocaine users no attachment loss has been found.[12]
Abused drugs such as opiates lead to suppression of pain responses causing patient to ignore the signs of tooth decay, periodontal diseases and limited access to dental care.[13] Opiates, amphetamines and alcohol are xerostomic, meaning that they reduce the saliva production that protects against dental decay and periodontal diseases. Most injectable drug users (IDU), smoke tobacco causes periodontal problems, oral cancer and pre-cancerous conditions.[14] IDU should always be tested for human immunodeficiency virus and hepatitis as they repeatedly use unsterile needles, which increase the risk for these diseases. The caries prevalence, periodontal health and oral hygiene status was assessed in 124 drug addicts, 96% of them were using heroine.[15] In this study, the mean periodontal index were 1.37 and simplified oral hygiene index Scores were 1.71.
Regular use of cocaine may have severe orofacial effects, such as perforation of the nasal septum, palate, gingival lesion and erosion of the tooth surface. Use of cocaine increases the risk of a medical emergency during dental treatment especially when adrenaline containing local anesthetic or retraction cord is used. This may increase the risk of cardiovascular complications during the dental treatment.[16]
Dental treatment should be postponed for 6-24 h after use of drugs like cocaine. Cocaine users are more prone to oral infections due to the immunosuppressive effects.[15] Oral effects caused by ecstasy include mucosal changes, xerostomia and increased risk of developing dental erosions and bruxism.[3] After abusing drugs like ecstasy subjects experienced dryness in their mouth.[17]
Long-term addiction of heroin contributes directly to lower the oral hygiene status through direct physiologic effects or through poor personal hygiene and chronic malnutrition.[18] High levels of decay, periodontal disease and orofacial/dental trauma have been described in heroin and in-treatment methadone users.[9] Drug abusers also noticed the habit to grind or clench teeth together and felt pain or tenderness in the jaw muscles or joints.[17]
Cannabis users have poor oral health than non-users. There is increased incidence of dental caries and periodontal diseases. Cannabis smoke acts as a carcinogen and can cause premalignant lesions in the oral mucosa.[4] Cannabis associated oral side effects are xerostomia, leukodema and increased prevalence and density of Candida albicans.[19]
Qat leaves are kept into mucobuccal fold and chewing it for several hours with the release of psychoactive agents similar to amphetamine inducing release of dopamine. It is often accompanied by smoking tobacco. Oral diseases associated with qat chewing include periodontitis, oral leukoplakia and oral cancer.[20]
Tobacco use is a known risk factor for the development of oral and periodontal diseases. Its use is associated with increased pocket depth, loss of periodontal attachment, alveolar bone and higher rate of tooth loss. Tobacco also affects the outcome of non-surgical, surgical therapy and also implant placement. Tobacco has nicotine as main ingredient that affects gingival blood flow, cytokine production, neutrophil and other immune cell function and lead to destruction of periodontal tissues.[5,18]
Another factor associated with the development of periodontitis in addicts is the nutritional impairment. It has been found that 21% of alcoholics were malnourished.[21] The addicts do not take proper nutrition, which leads to gingival and periodontal diseases caused by nutritional impairment (reduced body mass index and mid-arm muscle circumference).[22] More so addicts have erratic and irregular eating pattern, which is also associated with dental diseases.
A study concluded that there is a large gap in dental health status and behavior between drug addicts and the general population. Long-term drug addiction either contribute directly to lower the oral health status or the altered life-style of the addicts leads to increase in oral diseases.[23] Addicts neglect their oral hygiene because of physical and emotional dependence on drugs. Local environmental factors combined with systemic effects of drug, rather than drug itself seem to be responsible for high incidence of dental diseases.[24]
ORAL MANAGEMENT IMPLICATION IN SUBSTANCE ABUSE
The identification of dental patients with substance abuse is an important task in the modern practice dentistry. Negative outcomes related to oral care is essential, but also assisting the client in seeking treatment to become sober is important. Following considerations are important in patients with substance abused.
HABIT CESSATION PROGRAMS
A study describing the patterns of tobacco use counseling among physicians and dentists (as reported by these adolescents) determined the association between provider advice to quit and cessation activities among current smokers.[25] The findings were 33% of adolescents, who visited a physician or a dentist in the past year reported that a physician counseled them about the dangers of tobacco use and 20% reported that a dentist provided a similar message. Among students who smoked in the past year, 16.4% received advice to quit from a physician and 11.6% received advice to quit from a dentist. Physician or Dentist advice to quit was correlated with one or more quit attempts in the past 12 months. Researchers concluded that physician and dentist practice patterns on smoking cessation are well below recommended guidelines and that failure to suggest smoking cessation may represent a missed opportunity to affect adolescent smoking behavior.
