

Abstract
The purpose of the study was to describe the magnitude of the selected sports medicine problems (i.e. cauliflower ear and skin infections) among wrestlers in Tehran. A number of 411 wrestlers were randomly selected from wrestling clubs in Tehran employing cluster sample setting method. The participants were interviewed using a specially designed and validated questionnaire. Nearly half of the participants (44%) had “cauliflower ears”. Only 23% of these participants had received any kind of treatment for their acute ear haematomas that are known to result in “cauliflower ears”. The prevalence of reported hearing loss among participants with cauliflower ears (11.5%, 95%CI: 6.9 to 16.2) was significantly more than this prevalence among those participants without cauliflower ears (1.8%, 95%CI: 0.1 to 3.5) (p < 0.05). More than half of the participants (52%) had skin infection diagnosed by a physician during the previous year. This study has identified evidence of an increase in hearing loss as a possible side effect of either cauliflower ear or ear injury in wrestling in Iran. There has been an outbreak of ringworm and there is a significant potential for an outbreak of impetigo among wrestlers in Tehran.
Key points.
Skin infections are prevalent among wrestlers in Tehran.
Commonly wrestlers in Tehran continue to carry out wrestling training while affected by skin infections.
Cauliflower ear ”is common among wrestlers in Tehran.
More research is needed to investigate hearing loss as a possible side effect of either cauliflower ear or ear injury in wrestling in Iran.
Key words: Wrestling, cauliflower ears, skin infections
Introduction
Wrestling is the national sport of Iran and it remains quite popular in this country. According to the National Wrestling Federation of Iran 232068 wrestlers were training wrestling in Iran in 2005 (NFSMI, 2005). Injury and disease preventive plans are essential to improve health of wrestlers in Iran. In order to develop effective sports medicine preventive plans the magnitude, scope, and characteristics of the health problems in this group of athletes must be investigated. Such information will identify the extent of the current health problems, and where preventative actions are needed (Holder et al., 2001, WHO, 2003).
To our knowledge, there is no published data on the health problems of wrestlers in Iran. In addition, data on health problems of wrestlers in other countries, except the United States of America, are scarce. Investigation of sports medicine problems of wrestlers in Iran could be beneficial for the prevention of these problems among wrestlers both in Iran and internationally.
A review of the literature has suggested that skin infection has been a major health problem among wrestlers in the US which can cause a significant disruption of sporting activity in this group of athletes (Adams, 2000; 2002; Lillegard et al., 1997; NCAA, 2003). Anecdotal data in Iran suggest that cauliflower ear is common among wrestlers in Iran and it can cause hearing loss. Therefore, we focused on skin infection and cauliflower ear as possible health problems of wrestlers in Iran in this study.
Cauliflower ear (wrestler’s ear)
The outer ear (pinna) is composed mainly of cartilage covered by perichondrium, subcutaneous tissue, and skin. Direct trauma or continues friction to the outer ear can cause acute haematomata within the potential space between perichondrium and the cartilage in the pinna. Separation of the perichondrium from the cartilage can lead to necrosis of the cartilage because of the consequential loss of blood supply. Cartilage necrosis and fibroneocartilage formation in the region results in deformity of the pinna and may result in the loss of cartilaginous support for the shape of the pinna resulting in a “cauliflower ear ”or “wrestler’s ear ”deformity (Figure 1). Cauliflower ears are reported in athletes practicing contact sports such as boxing, wrestling, rugby, and judo (Yotsuyanagi et al. , 2002). Prompt and proper treatment of this injury should reduce the likelihood of severe deformity and a permanent cosmetic malformation (Jones and Mahendran, 2004).
Figure 1.
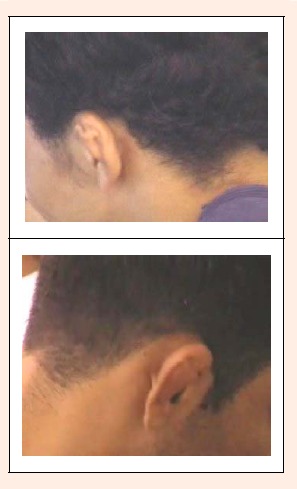
"Cauliflower ear ”or “wrestler’s ear”.
