

Abstract
Introduction
This study investigated procedural errors made during root canal preparation using stainless steel and nickel-titanium (NiTi) instruments by undergraduate students, using two diagnostic imaging methods.
Materials and Methods
Sixty human molars were divided into three groups (n=20; group 1: K-Flexofile, group 2: K3, and group 3: BioRace). The root canals were filled with gutta-percha and AH Plus. Periapical radiographs and cone beam computed tomography (CBCT) images were obtained to detect procedural errors made by undergraduate students during root canal preparation. Two examiners evaluated the presence or absence of fractured instruments, perforations and canal transportations. The agreement between observers was assessed using the kappa coefficient. The Kolmogorov-Smirnov, Fisher exact, ANOVA and Tukey tests were used for statistical analysis. The level of significance was set at 5%.
Results
There were no significant differences in detecting procedural errors between two- and three-dimensional diagnostic imaging methods. There were no significant differences in procedural errors between stainless steel and NiTi instruments. Mean preparation time was recorded in minutes, and results were significantly different between the three groups. NiTi instruments had the lowest mean preparation time.
Conclusion
Both periapical radiographs and CBCT identified procedural errors, however, three-dimensional images offered more diagnostic resources. The frequency of procedural errors was low for any of the endodontic instruments despite being used by inexperienced operators.
Keywords: Cone Beam Computed Tomography, Dental Education, Dental Instruments, Nickel-Titanium, Perforation, Root Canal Preparation
Introduction
Contemporary endodontics has undergone important changes with the development of new methods and instruments. The introduction of nickel-titanium (NiTi) for orthodontic archwires, favored the production of new instruments in endodontics [1]. Walia, et al. studied the properties of this alloy in endodontic instruments, and their results gained the attention of the industry [2]. The superelasticity of NiTi enabled the preparation of curved root canals with better quality.
During last years, the use of engine-driven NiTi instruments for the preparation of curved root canals has been gradually incorporated into the curriculum of undergraduate courses. Endodontic courses for under-graduate students should include updated scientific knowledge which covers comprehensive methodological strategies as well as science of materials [3-6].
Instrumentation of curved root canals is one of the critical procedures of endodontic therapy [7]. The flexibility of NiTi instruments preserves the original shape of the root canal and ensures a better canal curvature compared to stainless steel instruments (K-flex) [8].
Several factors favor the adoption of NiTi rotary instruments for root canal preparation including a more centralized preparation, maintenance of the working length, fewer procedural errors and better quality [2, 3, 8-10]. New NiTi rotary instruments with different characteristics (cross-section, cutting angle, helical angle, radial grooves/edge, flutes, etc.) have been introduced into the profession [1, 9, 10].
Numerous dental schools have included the use of rotary instrumentation in their curriculum. However, there is still strong resistance against it. Several studies showed that undergraduate students make few procedural errors when using NiTi rotary instruments [3, 4, 11-13]. Moreover, the cost of NiTi instruments is rather low, and teaching this technique in graduate programs seems time consuming [11]. Spangberg [14] reported that although the rotary technique is not a basic procedure for undergraduate training, general practitioners and endodontists use these instruments. Therefore, it was logical and natural for schools of dentistry to teach at least one technique of using NiTi rotary instruments. Pécora et al. [5] emphasized the importance of using these mechanized systems in NiTi endodontics, as well as their application in laboratory and clinical activities during the undergraduate course.
All factors that may influence the inclusion of these resources and knowledge in the undergraduate curriculum, such as the risk of instrument fracture, root canal perforation and apical transportation, should be evaluated together with the need for preclinical training. Therefore, based on the performance of NiTi rotary instruments in the preparation of curved root canals, several studies evaluated the use of these resources in undergraduate teaching using various methods [3, 9-12].
Parallel with all advances in dentistry technologies, cone beam computed tomography (CBCT) has been used for different purposes in endodontics, such as study of root canal anatomy, three-dimensional simulation of internal and external tooth structures, evaluation of root canal preparation, obturation, retreatment, diagnosis and treatment of bone lesions [15-24]. Its ability to reduce or eliminate the superimposition of surrounding structures makes CBCT superior to conventional periapical films [22]. Compared with medical tomography, CBCT has some advantages: lower radiation dose, higher scanning resolution and more accuracy of volume measuring in different directions due to voxels being isotropic which make them different from CT [16].
