

Abstract
Rapid eye movement (REM) sleep behavior disorder is a condition characterized by dream enactment. This condition may accompany neurodegenerative disorders. However, only a few reports from India are available, that too, without any polysomnographic evidence. We are reporting a case of REM sleep behavior disorder with polysomnographic evidence.
Keywords: Parkinson's diasease, polysomnography, REM sleep behavior disorder
Introduction
Parkinson's disease (PD) is a chronic progressive neurodegenerative disorder that typically affects the male with a mean onset of symptoms at age 60 years.[1] Neuropathologically, the loss of neurons is not limited to dopaminergic neurons in the substantia nigra, but also involves the serotonergic, noradrenergic and the cholinergic nuclei which accounts for non-motor symptoms such as emotional and cognitive impairment, autonomic dysfunction, and sleep disorders.[2,3,4]
Sleep disorders and nocturnal problems are common in PD and they are seen in approximately 90% of PD patients.[3,4] Sleep problems with PD include insomnia, hypersomnia, restless legs syndrome, nocturnal leg cramps, circadian rhythm disorders and the very interesting phenomenon, REM sleep behavior disorder (RBD).[3,5] Of note, RBD may precede the typical manifestations of PD and other synucleinopathies such as multiple system atrophy and Lewy body dementia by many years.[6,7]
The prevalence of PD in India varies greatly depending upon geographical area, from a relatively low of 14-41/100,000 in non-Parsi communities to an exceptionally high of 328/100,000 in Parsi communities.[8] Using clinical criteria without confirmation by polysomnography for the diagnosis of RBD, Vibha et al.[9] reported the prevalence of RBD of 19.4% in a case control study of patients with PD from North India. Most parasomnia episodes described were brief and were not associated with violent behavior.
Polysomnography is a useful tool for the diagnoses of sleep disorders. Its diagnostic utility is not limited to sleep apnea. Rather, it helps in picking up the underlying causes for chronic insomnias, hypersomnia, nocturnal epilepsy, periodic limb movement during sleep (PLMS) and parasomnias viz., sleep-talking, sleep-walking, and night-terrors. REM sleep behavior disorders is a parasomnia, of rapid eye movement (REM) sleep. It is characterized by absence of muscle atonia, which is normally seen during the REM sleep. Clinically, it manifests as an episode of dream enactment that is often violent and may result in self-injury or an injury to the bed partner.[3,5] However, other entities e.g., nocturnal epilepsy, sleep-walking, sleep-terrors, etc., may also be clinically present with violent behavior during sleep. Hence, polysomnography is essential in diagnosis of REM-sleep-behavior-disorder. Further, it can also provide us an idea not only regarding the severity but also about the etiology of sleep disorders e.g. PLMS, insomnia, and hypersomnia which are commonly seen in PD.[3,5]
We, herein, present a patient with PD with REM sleep behavior disorder in whom the diagnosis was objectively confirmed by polysomnography.
Case Report
A 55-year-old male presented with the complaints of non-refreshing sleep, excessive drowsiness during the day but, without experiencing irresistible sleepiness. He also had a history of nocturnal symptoms for the past 2.5 years manifesting as somniloquy and abnormal sleep behavior. On a recent visit to his attending neurologist (DG), his wife complained of increasing frequency of abnormal activity during sleep after which he was referred to a sleep specialist (RG).
According to his wife, he followed a regular sleep schedule (bedtime: 11:00 pm and wake-time: 5:00 am). His wife reported that he used to have episodes of sleep talking (4-5 times/night), each lasting 10-15 minutes on most of the nights. At times, he also appeared enacting his dreams. During night-time acts his movements used to be a combination of sitting up in bed, kicking, searching, and picking. He had occasionally struck his wife and also fallen out of bed during these episodes. He himself reported having violent dreams during the night in which he was fighting with somebody. Content of the dreams varied and he reported being engaged in searching activity after losing some belongings in dreams. On few occasions, he woke up during these dreams and found that he was acting on his dreams. He snored (Grade II) but apneas were never witnessed by the bed-partner. Any kind of behavioral abnormality was never noticed during daytime. His Epworth Sleepiness score was 6 (normal < 10).