It is reported that 39% of high school wrestlers in US had a cauliflower ear (Schuller et al., 1989). According to the high school and collegiate wrestling rules in the USA, “a protective ear guard must be worn anytime wrestling takes place ”(this includes both practice and competitions) (NCAA, 2005). Headgear may provide partial protection for ear injuries (Schuller et al., 1989). According to the international wrestling regulation, ear protectors are not obligatory for wrestlers except for cadet and junior women wrestlers (FILA, 2005). In Iran, wrestlers do not wear ear protectors.
Wrestling has been a symbol of power and virility for the people in a number of countries such as Iran (FILA, 2003). Therefore, wrestlers refuse to treat their ear haematoma in order to develop a cauliflower ear (Reid, 1992). Cauliflower ear should be common among wrestlers in the Asian countries such as Iran not only because the wrestlers in these regions do not wear ear protectors but also because some wresters might refuse to have their ear haematoma treated. To our knowledge, there is no published data on the prevalence of cauliflower ear in these regions.
The cosmetic problem has been mentioned as the main concern of cauliflower ear in the literature (Jones and Mahendran, 2004). Our interview with some Iranian wrestling experts suggested that wrestlers and coaches in Iran believe that cauliflower ear may lead to some degree of hearing loss. We could not find any studies on possible hearing loss associated with cauliflower ear in the literature.
Skin infections in wrestling
Opponents in wrestling have prolonged close body contact during wrestling when skin infections may be transmitted from the infected wrestler to the opponent. It is suggested that skin infection is a major health problem in wrestling in the US (Beck, 2000, Mysnyk, 2001). Tinea corporis (tinea gladiatorum) and herpes simplex virus (HSV) infection (herpes gladiatorum) are common wrestling skin infections. Both of these infections are predominantly transmitted as a result of skin-to-skin contact (Belongia et al., 1991; Landry and Chang, 2004). Some case reports of outbreaks of herpes simplex and tinea corporis have been published in the literature, mainly in small groups of wrestlers (Belongia et al., 1991; El Fari et al., 2000; Kohl and Lisney, 2000).
According to the National Collegiate Athletic Association Injury Surveillance System of the US (NCAA), skin infections were responsible for 10 to 31% of time loss from wrestling. Data from this surveillance system showed that skin infection was the first or the second most common injury in recent years in the US (Jarret et al., 1998; NCAA, 2003). Based on the NCAA injury surveillance system, the skin infections reported from 1991 to 2003 in wrestlers were herpes (39%), tinea corporis ( 23%), impetigo (14%), Scabies (0.5%), and other infections (23.5%) (Landry and Chang, 2004).
The National Athletic Trainers’ Association (NATA) performed a three-year injury surveillance study on high school athletes from 1995 to 1997. The data from this study showed that one in four high school wrestling teams were affected by at least one kind of skin condition, most commonly ringworm. In 1995, skin disorders accounted for 11.4% of injuries to high school wrestlers and were the third most common injury. Skin disorders included ringworm (83.8%), impetigo (6.8%), dermatitis (3.4%) herpes zoster (1.7%) and other skin infections (3.4%) (NATA, 2003).
Pasque and Hewett, 2000 performed a prospective survey on 458 male high school wrestlers during one season. About 5% of wrestlers during that year had skin infections. The average time lost from wrestling was 5 days (range- 2 to 19 days). Impetigo was the most common skin conditions.
Kohl et al., 2002 carried out a retrospective mail survey on wrestlers from 540 high schools to assess the prevalence of ringworm in a larger population during the 1998-1999 season. The athletic trainers and/or athletic directors and/or wrestling coaches of the schools responded to this mail survey. The result showed that at least one wrestler was infected with ringworm in 85% of the teams; at least one wrestler was infected with impetigo in 42%, and infected with herpes in 11% of the teams. In two teams (0.9% of the responders) more than 15 wrestlers were infected by ringworm during the season, but the majority of teams (62%) had between 1 and 5 cases. Ringworm mainly caused only 1 to 4 missed practice session in infected wrestlers. About one-third of teams had at least one wrestler who missed a match because of ringworm. To our knowledge, there is no published data on skin infections among wrestlers in Iran.
The objective of this study was to describe the magnitude of skin infections and cauliflower ear among wrestlers in Tehran.
