

Abstract
Background:
Changes in pulse rate and blood pressure are common consequences during oral surgeries. Hypoxia during surgical process is another side effect. The objective of the present study was evaluation of blood hemoglobin oxygenation and hemodynamic changes during periodontal surgery.
Materials and Methods:
This clinical trial study was conducted upon 50 subjects aged 30-55 years who referred to the clinic of dental faculty of Babol University and needed periodontal surgery with modified widman flaps in the anterior section of the maxilla. Pulse rate, blood pressure, and pulse oximetric evaluations were recorded in five stages during surgery.
Results:
The average of systolic and diastolic blood pressure had been in their maximum amount in the second stage of evaluation and minimum amounts were in the first one; while pulse rate changes were greatest in the second stage and lowest in the fifth stage. Analyzing the data revealed no significant difference in Blood Oxygen Saturation (SpO2) measurements in none of the stages evaluated.
Conclusions:
Blood pressure and heart rate increased significantly after the injection of anesthetic drug and in further phases they were decreased after the elimination of stimulating effect of adrenaline. SpO2 changes were not significantly prominent.
Keywords: Hemodynamic changes, pulse oximetry, periodontal surgery, SpO2
INTRODUCTION
Successful management and treatment of periodontal disease depends upon simple medical procedures such as health education, prophylaxis, scaling and root-planing, gingivectomy, gingival grafts, and different types of gingival flaps.[1]
Periodontal pocket refers to the pathological increase in the depth of gingival sulcus, and is one of the main clinical features of periodontal disease. Elimination of pathological changes of the pocket wall is among the objectives of surgical treatment for periodontal pockets, so that a stable and sustainable situation can be achieved. Currently, several flap techniques have been applied for the treatment of pocket, among which modified Widman flap is worth mentioning. This technique facilitates the use of equipment, in which pocket lining is removed with no effect on reducing the pocket depth.
Dental treatments are accompanied by patients’ hemodynamic changes; for instance, increase in blood pressure and heart rate during dental treatment are influenced by various factors such as physical and physiological stress, painful stimuli, and activity of catecholamines present in local anesthetic solutions.[2] Heart rate, which is indicative of ventricular contraction, changes in different conditions, including pain, anxiety, stress, heart diseases, metabolic and endocrine disorders and heart muscle diseases, and is evaluated by peripheral pulse measurement or the electrocardiogram and pulse oximetry. For the measurement of blood pressure, different methods are applied, from which Riva-Rocci, Korotokoff, Dinamap, and Finometer techniques can be enumerated. Due to the risk of hypoxia in oral surgeries, pulse oximetry is also recommended to be used in these cases.[3] Pulse oximeter is a reliable and sensitive apparatus in detecting small amounts of blood oxygen saturation, and in all patients, SpO2 (SpO2) normal percentage is not less than 95%.[4]
A dental patient is exposed to stressors, such as physiological responses to emotional factors and/or pain. Pain and anxiety, are important stimuli for the secretion of endogenous adrenaline, which plays a significant role in cardiovascular responses during dental treatment.[5]
Local anesthetics mainly affect a limited area; however, they will be absorbed from the injection site and exert general effects, especially on cardiovascular or central nervous system. General effects are pronounced particularly in cases with high dose administrations.[6]
Lidocaine along with epinephrine is the most common anesthetic used in oral surgeries. It is obvious that more the concentration of epinephrine, the better the control of bleeding, but there will be more cardiovascular changes. In spite of the effect of local anesthetics on vital signs, their accurate application is able to dramatically reduce stress.[7]
Given the above bodies of evidence and the importance of monitoring patients’ hemodynamic changes during oral surgery, the present study has been conducted to investigate these alterations during periodontal surgery outside the operating room with local anesthesia.
MATERIALS AND METHODS
This practical clinical trial study was carried out on patients with gingival disease referred to the clinic of Dental Faculty of Babol University of Medical Sciences, and underwent modified Widman flap surgery on anterior maxillary region in Periodontology Department. The equipments used in the study included (1) Finger pulse oximeter (Soor Afarinesh Company), and (2) Automatic sphygmomanometer (Omron Company)
Study design
According to the following inclusion criteria, 50 patients ranging from 30 to 50 years participated in this study. In all patients, changes in heart rate, blood pressure, and also pulse oximetry were examined during five steps; the first step before injecting the anesthetic, the second step after the anesthetic injection and before the incision, the third step after the incision, the forth step after debridement, and the fifth step following stitching and the end of the operation.