APPOINTMENT CONSIDERATIONS
Regular visits for oral health services are difficult due to the life-style of the addict. Substance abusers have frequent missed appointments and failure to pay for services may occur. Behavior management problems are possible. Medical complications may cause treatment to be delayed in order to complete medical consultations. Vital signs must be measured at every appointment to assess systemic health. Needle tracks may be evident when the blood pressure cuff is placed. Pain tolerance may be decreased, resulting in failure of local analgesic agents to relieve pain. Oral health-care providers should require anyone suspected of drug abuse to sign a statement indicating drugs have not been used within the previous 24 h.[26,27] When alcohol abuse is suspected in the dental patient, management depends on if the patient is intoxicated or simply shows signs of alcohol abuse (red face, bloodshot eyes, hypertrophy of parotid glands, breath odors of alcohol) or reports substance abuse on the health history. A patient who comes to the appointment in an inebriated state should be rescheduled. The client should be escorted and accompanied to their home by a responsible person. This can include a family member, friend or caregiver.
ORAL HYGIENE IMPLICATIONS
The dental hygienist must use the medical history information as well as extra-oral observation and clinical examination to identify the patient with substance abuse problems. Periodontitis in adolescents may suggest a need to question the client about marijuana use. Breath odors may be indicative. Enlarged parotid glands should be investigated for etiological factors. The practitioner should be aware of the possibility for increased blood pressure and monitor vital signs during each appointment. Awareness of the potential for excessive bleeding when poor liver function is likely and monitoring bleeding during periodontal procedures is necessary. If excessive bleeding is observed, treatment should be stopped and digital pressure applied. Referral for medical evaluation and necessary blood coagulation tests should be advised before further treatment procedures. Since alcohol and tobacco use increases the risk for oral cancer, an oral cancer examination should be completed at each maintenance visit. Reduced salivary flow may cause increased caries or candidiasis. Anticaries agents should be recommended if needed and antifungal therapy should be prescribed by the dentist, if indicated. Because opioid abusers develop tolerance to the analgesic effects of opioids managing dental pain can be difficult. Non-steroidal analgesics (ibuprofen, naproxen) may be used. If the patient is in recovery, giving an opioid-containing analgesic can cause the recovery to fail and stimulate the person to begin abusing opiates again. For the alcoholic patient, acidic drugs, such as aspirin and non-steroidal anti-inflammatory drugs should be avoided due to the risk of inducing bleeding in the stomach. Acetaminophen can be used up to 4 g daily. There is an absolute drug interaction between vasoconstrictors and cocaine that prohibits using the two drugs together. Vasoconstrictors should also be avoided when methamphetamine has been used within the past 24 h. This must be explained to the patient and the patient must provide assurance that drugs will not be used within 24 h prior to an oral hygiene appointment where local anesthesia with a vasoconstrictor is indicated. The vasoconstrictor is needed to reduce the periodontal bleeding as the use of a local anesthetic alone may not provide the duration of anesthesia or the degree of hemostasis necessary for the procedure. When central nervous system depressant drugs (e.g., cocaine, heroin, narcotics in general) are taken there can be dangerous drug interactions with local anesthetics containing vasoconstrictors. Cocaine and vasoconstrictors have a strong interaction that can lead to cardiac arrest. Non-alcohol mouth rinse products should be recommended when substance abuse is suspected or in those with a history of alcohol abuse. Dental implications for the alcohol abuser includes the need for a thorough oral examination due to the increased risk for oral cancer, monitoring of oral self-care (neglect of oral care is common) and questioning about a history of liver disease and subsequent bleeding problems. The diseased liver is unable to store adequate levels of vitamin K and the conversion of vitamin K to coagulation factors is reduced. This reduces the vitamin K-dependent coagulation factor (II, VII, IX and X) levels and increased bleeding. Other comorbid conditions include thrombocytopenia, esophageal varices, spontaneous bleeding and abdominal distension associated with liver failure. The drugs used in dentistry that are metabolized in the liver are amide local anesthetics and benzodiazepines. These drugs may have reduced metabolism and blood levels will not fall as rapidly as in the normal patient. Single dose of the drug do not require reduction, but repeated doses may be required to be reduced, or the interval between doses to be prolonged, to prevent excessive blood levels. Practitioners can advise counseling for drug addiction when the abusing client admits.