Methods
This study was a population-based cross sectional survey. The target population was the general populations of wrestlers in Tehran i.e. wrestlers who were members of wrestling clubs in Tehran and had experience of at least one year of wrestling training. Wrestlers (n = 411) were randomly selected from wrestling clubs in Tehran employing cluster sample setting method. Tehran was divided into four zones based on geography and socio-cultural parameters. Wrestling training was conducted in 95 wrestling clubs in Tehran in 2005. We randomly selected 30% of the clubs in each region and selected about 15% of the population of each club. In total 411 wrestlers randomly selected from 28 clubs in Tehran.
The participants were interviewed using a specially designed and validated questionnaire (Kordi et al., 2005).
Results
Participants
The majority (97%) of the wrestler’s participants practiced Free-style and 3% of them practiced Greco-Roman style. The age, weight, height and year of wrestling training of the participants are listed in the Table 1.
Table 1.
The age, weight, height, and year of wrestling training of the subjects (n = 411). Data are means (±SD) [minimum-maximum].
| Age (year) | 19.1 (4.0) [11-42] |
| Weight( kg) | 69.0 (15.7) [30-126] |
| Height (m) | 1.72 (.10) [1.30-1.92] |
| Year of wrestling training | 4.0 (3.4) [1-24] |
The participants had an average of 3.0 ± 1.5 training sessions per week (range: 1 to 12). They trained for a mean of 2.0 ± 0.46 hours per training session (range: 1 to 4.5).
Cauliflower ear
Of all the participants, 44% (95%CI =39% to 50%) had a “cauliflower ear”, (25% in one ear and 19% in both ears). Only 23% of these participants had received any kind of treatment for their cauliflower ear. Of those participants who had a cauliflower ear, 11.5% (95%CI = 6.9% to 16.2%) reported that they felt they suffered from hearing loss. Of the participant who had no cauliflower ear 1.8% (95%CI = 0.1% to 3.5%) reported that they felt they suffered from hearing loss. The differences between these groups were statically significant (p < 0.05).
Of those who had two cauliflower ears, 11.4% reported hearing loss and of those who had one cauliflower ear, 11.6% reported hearing loss.
Twenty- five percent of those participants who received treatment for their cauliflower ear reported a hearing loss (95%CI = 11.6% to 36.7%). Only 7.7% of those who did not receive treatment reported a hearing loss (95%CI = 3.4% to 11.1%). The differences between these groups were statistically significant (p < 0.05). Nearly half (48%) of the participants with a cauliflower ear who reported a hearing loss had been treated by a physician for their cauliflower ears.
The percentage of reported hearing loss among those who had one cauliflower ear (11.6%) was similar to those who had two cauliflower ears (11.4%).
Skin infection
More than half (52%) of the participants had skin infection diagnosed by a physician during the previous year (95%CI = 47% to 57%). The most common skin infection was ringworm that infected 47.4% of all the participants. Ringworm was reported by 22% to 100% of the participants from all the 28 clubs. In the same period a small percentage of participants (3.2%) suffered from herpes gladiator. Also 1.2% of participants suffered from impetigo and 0.2% sustained scabies during the previous year. Scabies was reported from one club, herpes gladiatorum from 10 clubs and impetigo from three clubs. In one club, 20% of participants were infected by impetigo.
Of the participants who had skin infections, only 39% did miss training sessions because of their skin infections.
Discussion
Cauliflower ear or wrestler’s ear
The results of this study have shown that “cauliflower ear ”is common among wrestlers in Tehran. In addition, the data suggests that the majority of those who had cauliflower ear (77%) have not received any treatment. This is probably because a severe cauliflower ear is recognized as a “badge of courage ”in Iran. Therefore, wrestlers refuse to have their ear haematomata treated.
The Ministry of Health and Medical Education of Iran (MHME, 1992) conducted a survey of health and disease in the general population of Iran. This involved sampling 1/1000 of the population from all parts of the country. Data were collected over a period of one year (November 1990-November 1991). The results of this survey in relation to hearing loss in the general population of Tehran are shown in Table 2.
Table 2.
Hearing loss in the population of Tehran based on the Survey of Health and Disease in the Islamic Republic of Iran (MHME, 1992).