Based on the importance of introducing modern root instrumentation techniques and new imaging resources into undergraduate courses, this study evaluated procedural errors made by undergraduate students during root canal preparation with stainless steel and NiTi instruments using periapical radiography and CBCT.
Material and Methods
This study was approved by the Ethics Committee of the Federal University of Goiás (Proc. # 042/2011), Brazil, and an informed consent form was obtained from all patients.
Selection and tooth preparation
Sixty extracted human maxillary and mandibular molars were obtained from the Dental Urgency Service of the School of Dentistry in Federal University of Goiás, Brazil. The teeth were stored in 0.2% thymol solution and then immersed in 5% NaOCl for 30 min to remove external organic tissues.
Image acquisition
Preoperative radiographs of each tooth were taken to confirm the absence of calcified root canals, internal/external root resorption, and the presence of a fully formed apex. Radiographic images were acquired using a Spectro X70 electronic X-Ray unit (Dabi Atlante, Ribeirão Preto, Brazil), 0.8×0.8 mm tube focal spot, Kodak Insight film-E (Eastman Kodak Co, Rochester, NY, USA) and paralleling technique. A radiographic platform was used to standardize all radiographs. All films were processed in an automatic processor, and images were evaluated in a dark room using a light box under a magnifying glass.
CBCT images were obtained using an I-CAT Cone Beam 3D imaging system (Imaging Sciences International, Hatfield, PA), with 0.20×0.20×0.20 mm voxel size and 14 bits. Images were examined using the Xoran 3.1.62 software (Xoran Technologies, Ann Arbor, MI) in a PC workstation running Microsoft Windows XP professional SP-2 (Microsoft Corp, Redmond, WA, USA).
Inclusion and exclusion criteria
Only three-canalled teeth were used in the study (maxillary molars with palatal, mesiobuccal and distobuccal canals and mandibular molars with distal, mesiobuccal and mesiolingual canals). All teeth were shorter than 22 mm, and at least one of the buccal canals of maxillary molars and the mesial canals of mandibular molars had a moderate curvature (4<radius≤8 mm). The root curvature radius (r) was estimated by methods described by Estrela et al. [18].
Standard access cavities
After taking periapical radiographs and CBCT images, standard access cavities were made by an endodontist using round diamond burs (#1013, #1014; KG Sorensen, Barueri, SP, Brazil) and Endo Z burs (Dentsply-Maillefer, Ballaigues, Switzerland), with a high speed handpiece and air-water spray cooling.
Working length determination
The working length (WL) was determined using #10 and #15 K-Flexofiles (Dentsply, Ballaigues, Switzerland) which were introduced into the root canals until being visible at the apical foramen. The WL was set 1 mm short of the apex.
Student selection
To evaluate the root canal preparation by inexpert operators, undergraduate students of the School of Dentistry of Federal University of Goiás were invited to participate in the study. Each student prepared/filed 30 root canals of each group. They did not have any experience in the preparation of curved root canals, and had an 8-h theoretical course on rotary instrumentation associated with clinical applications.
Group assignment
The root canals were randomly divided into three experimental groups of 20 teeth each (n=60 canals) and prepared using the following instruments: G1- stainless steel files (K-Flexofile, Dentsply-Maillefer, Switzerland); G2- K3 (SybronEndo, Orange, CA); and G3- BioRace (FKG Dentaire, La Chaux-de-Fonds, Switzerland).
Root canal preparation
Gates Glidden drills sizes #1 and 2 were used in G1, files #25/.10 and #25/.08 in G2, and #25/0.08 BR0 in G3 for preparation of coronal part of root canals. After working length determination, the apical third was prepared using files #15 to 40 in G1. Files up to #35 were used in mesial canals of mandibular molars and buccal canals of maxillary molars; and size #40, was the final apical preparation for the distal canals of mandibular molars and palatal canals of maxillary molars. In G2, the sequence used was #15/.02-45/.02, #25/.04 and #25/.06 for all root canals [25]. In G3, BR1 (#15/0.05), BR2 (#25/0.04), BR3 (#25/0.06), BR4 (#35/0.04) and BR5 (#40/0.04) were used. For wider root canals of this group (distal canal of mandibular molars and palatal canal of maxillary molars), the BR6 (#50/0.04) and BR7 (#60/0.02) instruments were also used. The root canals were shaped at a rotational speed of 500 rpm (X-Smart, Dentsply, Ballaigues, Switzerland) and 1.5 Ncm torque. Two sets of instruments were used, and the time required for each preparation was recorded using a digital stopwatch.
