

Sir,
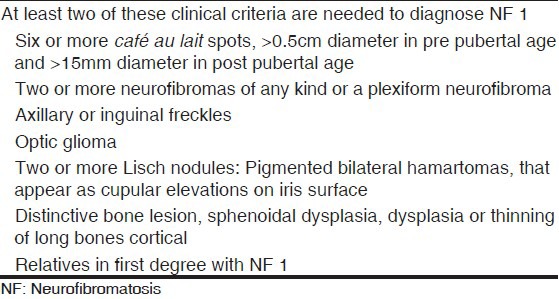
Neurofibromatosis (NF) is an autosomal-dominant disorder that affects the nervous system, the skeletal system, soft tissues, and the skin. Neurofibromatosis occurs in two distinct forms: Type 1 (NF1, von Recklinghausen's disease) and type 2 (NF2). Type 1 NF affects 1 in 4000 people and is usually diagnosed during childhood. Patients are diagnosed with NF1 if they demonstrate two or more of the criteria in Table 1.[1]
Table 1.
Clinical criteria for the diagnosis of NF-1
In NF1, there have been structural anatomical features include skin pigmentation, discrete plexiform neurofibromata, and tumors of neuronal origin both in the central nervous system and peripheral nerves, ocular lesions, skeletal and other miscellaneous features.[1,2]
In literature, the association of NF1 with Chiari 1 malformation and syringomyelia have been previously rarely described.[3] Here, we reported a patient who had a combination of optic-pathway glioma, scoliosis, Chiari type 1 malformation, and syringomyelia with skin lesions as a variant form of NF1. A 16 years-old-girl presented with skin pigmentation, short stature, and increasing numbness on the upper left arm for past one year. Her parents were non-consanguineous. Describe the same cutaneous lesions in other family members. On her examination, the vital signs, including the blood pressure were normal. Her height was short (135 cm) for her age. More than six café au lait spots over 15 mm diameter could be seen throughout her skin. Axillary and inguinal freckles were also present. She had mild scoliosis. Ophthalmic evaluation showed bilaterally Lisch nodules in the iris. On neurological examination, there was light touch and pin-prick hypoesthesia in the left arm. The remainder of the physical and neurological examination was unremarkable. Cerebral, spinal, and orbital magnetic resonance imaging (MRI) were performed. The brain MRI showed Chiari type 1 malformation and hamartomatous lesion in the right basal ganglia [Figure 1]. Syringomyelia was noted in the C3 to T7 level in the spinal MRI [Figure 2]. Orbital MRI showed right optic pathway glioma. The NF1 was diagnosed based on these clinical, and radiological criteria. The MRI findings suggested Chiari 1 malformation, optic pathway glioma, and syringomyelia besides with NF1 lesions.
Figure 1.

Magnetic resonance imaging brain scan shows Chiari malformation
Figure 2.

Cervico-torachal syringomyelia in the spinal MRI
Neurofibromatosis is a disorder with a wide spectrum of clinical manifestations. Many organ systems can be affected. Chiari type 1 malformation and ventriculomegaly in NF1 were first described by Afifi et al.[4] The two cases had skeletal anomalies but no brain tumors to account for the ventriculomegaly. Since then, a few cases were described with Chiari 1 malformation and ventriculomegaly in the literature. Dooley et al. and Battistella et al. reported Chiari type 1 malformation with NF1.[5,6] Another case described by Fernandez et al. a patient of NF1 with Chiari malformation, syringomyelia, and scoliosis.[7] They suggested that Chiari type 1 malformation should be considered as a cause of non-tumoral ventricular enlargement, coincidental, or variety of cerebral dysplasias in patients with NF1. Chakrawarthy et al.[3] reported a case of optic pathway glioma, Chiari 1 malformation, syringomyelia, and scoliosis as a variant of NF1. Interestingly, their patient had no cutaneous lesions for NF1. Tubbs et al. have retrospectively reported two large groups of pediatric patients. Group I, with the primary diagnosis of Chiari I malformation, who have undergone posterior fossa decompression for symptomatology; and group II patients, who have been observed in their hospital's NF clinic for evaluation. Of 130 surgically addressed Chiari I malformations (Group I), they determined that 5.4% of these patients had the additional diagnosis of NF1. Of group II patients who underwent imaging of the brain, 8.6% were found to have a concomitant Chiari I malformation.[8] In addition, individuals with NF1 are prone to the development of both benign and malignant tumors. The most common central nervous system tumor in children and adults with NF1 is the glioma.[1] In childhood, gliomas are primarily located in the optic pathway, that occur in about 15% of cases with NF1 but about of a third of all optic pathway gliomas have underlying NF1.[9] Our patient had a combination of optic pathway glioma, Chiari type 1 malformation, syringomyelia, and scoliosis, Also, she had cutaneous lesions and Lisch nodules in the iris for NF1. Due to the heterogeneity of the disorder many authors have suggested including these as variants of NF1. Genetic studies will help to classify variants. We suggest Chiari 1 malformation, syringomyelia and scoliosis could be more common in NF1 than clinicians appreciate. Therefore, routine screening of children with NF1 for Chiari 1 malformation and syringomyelia around 10 years of age may detect the onset of these abnormalities early.
References
- 1.Jett K, Friedman JM. Clinical and genetic aspects of neurofibromatosis 1. Genet Med. 2010;12:1–11. doi: 10.1097/GIM.0b013e3181bf15e3. [DOI] [PubMed] [Google Scholar]
- 2.Boyd KP, Korf BR, Theos A. Neurofibromatosis type 1. J Am Acad Dermatol. 2009;61:1–14. doi: 10.1016/j.jaad.2008.12.051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chakravarty A, Bhargava A, Nandy S. A patient with optic pathway glioma, scoliosis, Chiari type I malformation and syringomyelia: is it Neurofibromatosis type 1? Neurol India. 2002;50:520–1. [PubMed] [Google Scholar]
- 4.Afifi AK, Dolan KD, Van Gilder JC, Fincham RW. Ventriculomegaly in neurofibromatosis-1. Association of Chiari type 1 malformation. Neurofibromatosis. 1988;1:299–305. [PubMed] [Google Scholar]
- 5.Dooley J, Vaughan D, Riding M, Camfield P. The association of Chiari type 1 malformation and neurofibromatosis type 1. Clin Paediatr. 1993;32:189–90. doi: 10.1177/000992289303200316. [DOI] [PubMed] [Google Scholar]
- 6.Battistella PA, Perilongo G, Catollo C. Neurofibromatosis type 1 and type 1 Chiari type 1 malformation: An unusual association. Child's Nerv Syst. 1996;12:336–8. doi: 10.1007/BF00301023. [DOI] [PubMed] [Google Scholar]
- 7.Fernandez JA, Calleja PB, Paseual CI. Syringomyelia, Chiari 1 malformation and scoliosis in a patient with type 1 neurofibromatosis. An Esp Paediatric. 1998;48:522–4. [PubMed] [Google Scholar]
- 8.Tubbs RS, Rutledge SL, Kosentka A, Bartolucci AA, Oakes WJ. Chiari 1 malformations and Neurofibromatosis type 1. Paediatr Neurol. 2004;30:278–80. doi: 10.1016/j.pediatrneurol.2003.09.013. [DOI] [PubMed] [Google Scholar]
- 9.Listernick R, Ferner RE, Liu GT, Gutmann DH. Optic pathway gliomas in neurofibromatosis-1: Controversies and recommendations. Ann Neurol. 2007;61:189–98. doi: 10.1002/ana.21107. [DOI] [PMC free article] [PubMed] [Google Scholar]