*i.e. Those who reported hearing loss, but were not deaf and did not use hearing aids, based on a questionnaire survey (self reported hearing loss).
**Those who used hearing aids = 1.1%, Deaf in one ear = 0.2%, Deaf in both ears = 0.1%.
The percentage of those who had hearing loss but were not deaf and did not used hearing aids reported by MHME (1992) in 15 to 39 years old people in Tehran (3.2%) was lower than the percentage of those who reported hearing loss in our participants with cauliflower ear, (11.5%, 95%CI = 6.9 to 16.2) but was in the range of 95% of confidence interval of this rate in our participants without cauliflower ear (1.8%, 95%CI = 0.1 to 3.5). As shown in Table 2 the rate of hearing loss increased with age. The majority (95%) of the participants in this study were less than 25 years old. Therefore, based on this limited data there is no evidence that the percentage of hearing loss in wrestlers without cauliflower ears in Tehran is different from this rate in the general population in the same age in Tehran.
Based on the survey of “Health and disease in the general population of Iran ”0.9% of 15 to 35 years old men in Tehran province had a pinna with an abnormal appearance. The cause of these abnormalities was not investigated or reported (MHME, 1992). However, wrestling is likely to have been an important cause of these abnormalities.
To our knowledge, there is no published data on the side effects of cauliflower ear in wrestlers. However, the main problem associated with a cauliflower ear is believed to be cosmetic (Naftulin and Mckeag, 1999).
The higher prevalence of hearing loss among wrestlers who had cauliflower ears in this study might be because of two main reasons:
-
Hearing loss associated with the cauliflower ear deformity: The external ear consists of the pinna (auricle) and the external auditory canal. Its function is thought to be mainly protective, although its physical configuration may provide moderate passive augmentation of sounds (Yueh et al., 2003, Ballachanda, 1997). Complete occlusion of the ear canal dose cause conductive hearing loss (Isaacson and Vora, 2003). In some severe cauliflower ear cases, the deformity does extend to the external auditory canal (Yotsuyanagi et al., 2002) which might lead to obstruction in the external ear and cause hearing loss. Also cauliflower ear may cause functional complications, such as disruption of the normal mechanism of wax transport from the ear canal, and an increased risk of otitis externa (Macdonald et al., 2005).
These complications might subsequently lead to hearing loss. Of the 15 to 35 years old men in Tehran province 1.4% had a perforated tympanic membrane and 1.4% had an infected discharge from their ears (MHME, 1992). These complications might have important roles in hearing loss in wrestlers in Tehran and require further investigation.
Hearing loss associated with injury to a deeper part of the ear: Direct trauma to the external ear that causes an ear haematoma may cause hearing loss due to associated trauma to the middle or inner ear. Stiernberg and Strunk, 1986 have claimed that ear injuries that cause hearing loss are more common among wrestlers and boxers.
Nearly half of the participants who reported hearing loss in this study (48%) had been treated by a physician for their “ear haematoma”. The participants who had received treatment for their ear haematomata had reported significantly more hearing loss than those participants who had untreated cauliflower ear (p < 0.05). It could be hypothesised that participants with a cauliflower ear who sought medical treatment were those who had more severe injuries that either caused more serious ear haematomata or caused injury to other parts of the ear that encouraged the wrestlers to visit a physician.
The percentage of reported hearing loss among those who had one cauliflower ear was similar to those who had two cauliflower ears. This reduces the likelihood that it was the physical deformity of the cauliflower ear alone that was the cause of the reported hearing losses.
Anecdotal data suggests that it is a common belief among Iranian wrestlers that “cauliflower ear can cause hearing loss”. This might have influenced the answer given by our wrestlers. To reduce the effect of this perception, we put three possible answers to the question “Do you have hearing loss? ”- “Yes, ”“No ”and “Not sure ”and treated “Not sure ”as “No ”in our analysis.