During preparations, the canals were irrigated between instruments with 3 mL of a recently prepared 1% NaOCl using a syringe with a 30-gauge needle (Injecta, Diadema, Brazil). Root canals were dried and filled with 17% EDTA (pH 7.2; Biodinâmica, Ibiporã, Brazil) for 3 min to remove the smear layer. Another 3 mL of 1% sodium hypochlorite solution was used for irrigation. Periapical radiographs and CBCT images were then taken.
Root canal filling
The root canals were filled with gutta-percha and AH Plus sealer (Dentsply, Ballaigues, Switzerland) using the conventional lateral condensation technique. The sealer was prepared according to manufacturer’s directions. After obturation, new periapical radiographs and CBCT images were taken under the same conditions described previously.
Image evaluation
Two examiners (a radiologist and an endodontist) were calibrated using 20% of the specimens, and all images were evaluated to detect the presence or absence of fractured instruments, root perforations (coronal, middle or apical third) and deviations from the original trajectory of the root canal (apical transportation). Instrument fractures during preparation were also detected. When a consensus was not reached by the two examiners that interpreted the procedural errors using the images, a third observer (an endodontist) made the final decision.
Statistical Analysis
The agreement between examiners was analyzed using kappa statistics. The differences between types of procedural errors according to periapical radiographs and CBCT images were analyzed using the Kolmogorov-Smirnov test. The association of periapical radiographs and CBCT images with types of procedural errors was evaluated using the Fisher exact test. The differences of mean time for root canal preparation between the three groups were assessed using ANOVA, and the comparison of means, using the Tukey test. The level of significance was set at 5%.
Results
The results of kappa statistics (κ=0.889) revealed that agreement was significant (P<0.001).The frequency of procedural errors detected using periapical radiographs and CBCT images and the mean time of root canal preparation according to instrument used are described in Tables 1-3. In a total of 180 root canals prepared (maxillary and mandibular molars), 11 (6.11%) procedural errors were detected using periapical radiographs (7 [3.88%] fractures and 4 [2.23%] canal transportations). CBCT also detected 11 (6.11%) procedural errors (7 [3.88%] fractures, 3 [1.67%] canal transportations and 1 [0.56%] perforation).
Table 1. Frequency of procedural errors in canals detected using periapical radiographs and CBCT (Kolmogorov-Smirnov test).
| Method | n | Fracture | Canal Transportation | Perforation | P-value |
|---|---|---|---|---|---|
| Periapical radiograph | 180 | 7 (3.88%) | 4 (2.23%) | 0 (0.00%) | P>0.05 |
| CBCT a | 180 | 7 (3.88%) | 3 (1.67%) | 1 (0.56%) | P>0.05 |
a. Cone beam computed tomography
The analysis of types of procedural errors, instruments and diagnostic imaging methods revealed no significant differences (P>0.05). The analysis of time to prepare root canals using different instrumentation systems revealed significant differences between K-Flexofile and K3 (P=0.002), K-Flexofile and BioRace (P<0.001) and K3 and BioRace (P=0.003).
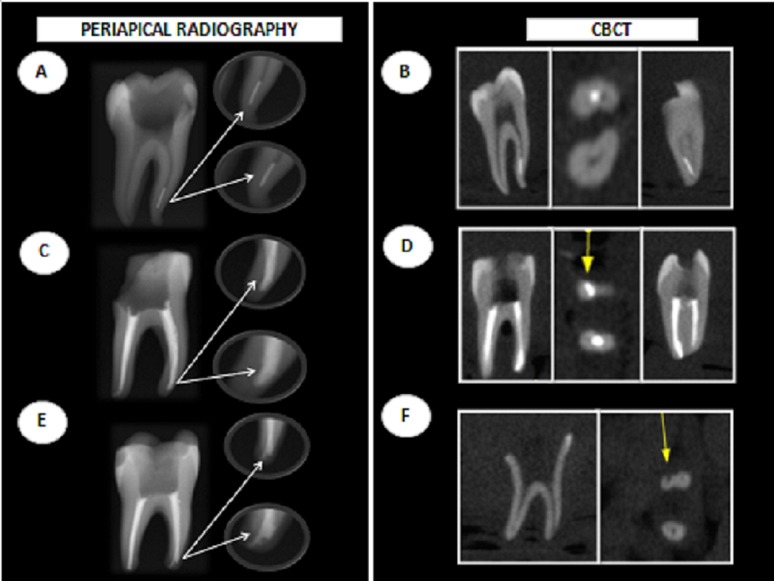
Figure 1 illustrates cases of instrument fracture, canal transportation and perforation detected using periapical radiography and CBCT.