It should be noted that all the operations were performed by one surgeon, and all patients received two anesthetic cartridges containing lidocaine (2%) and epinephrine (1:80000) (Darou Pakhsh Company), using the infiltration technique into the vestibular depth and interdental papilla and also hard palate mucosa, in anterior 1/6 region and incisive canal; no additional anesthetic cartridge was used during surgery, and those in need of re-injection were excluded from the study.
SpO2 and hemodynamic alterations were assessed using the automatic sphygmomanometer and pulse oximeter attached to the patient's finger during surgery.
Inclusion criteria
Having no systemic disease to be considered as contraindication of periodontal surgery or affecting the heart rate and blood pressure
Having no sensitivity to anesthetics
Not being in pregnancy or lactation period.
Statistical analysis
Data were analyzed by SPSS statistical software using ANOVA repeated measure test, and P < 0.05 was considered as statistically significant level.
RESULTS
The present research has been implemented on 50 patients referring to Periodontology Department of Dental Faculty for periodontal surgery. Among the study participants with the mean age of 42.58 ± 7.14 years, ranging from 30 to 55 years old, there were 22 men and 28 women. In all cases, systolic and diastolic blood pressure, heart rate, and SpO2 were evaluated during five stages; the first step before injecting the anesthetic, the second step after the anesthetic injection and before the incision, the third step after the incision, the forth step after debridement, and the fifth step following stitching and the end of the operation.
The Mean±SD systolic blood pressure
The mean systolic blood pressure was highest in the second stage and lowest in the first one. In the five steps studied, there was a significant difference between the first step and the second (P < 0.0001) and the third (P = 0.001), the second step and the first (P = 0.001) and the fourth and the fifth (P < 0.0001), the third step and the first (P = 0.001) and the fourth (P = 0.010), the fourth step and the second (P < 0.0001) and the third (P = 0.010), and also the fifth step and the second (P < 0.0001) [Table 1 and Figure 1].
Table 1.
Comparison of the Mean±SD SB* during the five stages of modified Widman flap surgery
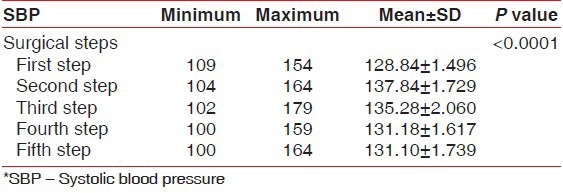
Figure 1.
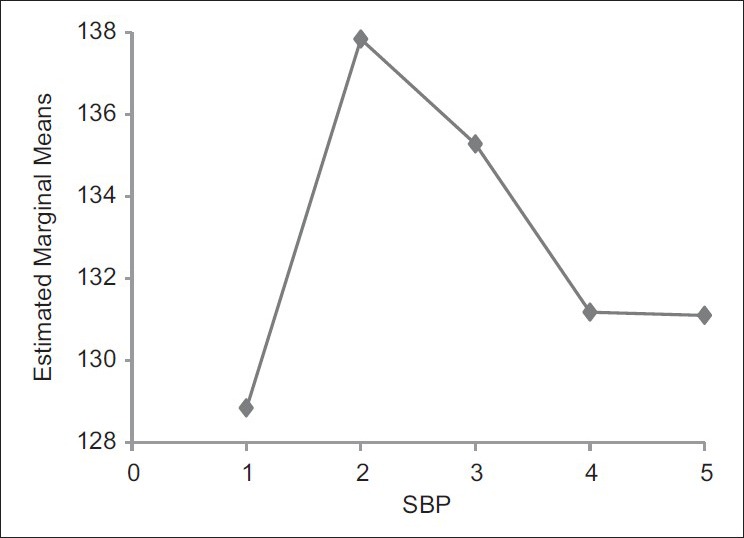
SBP changes during the five stages of modified Widman flap surgery
The Mean±SD diastolic blood pressure
The maximum and the minimum diastolic blood pressures were, respectively, obtained in the second and the first stage. Statistical analysis showed significant difference between the first stage and the second (P = 0.001), the second stage and the first (P = 0.001) and the third (P < 0.0001) and the fourth (P = 0.003), the third stage and the second (P < 0.0001), and the fourth step and the second (P = 0.003); however, no meaningful relationship was found between the fifth step and the other stages [Table 2 and Figure 2].
Table 2.
Comparison of the Mean±SD DBP* during the five stages of modified Widman flap surgery
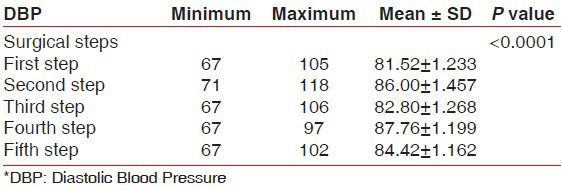
Figure 2.