SPECIAL CARE IN PREGNANT WOMEN WITH SUBSTANCE ABUSE
The fact that pregnant women and health-care providers who are also substance abusers can seek dental care is often overlooked. Substance used by pregnant women is a leading preventable cause of mental, physical and psychological problems in infants and children. Regardless of the drug(s) ingested or the clinical symptoms, it is very hard to predict the anesthetic implications in the drug abusers. It is also true for both regional and general anesthesia administered to the parturient. Alcohol and other substances taken by pregnant women can harm the mother and the unborn baby. Occasionally, emergency situations may arise where the dentists will have to perform major surgical procedures on the expecting mothers who also have a known or concealed substance abuse history. Accidents and other trauma cases may require emergency maxillofacial surgical procedures on a pregnant patient who can also be an active substance abuser. In those cases, administering regional or even general anesthesia may become imperative. Unfortunately, the administration of local, regional or general anesthesia can have major health consequences.
CONCLUSION
Drug abuse is a matter of growing concern these days as it is increasing day by day. There are various types of drugs which are abused such as alcohol, opiates, cocaine, cannabis, tobacco, qat, amphetamines etc., Patients who abuse these drugs are physically, mentally and emotionally dependent upon these drugs and cannot leave them on their own. These drugs have deleterious effect on patients overall health in general and oral health in particular. Patients who are addicted to drugs suffer from poor oral hygiene, xerostomia, increased prevalence of dental and periodontal diseases. This review can be of helpful to the dental professionals to understand the effects of substances abused on the periodontal tissues in addicts. Dentists attending to these patients should follow the proper protocol while handling such patients.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.World Health Organization. Global Status Report on Alcohol-2004. Department of Mental Health and Substance Abuse. [Last accessed on 2013 Apr 25]. Available from: http://www.who.int/substanceabuse/publications/globalstatus_report_2004_overview.pdf .
- 2.Substance Abuse and Mental Health Services Administration-2000. National Household Survey on Drug Abuse-2000. [Last accessed on 2013 Apr 26]. Available from: http://www.SAMHSA.gov .
- 3.Brand HS, Dun SN, Nieuw Amerongen AV. Ecstasy (MDMA) and oral health. Br Dent J. 2008;204:77–81. doi: 10.1038/bdj.2008.4. [DOI] [PubMed] [Google Scholar]
- 4.Cho CM, Hirsch R, Johnstone S. General and oral health implications of cannabis use. Aust Dent J. 2005;50:70–4. doi: 10.1111/j.1834-7819.2005.tb00343.x. [DOI] [PubMed] [Google Scholar]
- 5.Malhotra R, Kapoor A, Grover V, Kaushal S. Nicotine and periodontal tissues. J Indian Soc Periodontol. 2010;14:72–9. doi: 10.4103/0972-124X.65442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Molendijk B, Ter Horst G, Kasbergen M, Truin GJ, Mulder J. Dental health in Dutch drug addicts. Community Dent Oral Epidemiol. 1996;24:117–9. doi: 10.1111/j.1600-0528.1996.tb00826.x. [DOI] [PubMed] [Google Scholar]
- 7.Fazzi M, Vescovi P, Savi A, Manfredi M, Peracchia M. The effects of drugs on the oral cavity. Minerva Stomatol. 1999;48:485–92. [PubMed] [Google Scholar]
- 8.Tezal M, Grossi SG, Ho AW, Genco RJ. The effect of alcohol consumption on periodontal disease. J Periodontol. 2001;72:183–9. doi: 10.1902/jop.2001.72.2.183. [DOI] [PubMed] [Google Scholar]