Figure 1. Procedural errors detected using periapical radiographs and CBCT images: instrument fracture (A, B), canal transportation (C, E, D) and perforation (F).
Discussion
Probable procedural errors affecting treatment prognosis should be considered and evaluated before choosing a new endodontic instruments to be used. This study found no significant difference in the ability of different imaging techniques in diagnosis of procedural errors, either the occurrence of procedural errors using different canal preparation techniques. [3, 4, 9-11, 13, 26-29].
A total Of 180 root canals were prepared in this study and 11 (6.11%) procedural errors were detected using periapical radiography and CBCT. The quality of the preparation of curved root canals has been assessed using different methods on extracted teeth, such as tooth clearing[30], radiography [3, 8, 9], microcomputed tomography (µ-CT) [9, 21, 28] and CBCT [3, 17, 23] or by using simulated canals [10, 27, 31]. The unpredictability of internal dental anatomy is a great challenge in the preparation of the whole root canal system [31], and studies about noninvasive diagnostic methods should be conducted to detect procedural errors, which are risk factors for endodontic failures [3].
Rather resolution of CBCT images and three-dimensional imaging techniques have contributed to the analysis of the internal morphology and are important resources to assess the shape of the root canal before and after preparation [3, 9, 16, 21, 23, 28]. Peters et al. [28] evaluated the potential and accuracy of a three-dimensional in vitro technique (µ-CT) to describe the geometry of root canals using extracted human molars. They accurately determined the internal anatomy of canals using this innovative technique, and their variables and indices may serve as a basis for studies of root canal anatomy, but this imaging method is not used in clinical situations due to high lethal amount of exposure.
CBCT must be carefully used, especially considering its appropriate indication and method of analysis [15]. Metal artifacts and filling materials may interfere with CBCT images, and, therefore, a periapical radiograph should be obtained in advance for simultaneous analysis with CBCT. Precautions must be taken to deal with the effect of solid materials in the interior space of root canals on CBCT images [15]. To minimize this effect, CBCT images were taken at three time points in this study: before and after instrumentation and after root canal filling. In this study the perforations were detected at the second time point, which ruled out the possibility of a false negative data due to an artifact because the tooth had not been filled yet. Periapical radiographs were also taken at three time points because, within the limitations of this type of imaging, canal transportation is best viewed when the root canals are filled.
The instruments used in this study were stainless steel K-Flexofiles for hand use, the K3 NiTi rotary system and BioRace. The samples were carefully selected and comprised teeth with moderate canal curvatures in at least one of the mesial roots of mandibular molars and buccal roots of maxillary molars (4<r≤8 mm). The occurrence of procedural errors was low regardless of type of instrument used. The results of this study confirm the low frequency of procedural errors during root canal preparation using NiTi instruments [3, 9, 12].
The frequency of errors according to instrument used was not significant. The analysis of type of error revealed that no fracture occurred with the use of stainless steel K-Flexofiles (Tables 1 and 2). The main procedural error detected when using this type of instrument was canal transportation, which may be explained by the fact that stainless steel instruments do not have characteristics of superelasticity or shape-memory effect and tend to straighten the canal. Because of that, operators should pre-curve the file manually and file the root canal walls with short length movements, a technique that is difficult to standardize and this fact favors the occurrence of canal transportation.
Oliveira et al. used CBCT to evaluate apical transportation after root canal preparation using different automated systems (K-Flexofile, Nitiflex, K3 and Race) [23]. Centralizing ability and apical transportation were not influenced by mechanical motion or type of instrument used. Hartmann et al. [21] used computed tomography (CT) to compare transportation in the mesiobuccal canals of maxillary molars prepared using different techniques: manual instrumentation with K-Flexofile, K-Flexofile attached to an oscillatory system and ProTaper rotary system. All techniques caused root canal transportation and the oscillatory technique had the greatest reduction from the dentinal walls of inner curvature. Alencar et al. [3] compared students in their final undergraduate year and endodontists with over five years of experience to evaluate the occurrence of procedural errors (fracture, perforation and canal transportation) using the ProTaper Universal and found that both undergraduate students and dentists used rotary NiTi instruments successfully and achieved low rates of procedural errors.