It has been shown that a single question about hearing difficulty has high sensitivity for detecting significant hearing loss in the elderly (Patterson, 1997). Niskar, et al. (1998) studied the prevalence of hearing loss among children 6 to 19 years of age in the third National Health and Nutrition Examination Survey in the US. They reported that of children who were suspected of having hearing loss (3.4%), almost half had their hearing loss confirmed by audiometric examination. However, of children who were reported to have normal hearing, only 13.8% had measured hearing loss at the time of audiometric testing. Therefore, it is more likely that those who reported hearing loss would have an impaired audiometric test. Therefore, more research is needed to show if wrestlers who reported hearing loss actually have impaired audiometry tests or not. In addition, more research is needed to show if the reported hearing loss is because of the physical deformity of the cauliflower ear or an undiagnosed injury to the middle or inner ear. As an example a case control study on those wrestlers who have one cauliflower ear, could be designed employing audiological testing. The case group should be the ears with cauliflower ear and the control group could be the ears without cauliflower ear. This study could also have a second control group of wrestlers who have no cauliflower ear.
Ear guards are useful in protecting against the formation of auricular haematoma (Naftulin and Mckeag, 1999). Cosmetic problems alone may not justify the mandatory use of headgear by wrestlers. However, the results of this study bring a real concern about possible side effect of ear injury in wrestling that might justify the compulsory use of headgear. More research is needed in this area.
Skin infections
The results of this study suggest that skin infections were quite common among wrestlers in Tehran.
The rates of different skin infections among wrestlers published in studies vary considerably; because they were affected by the outbreaks of these infections at the time of studies. The prevalence of tinea corporis varies between studies from 20% to 77% of the wrestlers (Landry and Chang, 2004, Adams, 2002, Adams, 2000) and prevalence of herpes gladiatorum varies from 2.6 to 40% of wrestlers (Landry and Chang, 2004). Ringworm was reported by about half (47%) of the participants and reported by 22% to 100% of participants from all the 28 sampled clubs. This indicates that there was an outbreak of ringworm in the wrestling clubs in Tehran around the time of our studies.
The percentage of participants who contracted impetigo (diagnosed by a physician) during the previous year was relatively low at 1.2%. However, it is important that in one club, 20% of the participants had been infected by impetigo during the previous year. This suggests that there was a local outbreak of impetigo in that club. Without preventive measures, this limited number of infected wrestlers might spread the infections to other clubs.
According to the NATA (2003) in 1995, ringworm was the most common skin infections among high School wrestlers accounting for (84%) of skin infections. Similarly in our study the most common infection sustained by the participants was ringworm (91%). By contrast, data form the NCAA injury surveillance system (1991 to 2003) showed that herpes was the most common skin infection among college wrestlers (39%) (Landry and Chang, 2004). These differences were probably affected by the outbreaks of theses infections at the time of the studies.
In our study 61% of the participants who had skin infections did not miss training session. In other words, they continued to wrestler while they had skin infections. These wrestlers might spread skin infections amongst the other wrestlers. An important aspect of prevention of skin infections is early detection of the disease and the banning of infected wrestlers from wrestling training to prevent further spread of the disease. Therefore, skin conditions should be detected by health care personnel, wrestlers, and coaches. The infected wrestlers should be prevented from training until they provide a clearance document from their physician. Wrestlers must be educated about the highly contagious nature of skin infections such as herpes gladiatorum and informed that prompt treatment can minimize time off the training. Appropriate cleaning of equipment including mats, and pre-participation physical examination are also effective in the prevention of these infections (NCAA, 2003). A comprehensive skin disease prevention protocol achieved a statistically significant 90% reduction in the number of cases of tinea corporis in a college wrestling team (Hand et al., 1999).
Conclusion
There was an outbreak of ringworm and the potential for an outbreak of impetigo among wrestlers in Tehran. Some guidelines for the prevention of skin infections in wrestlers in Iran should be developed especially for early detection of skin infections, and return to training after infection, as well as appropriate cleaning of equipment including mats.
This study has identified evidence of an increase in hearing loss as a possible side effect of either cauliflower ear or ear injury in wrestling in Iran. More research employing an audiological testing is recommended in this area.
Biographies
Ramin KORDI
Employment
Ass. Prof. Sports and Exercise Medicine Centre, Tehran University of Medical Sciences.
Degree
MD, MSc(Sports Med), PhD
Research interests
Epidemiology in sports medicine.
E-mail: Ramin_kordi@tums.ac.ir
Mohammad Ali MANSOURNAI
Employment
Sports and Exercise Medicine Centre, Tehran University of Medical Sciences.
Degree
MPh, MD
Research interests
Statistics.