- 9.Shizukuishi S, Hayashi N, Tamagawa H, Hanioka T, Maruyama S, Takeshita T, et al. Lifestyle and periodontal health status of Japanese factory workers. Ann Periodontol. 1998;3:303–11. doi: 10.1902/annals.1998.3.1.303. [DOI] [PubMed] [Google Scholar]
- 10.Amaral Cda S, Luiz RR, Leão AT. The relationship between alcohol dependence and periodontal disease. J Periodontol. 2008;79:993–8. doi: 10.1902/jop.2008.070525. [DOI] [PubMed] [Google Scholar]
- 11.Marr JJ, Spilberg I. A mechanism for decreased resistance to infection by gram-negative organisms during acute alcoholic intoxication. J Lab Clin Med. 1975;86:253–8. [PubMed] [Google Scholar]
- 12.Khocht A, Janal M, Schleifer S, Keller S. The influence of gingival margin recession on loss of clinical attachment in alcohol-dependent patients without medical disorders. J Periodontol. 2003;74:485–93. doi: 10.1902/jop.2003.74.4.485. [DOI] [PubMed] [Google Scholar]
- 13.Carter EF. Dental implications of narcotic addiction. Aust Dent J. 1978;23:308–10. doi: 10.1111/j.1834-7819.1978.tb03528.x. [DOI] [PubMed] [Google Scholar]
- 14.Laslett AM, Dietze P, Dwyer R. The oral health of street-recruited injecting drug users: Prevalence and correlates of problems. Addiction. 2008;103:1821–5. doi: 10.1111/j.1360-0443.2008.02339.x. [DOI] [PubMed] [Google Scholar]
- 15.Angelillo IF, Grasso GM, Sagliocco G, Villari P, D’Errico MM. Dental health in a group of drug addicts in Italy. Community Dent Oral Epidemiol. 1991;19:36–7. doi: 10.1111/j.1600-0528.1991.tb00102.x. [DOI] [PubMed] [Google Scholar]
- 16.Brand HS, Gonggrijp S, Blankma CJ. Cocaine and oral health. Br Dent J. 2008;204:365–9. doi: 10.1038/sj.bdj.2008.244. [DOI] [PubMed] [Google Scholar]
- 17.Murray MO, Wilson NH. Ecstasy related tooth wear. Br Dent J. 1998;185:264. doi: 10.1038/sj.bdj.4809785. [DOI] [PubMed] [Google Scholar]
- 18.Novak MJ, Novak KF. Smoking and periodontal disease. In: Newman MG, Takei H, Carranza FA, editors. Carranza's-Clinical Periodontology. 9th ed. St. Louis: WB Saunders Companay; 2003. p. 245. [Google Scholar]
- 19.Versteeg PA, Slot DE, van der Velden U, van der Weijden GA. Effect of cannabis usage on the oral environment: A review. Int J Dent Hyg. 2008;6:315–20. doi: 10.1111/j.1601-5037.2008.00301.x. [DOI] [PubMed] [Google Scholar]
- 20.El-Wajeh YA, Thornhill MH. Qat and its health effects. Br Dent J. 2009;206:17–21. doi: 10.1038/sj.bdj.2008.1122. [DOI] [PubMed] [Google Scholar]
- 21.Harris CK, Warnakulasuriya KA, Johnson NW, Gelbier S, Peters TJ. Oral health in alcohol misusers. Community Dent Health. 1996;13:199–203. [PubMed] [Google Scholar]
- 22.Harris C, Warnakulasuriya KA, Gelbier S, Johnson NW, Peters TJ. Oral and dental health in alcohol misusing patients. Alcohol Clin Exp Res. 1997;21:1707–9. [PubMed] [Google Scholar]
- 23.Rosenstein DI. Effect of long-term addiction to heroin on oral tissues. J Public Health Dent. 1975;35:118–22. doi: 10.1111/j.1752-7325.1975.tb04035.x. [DOI] [PubMed] [Google Scholar]
- 24.Colon PG., Jr Dental disease in the narcotic addict. Oral Surg Oral Med Oral Pathol. 1972;33:905–10. doi: 10.1016/0030-4220(72)90181-8. [DOI] [PubMed] [Google Scholar]
- 25.Shelley D, Cantrell J, Faulkner D, Haviland L, Healton C, Messeri P. Physician and dentist tobacco use counseling and adolescent smoking behavior: Results from the 2000 national youth tobacco survey. Pediatrics. 2005;115:719–25. doi: 10.1542/peds.2004-0873. [DOI] [PubMed] [Google Scholar]
- 26.Scofield JC. The gravity of methamphetamine addiction. Dimens Dent Hyg. 2007;5:16–8. [Google Scholar]
- 27.Pitiphat W, Merchant AT, Rimm EB, Joshipura KJ. Alcohol consumption increases periodontitis risk. J Dent Res. 2003;82:509–13. doi: 10.1177/154405910308200704. [DOI] [PubMed] [Google Scholar]