The instrument fractures detected in this study occurred with the use of rotary NiTi instruments, with no significant differences between groups (Table 2). The fracture of NiTi instruments may be associated with the following factors: knowledge, experience, technique, design characteristics and surface treatment [13]. Lopes et al. evaluated the effect of electro-polishing as a surface treatment on the number of cycles to fracture when using a BioRace instrument (# BR5C) [31]. They concluded that the number of cycles to instrument fracture after electrolyte treatment was 124% higher than the instruments without receiving any surface treatment.
Table 2. Frequency of procedural errors in canals detected using periapical radiographs and CBCT images (according to instrument).
| Method | n | K-Flexofile | K3 | BioRace | P-value |
|---|---|---|---|---|---|
| Periapical radiograph | 180 | 3 (27.27%) | 3 (27.27%) | 5 (45.45%) | P>0.05 |
| CBCT a | 180 | 3 (27.27%) | 3 (27.27%) | 5 (45.45%) | P>0.05 |
a. Cone beam computed tomography
In this study, mean preparation time was recorded, and results were significantly different between the three groups (Table 3). The lowest mean preparation time belonged to NiTi instruments, that can be justified by the automation of rotary systems, which favors a faster canal preparation. Tu et al. [28] prepared 46 simulated curved canals in resin blocks using manual and automated instrumentation with the ProTaper system and found that the learning curve for students is lower for the rotary system than for the manual system.
Table 3. Mean time of root canal preparation in minutes per tooth according to instrument (ANOVA, Tukey test) .
| Mean time (SD) | K-Flexofile | K3 | BioRace | P-value |
|---|---|---|---|---|
| Students | 43 (15) | 30 (11) | 17 (6) | P<0.001 |
Devotion of extra time for preparation of curved canals using NiTi rotary systems may represent a greater risk of fracture. Mesgouez et al. determined the influence of operator experience (with and without previous knowledge) at the time of preparation of simulated curved canals using the Profile system [10]. Mean preparation time for all specimens was 2 minutes and 42 seconds per canal. The time required for preparation of the root canal was found inversely proportional to the operator's experience. Sonntag et al. [13] stated that operators with little experience performed better root canal preparation when using NiTi rotary instruments compared to stainless steel instruments, although more fractures occurred. Students prepared curved canals at least 2.5 minutes faster, provided that they had preliminary experience with a hand preparation technique.
Gekelman et al. evaluated the canals prepared by inexperienced clinicians who had received training sessions [9]. Computer software was used to analyze the canals and assess changes (volume, surface, shape, and transportation) during preparation. The results showed no significant differences between the instruments or operators in relation to variations in the center of mass; qualitative and quantitative data of canal transportation were similar for inexperienced students and experienced operators. Both systems were satisfactory when operated by inexperienced students who received a brief training session.
Dental schools worldwide have assessed the use of rotary NiTi instruments for curved canal preparation [3, 5, 9, 11, 13, 29]. Further research should investigate new concepts and technologies that raise opportunities for discussion, reflection and changes in the scientific world.
Conclusion
The frequency of procedural errors (fracture, canal transportation and perforation) during the preparation of canals of maxillary and mandibular molars using stainless steel and NiTi instruments was low regardless of diagnostic imaging method when used by inexperienced operators.
Acknowledgments
The authors deny any conflicts of interest related to this study. This study was supported in part by grants from the National Council for Scientific and Technological Development (CNPq grants 306394/2011-1 to C.E.).
Footnotes
Please cite this paper as:
Alvesa RAA, Souzaa JB, Gonçalves Alencara AH, Pécoraa JD, Estrela C. Detection of Procedural Errors with Stainless Steel and NiTi Instruments by Undergraduate Students Using Conventional Radiograph and Cone Beam Computed Tomography. Iran Endod J. 2013;8(4):161-5.