DBP changes during the five stages of modified Widman flap surgery
The Mean±SD heart rate
According to statistical analysis, the maximum and the minimum heart rate was respectively observed in the second and the fifth stage. Significant differences were found between the first step and the second and the third (P < 0.0001), the second and the third steps and the other stages, the fourth step and the second and the third (P < 0.0001) and the fifth (P = 0.001), and also the fifth step with the second and the third (P < 0.0001) and the fourth (P = 0.001) steps [Table 3 and Figure 3].
Table 3.
Comparison of the Mean±SD HR* during the five stages of modified Widman flap surgery
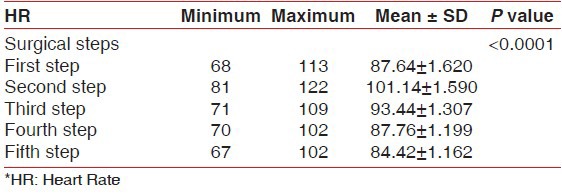
Figure 3.
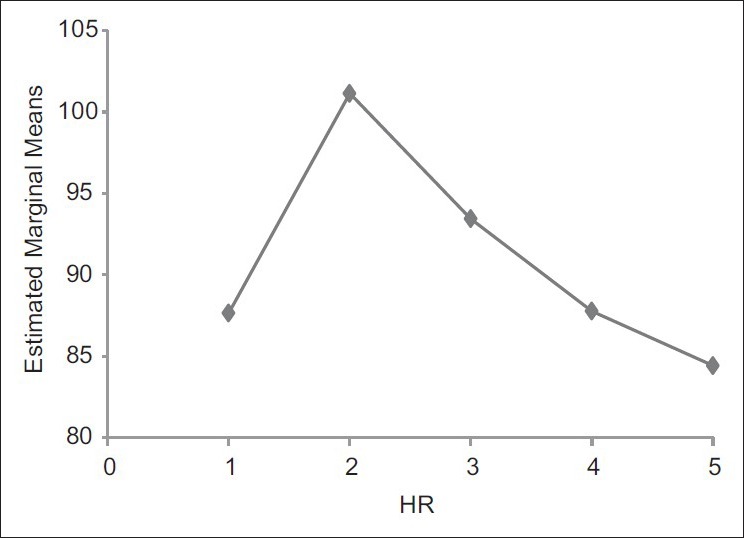
Changes in HR during the five stages of modified Widman flap surgery
The Mean±SD SpO2
Similarly, based on statistical analysis, no significant difference has been achieved in the mean SpO2 during the five stages studied (P > 0.05) [Table 4 and Figure 4].
Table 4.
Comparison of the Mean±SD SpO2* during the five stages of modified Widman flap surgery
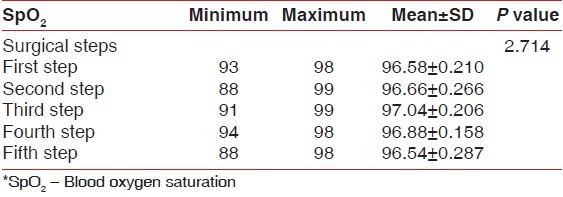
Figure 4.
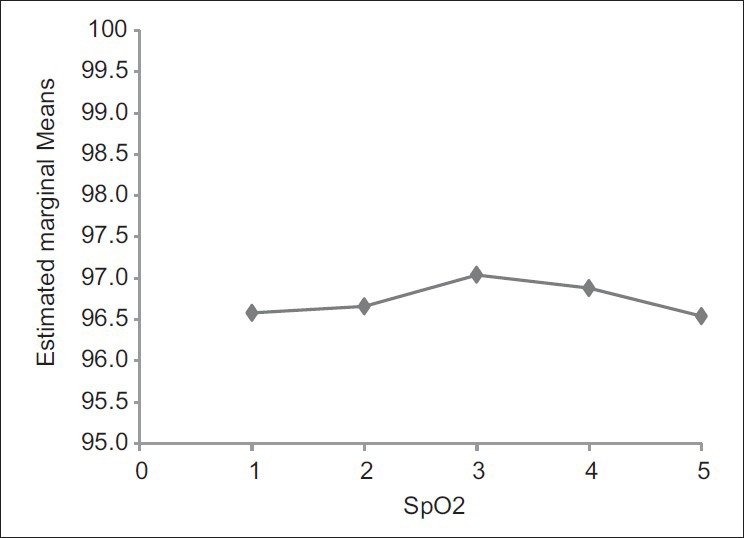
SpO2 variability during the five stages of modified Widman flap surgery
DISCUSSION
Hemodynamic changes during dental treatment have long been one of the main concerns among practitioners and researchers.[8] Increase in blood pressure and heart rate during surgery is inevitable; however, the effect of sympathetic nervous system is not well-identified on this augmentation. Since the use of local anesthesia does not merely contribute to increased concentration of plasma noradrenaline without dental treatment, blood pressure response appears to be depending on dental treatment process itself.[9]
As mentioned earlier, elevated blood pressure during oral surgery is attributed to the sympathetic nervous system. Due to possessing vasoconstrictors and anesthetic components, local anesthesia exerts different effects. Adrenaline is used as a vasoconstrictor along with lidocaine to increase the amount and duration of anesthesia. Besides, adrenaline acts as hemostats during surgery and leaves several hemodynamic effects.[10] Moreover, many researchers have pointed to changes probably effective on normal patients’ physiological stability. Sedative drugs and local anesthetics can be used to control the autonomic nervous system responses and help to reduce the cardiovascular alterations.[8] In addition, different people react differently to anxiety and pain, which could be significantly influential on their hemodynamic alterations.