He had developed resting tremor in the right hand 8 years earlier back subsequent to an alleged insecticide exposure. He was then diagnosed as PD by a neurologist. Presently, the patient was suffering from stage-II (Hoehn and Yahr Staging). Since then he had been on treatment with a combination of drugs that included carbidopa/levodopa 10/100 mg bid, amantadine 100 mg bid and pramipexole 0.25 mg bid. He responded well to these drugs and symptoms of PD improved. It must be noted here that he changed the dose of levodopa/carbidopa on his own in spite of counseling and efforts by doctor and family members. In addition, many a times he had presented with dyskinesia. Hence, the dose of levodopa was kept low, but it is difficult to comment whether he was taking the prescribed doses or higher doses.
There was no history to suggest childhood parasomnias, restless leg syndrome, sleep-terrors, narcolepsy, closed head injury, seizures, alcohol use, consumption or therapy with antidepressants. Also, there was no history of PD or RBD in the family members.
Physical examination revealed that he weighed 65 kgs, was 165 cms tall (BMI = 23.9). He had Mallampatti grade III airway with neck circumference of 38 cms. Neurological examination was unremarkable except for postural tremors in his hands. MRI scan of brain was non-diagnostic. Diagnostic polysomnography was performed (see below) confirming the diagnosis of RBD after which he was treated with clonazepam 1.0 mg at bedtime. One week later, his wife reported a significant reduction in frequency of these episodes. The dose was escalated to 1.5 mg for optimal suppression of the behavior.
Sleep study
Standard attended 17-channel polysomnography with video monitoring using Cadwell III Sleep Easy acquisition system (Cadwell Laboratories, Inc., Kennewick, WA.) was performed. Electrophysiologic sleep parameters included frontal, central, and occipital electroencephalogram, right and left electrooculogram, and submentalis electromyogram. Anterior tibialis electromyogram was recorded to assess limb movement activity. Airflow was detected by thermistors and respiratory effort was determined by measurement of chest and abdomen motion with piezoelectric sensors. The arterial oxygen saturation was measured by the Cadwell oximeter with a 4-beat averaging mode. Raw data was manually scored in 30-second epochs for sleep stages using standard criteria.[10]
Results of sleep measurements are shown in the Table 1. The hypnogram [Figure 1a] showed poor sleep continuity but total sleep time and REM duration that were adequate for evaluation. REM latency was longer than usual (170 minutes compared to normal approximately 90 minutes) but the amount of REM sleep was within normal limits (22% total sleep time; normal approximately 20-25%). Periodic limb movement index (PLMS) was mildly increased (12/hr; normal approximately 5/hr). Respiratory parameters were normal. The AHI measured 1/hr (normal < 5/hr) and there was no hypoxemia. Video monitoring depicted periods of frequent movements of the arms and legs associated with vocalizations and sitting up in bed developing strictly out of REM sleep [Video 1]. In addition, excessive phasic activity was noted in the submentalis and anterior tibialis recordings with movement artifacts during REM sleep [Figure 1].
Table 1.
Distribution of sleep stages
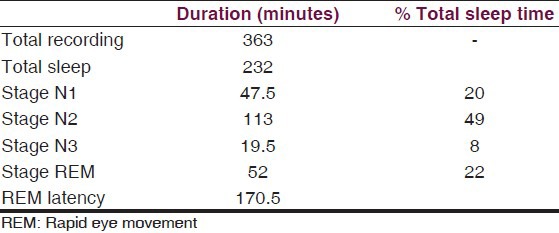
Figure 1.