E-mail: mansournia_ma@yahoo.com
Roh Allah NOURIAN
Employment
Sports and Exercise Medicine Centre, Tehran University of Medical Sciences.
Degree
MD
Research interests
Asthma.
E-mail: ghanounrn@yahoo.com
W. Angus WALLACE
Employment
Professor of Orthopaedic and Accident Surgery at the University of Nottingham.
Degree
MD, FRCS(Ed & Eng) FRCS(Orth.)
Research interests
Shoulder surgery, sports injuries, osteoporosis, biomechanics and research into passenger safety in aircraft and cars.
E-mail: angus.wallace@rcsed.ac.uk
References
- Adams B. (2002) Dermatologic disorders of the athlete. Sports Medicine 32, 309-321 [DOI] [PubMed] [Google Scholar]
- Adams B. (2000) Transmission of cutaneous infections in athletes. British Journal of Sports Medicine 34, 413-414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ballachanda B.B. (1997) Theoretical and applied external ear acoustics. Journal of American Academy of Audiology 8, 411-420 [PubMed] [Google Scholar]
- Beck C.K. (2000) Infectious diseases in sports. Medicine & Science in Sports & Exercise 32, S431-S438 [DOI] [PubMed] [Google Scholar]
- Belongia E.A., Goodman J.L., Holland E.J., Anders C.W., Homann S.R., Mahanti R.L., Mizener M.W., Erice A., Osterholm M.T. (1991) An outbreak of herpes gladiatorum at a high-school wrestling camp. New England Journal of Medicine 325, 906-910 [DOI] [PubMed] [Google Scholar]
- El Fari F., Graser Y., Presber Tietz H.J. (2000) An epidemic of tinea corporis caused by Trichophyton tonsurans among children (wrestlers) in Germany. Mycoses 43, 191-196 [DOI] [PubMed] [Google Scholar]
- FILA (the International Federation of Associated Wrestling Styles). (2003) Wrestling [online]. The International Federation of Associated Wrestling Styles, Available from URL: http://www.fila-wrestling.com [Accessed 3.9.2003]. [Google Scholar]
- FILA (the International Federation of Associated Wrestling Styles). (2005) International Wrestling Rules [online]. Lausanne: International Federation of Associated Wrestling Styles; Available from URL: http://www.fila-wrestling.com [Accessed 10.10.2005] [Google Scholar]
- Hand JW., Wroble RR. (1999) Prevention of tinea corporis in collegiate wrestlers. Journal of Athletic Training 34, 350-352 [PMC free article] [PubMed] [Google Scholar]
- Holder H., Peden M., Krug E., Lund J., Gururaj O., Kobusingye O. (2001) Injury surveillance guidelines. Word Health Organization and the Centre for Disease Control and Prevention, Geneve [Google Scholar]
- Isaacson J.E., Vora N.M. (2003) Differential diagnosis and treatment of hearing loss. American Family Physician 68, 1125-1132 [PubMed] [Google Scholar]
- Jarret G.J., Orwin J.F., Dick R.W. (1998) Injuries in collegiate wrestling. American Journal of Sports Medicine 26, 674-680 [DOI] [PubMed] [Google Scholar]
- Jones S.E., Mahendran S. (2004) Interventions for acute auricular haematoma. The Cochrane Database of Systematic Reviews Issue 2, Art. No. CD004166. DOI: 10.1002/14651858. CD004166.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kohl T.D., Giesen D.P., Moyer J.J., Lisney M. (2002) Tinea Gladiatorum: Pennsylvania’s experience. Clinical Journal of Sports Medicine 12, 165-171 [DOI] [PubMed] [Google Scholar]
- Kohl T.D., Lisney M. (2000) Tinea gladiatorum: wrestling’s emerging foe. Sports Medicine 29, 439-447 [DOI] [PubMed] [Google Scholar]
- Kordi R., Mansournai M. R., Nourian R.A., Nea K., Wallace W. A. (2005) Development of data collection instruments for evaluation of wrestling injuries and health problems in Iran. Iranian Journal of Public Health Supl. 103 [Google Scholar]
- Landry GL., Chang CJ. (2004) Herpes and tinea in wrestling managing outbreaks, knowing when to disqualify. The Physician and Sportsmedicine (serial online) 32(10). Available from URL: http://www.physsportsmed.com [DOI] [PubMed] [Google Scholar]