In the present study, blood pressure and heart rate were remarkably increased after injection of anesthesia (P < 0.05). According to Figures 1, 2, and 3, a meaningful difference has been found in the second step and following the anesthetic injection containing lidocaine and epinephrine (1:80000) (P < 0.0001) in systolic and diastolic blood pressure and heart rate, on which the result was almost predictable. This can be associated with hemodynamic effects of adrenaline, as well as alpha-adrenergic effects to peripheral vasoconstriction and beta-adrenergic effects to increased cardiac contraction. Furthermore, patient's physiological stress before surgery and also painful stimulus following injection might lead to increased sympathetic activity and subsequently blood pressure and heart rate. Thus, application of anxiety-reducing protocols such as psychological sedatives during treatment and minimizing patient's waiting time can greatly control endogenous secretion of adrenaline. The study figures present a reduction in systolic and diastolic blood pressure following the second step and during the third, fourth, and fifth steps, indicating the elimination of stimulatory effect of adrenaline on blood pressure and heart rate and showing insignificant impact of other surgical steps on vital signs in cases of no anesthetics injection. Furthermore, over time and acceptance of treatment processes by patient, the initial anxiety will be diminished and the person will reach to a relatively stable cardiovascular balance.
Since the peak effects of local anesthetics and alpha and beta epinephrine impact elimination occur in the third and the fourth steps, decrement in heart rate and blood pressure seems to be obvious in these stages.
According to Figure 2, diastolic blood pressure has been slightly elevated in the fifth step, after stitching at the end of the operation, which is probably due to feeling of pain by patient and decrease in the effect of anesthetic.
In a study by Matsumura et al. investigating changes in blood pressure and heart rate during dental surgery, the results revealed an increase in both parameters after anesthesia with lidocaine (2%) and epinephrine (1:80000), which is compatible to findings of the present research.[2]
In Faraco et al. survey on the effect of anesthetics containing lidocaine and epinephrine on cardiovascular changes during dental implant surgery, blood pressure was evaluated using the automated noninvasive oscillometric technique during ten steps; the results showed no significant difference in blood pressure and heart rate variability,[7] which is not in accordance to the findings achieved in this research.
In another study by Gedik et al. on blood pressure, heart rate and temperature variability during periodontal surgery, patients were divided into four groups according to types of surgery, and blood pressure and heart rate were measured after anesthetic injection and the end of the operation; blood pressure and heart rate were decreased in patients undergoing gingivectomy and periodontal flap, which is in consistence with the results obtained in the present research. However, no changes in heart rate and blood pressure have been observed following frenectomy and curettage,[9] indicating that the difficulty in treatment process is an effective factor in blood pressure.
As shown in Figure 4, no statistically significant difference has been found in the mean SpO2, measured by pulse oximetry, in different stages (P > 0.05). In other words, conventional periodontal surgery with technical and safety observations does not bring hypoxia in healthy subjects.
In an investigation by Kaviani and Birang, nausea, vomiting, decreased or increased blood pressure and other hypoxia complications following the use of nitrous oxide inhalation sedation during periodontal treatment have only been observed in 1 out of 32 cases, which was probably due to patient restlessness and movement during treatment.[11]
Matthews et al. have addressed to pulse oximetry during oral surgery with and without intravenous sedation and found out a significant reduction in arterial blood oxygen levels in the group receiving midazolam. This study illustrates remarkable sedative effect of midazolam on anxious patient prior to the surgery; nonetheless, this effect does not sustain during the operation.[4]
As mentioned, findings of various studies in terms of hemodynamic changes following dental treatments are contradictory, and such discrepancies could be related to different research approaches and different local anesthetics applied.