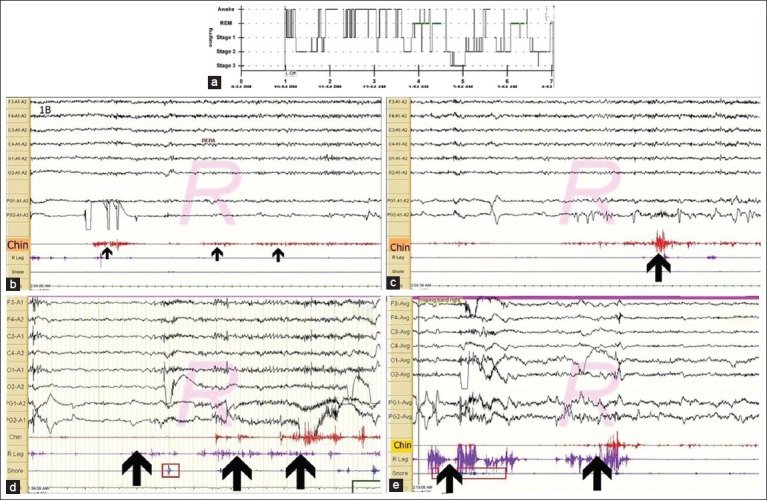
Hypnogram showing sleep staging (a); 30 seconds REM epochs depicting Submentalis muscle atonia (>20 sec) (b); Excessive phasic muscle activity (c); Movements during REM (d) and (e)
Discussion
This case illustrates the typical symptoms and polysomnographic findings in a patient with PD who later on developed clinical REM sleep behavior disorder. For a more complete description of all the sleep disorders associated with PD, especially the RBD and putative mechanisms as well to understand its relationship to neurodegenerative diseases, the readers are referred to recent references.[3,5,11]
Patients with RBD are typically elderly males who present with variable degrees of excessive and sometimes violent behavior especially during the later third of the night when REM sleep is most abundant.[11] These disturbances can be extremely troubling to the bed partner and serious injuries can occur. In some cases, complex movements with abnormal behavior are not found with sleep testing; however, other markers of the condition that may be observed include excessive phasic activity during REM sleep or REM sleep without atonia.[12] This sleep disorder may be the heralding manifestation of PD by many years or as in this case may develop years after the onset and such cases may be diagnosed as idiopathic RBD.[9] At present, it is not possible to accurately predict who would develop PD after the idiopathic RBD has been diagnosed, although, one study suggests that patients without REM atonia in chin EMG are at higher risk.[6] Similarly, it has been observed that PD patients who exhibit predominantly non-tremor manifestations, increased fall rates and show a poor response to dopaminergic medications develop RBD in due course of illness.[13] Hence, all RBD patients should be evaluated for PD and other neurodegenerative disorders and vice-versa.[3,14] Recognition of RBD prior to the onset of motor symptoms with PD is extremely important as this may enable earlier diagnosis and implementation of therapy for PD.[6,14,15]
Clinically, dream enactment behavior suggests the diagnosis of RBD, however, a clinical diagnosis without confirmation by overnight polysomnography may be misleading as dream enactment behavior is also a manifestation of benign parasomnias characterized by somnambulism or night terrors. Abnormal behavior is found in other situations e.g., obstructive sleep apnea, epilepsy, and substance withdrawal as well.[11] The condition may be precipitated by serotonin reuptake inhibitors and may follow closed head injuries. Loss of normal EMG atonia during REM sleep or excessive phasic activity in the submentalis muscle documented by polysomnography and a history of dream enactment are required for accurately diagnosing RBD.[7,11] The present case fulfilled both of these criteria. In addition to above findings, elevated PLMS index was also observed, i.e. increased number of periodic limb movements during sleep (PLMS). PLMS are associated with restless legs syndrome, RBD, and narcolepsy.[7] Although, these movements are seen during non-REM sleep in RLS, they are present during REM sleep only in patients with RBD.[7] We observed similar findings in the present case [Figure 1]. Hence, PLMS in this case did not require a separate diagnosis, especially when the clinical symptoms of RLS were not present. REM sleep behavior disorder has been found to respond well to clonazepam as in the present case and previously as well (typical effective doses 0.5-1.5 mg at bedtime).[16,17,18] Other medications such as melatonin have been used although with much less success.[16,17,18]
In conclusion, REM sleep behavior disorder is common in PD and antedates the PD in many cases. RBD mimics a number of other sleep disorders and polysomnography must be used to reach to a final diagnosis.