References
- 1.Thompson SA. An overview of nickel–titanium alloys used in dentistry. Int Endod J. 2000;33(4):297–310. doi: 10.1046/j.1365-2591.2000.00339.x. [DOI] [PubMed] [Google Scholar]
- 2.Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of Nitinol root canal files. J Endod. 1988;14(7):346–51. doi: 10.1016/s0099-2399(88)80196-1. [DOI] [PubMed] [Google Scholar]
- 3.Alencar AHG, Dummer PMH, Oliveira HCM, Pécora JD, Estrela C. Procedural errors during root canal preparation using rotary NiTi instruments detected by periapical radiography and cone beam computed tomography. Braz Dent J. 2010;21(6):543–9. doi: 10.1590/s0103-64402010000600011. [DOI] [PubMed] [Google Scholar]
- 4.Gao Y, Peters OA, Wu H, Zhou X. An application framework of three-dimensional reconstruction and measurement for endodontic research. J Endod. 2009;35(2):269–74. doi: 10.1016/j.joen.2008.11.011. [DOI] [PubMed] [Google Scholar]
- 5.Pecora JD, Capelli A. Shock of paradigms on the instrumentation of curved root canals. Braz Dent J. 2006;17(1):3–5. doi: 10.1590/s0103-64402006000100001. [DOI] [PubMed] [Google Scholar]
- 6.Wu MK, Barkis D, Roris A, Wesselink PR. Does the first file to bind correspond to the diameter of the canal in the apical region? Int Endod J. 2002;35(3):264–7. doi: 10.1046/j.1365-2591.2002.00474.x. [DOI] [PubMed] [Google Scholar]
- 7.Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18(2):269–96. [PubMed] [Google Scholar]
- 8.Esposito PT, Cunningham CJ. A comparison of canal preparation with nickel-titanium and stainless steel instruments. J Endod. 1995;21(4):173–6. doi: 10.1016/S0099-2399(06)80560-1. [DOI] [PubMed] [Google Scholar]
- 9.Gekelman D, Ramamurthy R, Mirfarsi S, Paque F, Peters OA. Rotary nickel-titanium GT and ProTaper files for root canal shaping by novice operators: a radiographic and micro-computed tomography evaluation. J Endod. 2009;35(11):1584–8. doi: 10.1016/j.joen.2009.07.018. [DOI] [PubMed] [Google Scholar]
- 10.Mesgouez C, Rilliard F, Matossian L, Nassiri K, Mandel E. Influence of operator experience on canal preparation time when using the rotary Ni-Ti ProFile system in simulated curved canals. Int Endod J. 2003;36(3):161–5. doi: 10.1046/j.1365-2591.2003.00625.x. [DOI] [PubMed] [Google Scholar]
- 11.Hanni S, Schonenberger K, Peters OA, Barbakow F. Teaching an engine-driven preparation technique to undergraduates: initial observations. Int Endod J. 2003;36(7):476–82. doi: 10.1046/j.1365-2591.2003.00677.x. [DOI] [PubMed] [Google Scholar]
- 12.Pettiette MT, Delano EO, Trope M. Evaluation of success rate of endodontic treatment performed by students with stainless-steel K-files and nickel-titanium hand files. J Endod. 2001;27(2):124–7. doi: 10.1097/00004770-200102000-00017. [DOI] [PubMed] [Google Scholar]
- 13.Sonntag D, Delschen S, Stachniss V. Root-canal shaping with manual and rotary Ni-Ti files performed by students. Int Endod J. 2003;36(11):715–23. doi: 10.1046/j.1365-2591.2003.00703.x. [DOI] [PubMed] [Google Scholar]
- 14.Spangberg L. The wonderful world of rotary root canal preparation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92(5):479. doi: 10.1067/moe.2001.120438. [DOI] [PubMed] [Google Scholar]
- 15.Bueno MR, Estrela C, De Figueiredo JAP, Azevedo BC. Map-reading strategy to diagnose root perforations near metallic intracanal posts by using cone beam computed tomography. J Endod. 2011;37(1):85–90. doi: 10.1016/j.joen.2010.08.006. [DOI] [PubMed] [Google Scholar]
- 16.Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod. 2007;33(9):1121–32. doi: 10.1016/j.joen.2007.06.011. [DOI] [PubMed] [Google Scholar]