CONCLUSION
Different surgical stages will be accompanied by diverse effects on hemodynamic variability and pulse oximetry. According to the present study, blood pressure and heart rate are significantly increased after anesthetic injection and are decreased in the following stages by the elimination of adrenaline stimulatory effect. Moreover, no significant alteration has been observed in SpO2 during the operational steps in this research.
ACKNOWLEDGEMENTS
We wish to thank Dr. Majid Fereyduni and Dr. Parand keshavarzi for their assistance in this study.
Clinical Relevance
Based on the acquired data of the present study, due to the hemodynamic alterations obtained during various stages of periodontal surgery (Modified widman flap), it is preferred for the patients, particularly cardiovascular sufferers to be monitored. Therefore, the re-injection of anesthetic drug can be performed in various stages of the surgery appropriately and be avoided from sudden changes in vital signs to some extents.
Footnotes
Source of Support: The corresponding author has had full access to all the data in the study and has final responsibility for the decision to submit for publication. No external funding was used for this study
Conflict of Interest: No.
REFERENCES
- 1.Wilson KE, Dorman ML, Moore PA, Gird NM. Pain Control and anxiety management for periodontal therapies. Periodontol 2000. 2008;46:42–55. doi: 10.1111/j.1600-0757.2008.00245.x. [DOI] [PubMed] [Google Scholar]
- 2.Matsumura K, Miura K, Takata Y, Kurokawa H, Kajiyama M, Abe I, et al. Changes in blood pressure and heart rate variability during dental surgery. Am J Hypertens. 1998;11:1376–80. doi: 10.1016/s0895-7061(98)00157-5. [DOI] [PubMed] [Google Scholar]
- 3.Stoeling RK, Miller RD. 5th ed. Philadelphia: Churchill Livingstone; 2006. Text Book of Basics of Anesthesia. [Google Scholar]
- 4.Matthews RW, Malkawi Z, Griffiths MJ, Scully C. Pulse oximetry during minor oral surgery with and without intravenous sedation. J Oral Surg Oral Med Oral Pathol. 1992;74:537–43. doi: 10.1016/0030-4220(92)90339-r. [DOI] [PubMed] [Google Scholar]
- 5.Brand HS, Gortzak RA, Palmer-Bouva CC, Abraham RE, Abraham-Inpijn L. Cardiovascular and neuroendocrine responses during acute stress induced by different types of dental treatment. Int Dent J. 1995;45:45–8. [PubMed] [Google Scholar]
- 6.Bayat M, Zaeri F, Sadatnia F. Comparison of o 2 saturation, heart and respiratory rate following injection of vasoconstrictor containing anesthetic (lidocaine 2%) and without vasoconstrictor anesthetic (Mepivacaine) J Dent Tehran Univ Med Sci. 2005;18:45–50. [Google Scholar]
- 7.Faraco FN, Kawakami PY, Mestnik MJ, Ferrari DS, Shibli JA. Effect of Ansethetics containing lidocaine and epinephrine on cardiovascular changes during dental implant surgery. J Oral Implantol. 2007;33:84–8. doi: 10.1563/0.845.1. [DOI] [PubMed] [Google Scholar]
- 8.Faraco FN, Armonia PL, Simone JL, Tortamano N. Assessment of cardiovascular parameters during dental procedures under the effect of benzodiazepines: A double blind study. Braz Dent J. 2003;14:215–9. doi: 10.1590/s0103-64402003000300014. [DOI] [PubMed] [Google Scholar]
- 9.Gedik RG, Marakoglu I, Demirer S. Blood pressure, heart rate and temperature variability during periodontal surgery. West Indian Med J. 2005;54:329–33. doi: 10.1590/s0043-31442005000500011. [DOI] [PubMed] [Google Scholar]
- 10.Golami GA, Ghamari M, Ghanavati F, Fathieh AR, Akbarzadeh AR, Araban N. The effect of lidocaine and Prilocaine on blood pressure, pulse rate and anxiety to undergo periodontal surgery. J Dent Shahid Beheshti Univ Med Sci. 2008;26:382–9. [Google Scholar]
- 11.Kaviani N, Birang R. Evaluation of need to pulse oximetry monitoring during inhalation sedation for priodontal treatments. Dent Res J. 2006;3:1–5. [Google Scholar]