Videos available on www.ruralneuropractice.com
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Van Den Eeden SK, Tanner CM, Bernstein AL, Fross RD, Leimpeter A, Bloch DA, et al. Incidence of parkinson's disease: Variation by age, gender, and race/ethnicity. Am J Epidemiol. 2003;11:1015–22. doi: 10.1093/aje/kwg068. [DOI] [PubMed] [Google Scholar]
- 2.Wolters EC. Non-motor extranigral signs and symptoms in Parkinson's disease. Parkinsonism Relat Disord. 2009;15(Suppl 3):S6–12. doi: 10.1016/S1353-8020(09)70770-9. [DOI] [PubMed] [Google Scholar]
- 3.Suzuki K, Miyamato M, Iwanami M, Hirata K. Sleep disturbances associated with Parkinson's disease. Parkinsons Dis 2011. [Last cited in 2012 May 25]. p. 2011. (2011): [About 10 p.] Available from: http://www.hindawi.com/journals/pd/2011/219056/cta . [DOI] [PMC free article] [PubMed]
- 4.Yong MH, Fook-Chong S, Pavanni R, Lim LL, Tan EK. Case control polysomnographic studies of sleep disorders in parkinson's disease. [Last cited in 2012 May 25];PLoS One. 2011 6:e22511. doi: 10.1371/journal.pone.0022511. Available from: http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone. 0022511 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Menza M, Dobkin RD, Marin H, Bienfait K. Sleep disturbances in parkinson's disease. Mov Disord. 2010;25(Suppl 1):S117–22. doi: 10.1002/mds.22788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Postuma RB, Gagnon JF, Rompre S, Montplaisir J. Severity of REM atonia loss in idiopathic REM behaviour disorder predicts Parkinson's disease. Neurology. 2010;74:239–44. doi: 10.1212/WNL.0b013e3181ca0166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Diagnostic and coding manual. 2nd ed. Westchester, Illinois: American Academy of Sleep Medicine; 2005. American Academy of Sleep Medicine. International classification of sleep disorders. [Google Scholar]
- 8.Bharucha NE, Bharucha EP, Bharucha AE, Bhise AV, Schoenberg BS. Prevalence of Parkinson's disease in the Parsi community of Bombay, India. Arch Neurol. 1988;45:1321–3. doi: 10.1001/archneur.1988.00520360039008. [DOI] [PubMed] [Google Scholar]
- 9.Vibha D, Shukla G, Goyal V, Singh S, Srivastava AK, Behari M. RBD in Parkinson's disease: A clinical case control study from North India. Clin Neurol Neurosurg. 2011;113:472–6. doi: 10.1016/j.clineuro.2011.02.007. [DOI] [PubMed] [Google Scholar]
- 10.Iber C, Ancoli-Israel S, Chesson A, Quan SF, editors. Westchester, IL: American Academy of Sleep Medicine; 2007. The AASM manual for the scoring of sleep and associated events: Rules, terminology, and technical specification. [Google Scholar]
- 11.Boeve BF. REM sleep behavior disorder: Updated review of core features, the RBD-neurodegenerative disease association, evolving concepts, controversies and future direction. Ann N Y Acad Sci. 2010;1184:15–54. doi: 10.1111/j.1749-6632.2009.05115.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bliwise DL, Rye DB. Elevated PEM (phasic electromyographic metric) rates identify rapid eye movement behavior disorder patients on nights without behavioral abnormalities. Sleep. 2008;31:853–7. doi: 10.1093/sleep/31.6.853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Postuma RB, Gagnon JF, Vendette M, Charland K, Montplaisir J. REM sleep behaviour disorder in Parkinson's disease is associated with specific motor features. J Neurol Neurosurg Psychiatry. 2008;79:1117–21. doi: 10.1136/jnnp.2008.149195. [DOI] [PubMed] [Google Scholar]
- 14.Claassen DO, Josephs KA, Ahlskog JE, Silber MH, Tippmann-Peikert M, Boeve BF. REM sleep behavior disorder preceding other aspects of synucleinopathies by up to half a century. Neurology. 2010;75:494–9. doi: 10.1212/WNL.0b013e3181ec7fac. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bugalho P, da Silva JA, Neto B. Clinical features associated with REM sleep behavior disorder symptoms in the early stages of Parkinson's disease. J Neurol. 2011;258:50–5. doi: 10.1007/s00415-010-5679-0. [DOI] [PubMed] [Google Scholar]
- 16.Trotti LM. REM sleep behaviour disorder in older individuals: Epidemiology, pathophysiology and management. Drugs Aging. 2010;27:457–70. doi: 10.2165/11536260-000000000-00000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Aurora RN, Zak RS, Maganti RK, Auerbach SH, Casey KR, Chowdhuri S, et al. Standards of Practice Committee; American Academy of Sleep Medicine. Best practice guide for the treatment of REM sleep behavior disorder (RBD) J Clin Sleep Med. 2010;6:85–95. [PMC free article] [PubMed] [Google Scholar]
- 18.Anderson KN, Shneerson JM. Drug treatment of REM sleep behavior disorder: The use of drug therapies other than clonazepam. J Clin Sleep Med. 2009;5:235–9. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.