- 17.Estrela C, Bueno MR, De Alencar AHG, Mattar R, Valladares Neto J, Azevedo BC, et al. Method to evaluate inflammatory root resorption by using cone beam computed tomography. J Endod. 2009;35(11):1491–7. doi: 10.1016/j.joen.2009.08.009. [DOI] [PubMed] [Google Scholar]
- 18.Estrela C, Bueno MR, Sousa-Neto MD, Pécora JD. Method for determination of root curvature radius using cone-beam computed tomography images. Braz Dent J. 2008;19(2):114–8. doi: 10.1590/s0103-64402008000200005. [DOI] [PubMed] [Google Scholar]
- 19.Estrela C, Bueno MR, Azevedo BC, Azevedo JR, Pecora JD. A new periapical index based on cone beam computed tomography. J Endod. 2008;34(11):1325–31. doi: 10.1016/j.joen.2008.08.013. [DOI] [PubMed] [Google Scholar]
- 20.Estrela C, Bueno MR, Leles CR, Azevedo B, Azevedo JR. Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod. 2008;34(3):273–9. doi: 10.1016/j.joen.2007.11.023. [DOI] [PubMed] [Google Scholar]
- 21.Hartmann MSM, Fontanella VRC, Vanni JR, Fornari VJ, Barletta FB. CT evaluation of apical canal transportation associated with stainless steel hand files, oscillatory technique and ProTaper rotary system. Braz Dent J. 2011;22:288–93. doi: 10.1590/s0103-64402011000400005. [DOI] [PubMed] [Google Scholar]
- 22.Lofthag-Hansen S, Huumonen S, Grondahl K, Grondahl HG. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(1):114–9. doi: 10.1016/j.tripleo.2006.01.001. [DOI] [PubMed] [Google Scholar]
- 23.Oliveira CA, Meurer MI, Pascoalato C, Silva SR. Cone-beam computed tomography analysis of the apical third of curved roots after mechanical preparation with different automated systems. Braz Dent J. 2009;20(5):376–81. doi: 10.1590/s0103-64402009000500004. [DOI] [PubMed] [Google Scholar]
- 24.Venkateshbabu N, Emmanuel S, Santosh G, Kandaswamy D. Comparison of the canal centring ability of K3, liberator and EZ Fill safesiders by using spiral computed tomography. Aust Endod J. 2009;35:1–5. doi: 10.1111/j.1747-4477.2009.00210.x. [DOI] [PubMed] [Google Scholar]
- 25.Estrela C. A Critical Review of Efficacy of Nickel-Titanium Instruments in Shaping Curved Root Canals. In: Sydney GB, Estrela C, editors. Endodontic Science, 2th Edition. São Paulo: Artes Médicas; 2009. pp. 659–83. [Google Scholar]
- 26.Aguiar CM, De Andrade Mendes D, Câmara AC, De Figueiredo JAP. Evaluation of the centreing ability of the ProTaper Universal™ rotary system in curved roots in comparison to Nitiflex™ files. Aust Endod J. 2009;35(3):174–9. doi: 10.1111/j.1747-4477.2009.00168.x. [DOI] [PubMed] [Google Scholar]
- 27.Bryant ST, Dummer PM, Pitoni C, Bourba M, Moghal S. Shaping ability of .04 and .06 taper ProFile rotary nickel-titanium instruments in simulated root canals. Int Endod J. 1999;32(3):155–64. doi: 10.1046/j.1365-2591.1999.00256.x. [DOI] [PubMed] [Google Scholar]
- 28.Peters OA, Laib A, Ruegsegger P, Barbakow F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res. 2000;79(6):1405–9. doi: 10.1177/00220345000790060901. [DOI] [PubMed] [Google Scholar]
- 29.Tu MG, Chen SY, Huang HL, Tsai CC. Endodontic Shaping Performance Using Nickel–Titanium Hand and Motor ProTaper Systems by Novice Dental Students. J Form Med Assoc. 2008;107(5):381–8. doi: 10.1016/S0929-6646(08)60103-5. [DOI] [PubMed] [Google Scholar]
- 30.Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10(1):3–29. [Google Scholar]
- 31.Lopes HP, Elias CN, Vieira VT, Moreira EJ, Marques RV, de Oliveira JC, et al. Effects of electropolishing surface treatment on the cyclic fatigue resistance of BioRace nickel-titanium rotary instruments. J Endod. 2010;36(10):1653–7. doi: 10.1016/j.joen.2010.06.026. [DOI] [PubMed] [Google Scholar]