- Lillegard W.A., Butcher J.D., Fields K.B. (1997) Dermatologic problems in athletes. Medical problems in athletes. Fields K.B., Fricker P.A.Malden: Blackwell Science; 234-246 [Google Scholar]
- Macdonald D.J.M., Calder N., Perrett G., McGuiness R.G. (2005) Case presentation: a novel way of treating acute cauliflower ear in a professional rugby player. British Journal of Sports Medicine 39, e29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MHME (the Ministry of Health, Medical Education of Iran). (1992) Survey of Health and Disease in the Islamic Republic of Iran. The Ministry of Health and Medical Education of Iran, Tehran [Google Scholar]
- Mysnyk M.C. (2001) Wrestling. Sports injuries: mechanisms, prevention, treatment. Fu F.H., Stone D.A.2nd edition Philadelphia, Pa., London: Lippincott Williams & Wilkins; 818-838 [Google Scholar]
- Naftulin S., Mckeag D. (1999) Protective equipment: baseball, softball, hockey, wrestling, and lacrosse. Sports medicine secrets: questions you will be asked in the office, on the sidelines,in the training room, on examinations. Mellion MB.Philadelphia: Hanley; 110-116 [Google Scholar]
- NATA (The National Athletic Trainers’ Association). (2003) Injury surveillance study. The National Athletic Trainers’ Association; Available from URL: http://www.nata.org[Accessed 19.11.2003] [Google Scholar]
- NCAA (The National Collegiate Athletic Association). (2003) 2003-04 NCAA sports medicine handbook. The National Collegiate Athletic Association; Available from URL:http://www.ncaa.org/library/sports_sciences/sports_med_handbook/[Accessed 18.11.2003] [Google Scholar]
- NCAA (The National Collegiate Athletic Association). (2005) Wrestling, 2005 rules and interpretations. The National Collegiate Athletic Association, Indiana [Google Scholar]
- NFSMI (The National Federation of Sports Medicine of Iran). (2005) National aAthletic insurance reports. The National Federation of Sports Medicine of Iran; Tehran [Google Scholar]
- Niskar A.S., Kieszak S.M., Holmes A., Esteban E., Rubin C., Brody D.J. (1998) Prevalence of hearing loss among children 6 to 19 years of age: the third national health and nutrition examination survey. Journal of the American Medical Association 279, 1071-1075 [DOI] [PubMed] [Google Scholar]
- Pasque C.B., Hewett T.E. (2000) A prospective study of high school wrestling injuries. The American Journal of Sports Medicine 28, 509-515 [DOI] [PubMed] [Google Scholar]
- Patterson C. (1997) Prevention of hearing impairment and disability in the elderly. Canadian task force on preventive health care, Ottawa: Available from URL: www.ctfphc.org[Accessed 2006.3.4] [Google Scholar]
- Reid D.C. (1992) Sports injury assessment and rehabilitation. Churchill Livingstone, New York; Edinburgh [Google Scholar]
- Schuller D.E., Dankle S.K., Martin M., Strauss R.H. (1989) Auricular injury and the use of headgear in wrestlers. Archives of Otolaryngology-Head & Neck Surgery 115, 714-717 [DOI] [PubMed] [Google Scholar]
- Stiernberg C.M., Strunk C.L. (1986) Ear injuries in sports. Texas Medicine 82(7), 32-36 [PubMed] [Google Scholar]
- WHO (World Health Organization). (2003) Department of Injuries and Violence Prevention. World Health Organization, Geneva: Available from URL: http://www.who.int/violence_injury_prevention/en/http://www.who.int/violence_injury_prevention/en/[Accessed 17.11.2003] [Google Scholar]
- Yotsuyanagi T., Yamashita K., Urushidate S., Yokoi K., Sawada Y., Miyazaki S. (2002) Surgical correction of cauliflower ear. British Journal of Plastic Surgery 55, 380-386 [DOI] [PubMed] [Google Scholar]
- Yueh B., Shapiro N., Maclean C. H., Shekelle P.G. (2003) Screening and management of adult hearing loss in primary care: scientific review. Journal of the American Medical Association 289, 1976-1985 [DOI] [PubMed] [Google Scholar]