

Abstract
Background
Smoking is an independent risk factor for coronary heart diseases and it increases all causes of cardiovascular morbidity and mortality.
Aim of the work
To assess the acute effect of cigarette smoking on ventricular diastolic functions (LV and RV) in healthy, young, and slim smokers.
Methods
Thirty volunteers who had recently commenced smoking (less than one year) and who smoked 1–2 cigarettes per day, underwent ECG, 2D and M-mode echocardiography, standard Doppler echocardiography, pulsed TDI (tissue Doppler imaging) on septal and lateral side of mitral annulus and lateral tricuspid annulus. Vp values were measured. The investigator asked them to hold smoking for at least two days after which echocardiographic examination was conducted before smoking one cigarette and the second examination conducted immediately after smoking one cigarette containing at least 0.4 mg of nicotine.
Results
Doppler findings over the mitral valve showed the E wave was significantly reduced from 82.7 ± 10.4 to 74.6 ± 10.4 after smoking; the A wave increased; the E/A ratio was reduced from 1.5 ± 0.3 to 1.2 ± 0.2; the E′ septal significantly decreased (15.3 ± 2.4 vs. 11.2 ± 1.1) after smoking, and the E/E′ ratio increased from 5.5 ± 1.1 to 6.7 ± 1.1. Doppler findings over the tricuspid valve showed the E wave was reduced from 60.6 ± 9.7 to 52.7 ± 9.6; the A wave increased from 42.2 ± 6.5 to 50.1 ± 6.6; and the E/A ratio decreased (1.45 ± 0.25 vs. 1.06 ± 0.19). The E′ significantly decreased from 14.1 ± 1.8 to 10.9 ± 2.4, while the A′ increased (10.2 ± 2.4 vs. 12.7 ± 3.6) after smoking; and the IVRT of the RV was significantly prolonged from 62.9 ± 7.5 to 68.7 ± 7.9 after smoking. The Vp was markedly reduced from 67.8 ± 8 to 55.2 ± 3.5 after smoking. These findings reflected on the LV filling pressure (LVFvp) which increased from 9.8 ± 1.4 to 10.5 ± 1.3 after smoking. All changes were statistically significant at P < 0.001.
Conclusions
Our study reveals that cigarette smoking can result in significant acute alteration in the diastolic functions of both ventricles.
Keywords: Cigarette, Smoking, RV dysfunction, LV dysfunction, Acute effect
Introduction
The clinical importance of diastolic function in normal and abnormal left ventricular (LV) performance has been recognized for many years. Impaired myocardial relaxation is observed during the course of various cardiac pathologies, [1] and is known to be associated with increased mortality rate in the presence of impaired systolic function. Impaired myocardial relaxation is considered an independent risk factor for increased risk of ventricular arrhythmias and sudden cardiac death even in the presence of normal systolic function [2]. Moreover, asymptomatic diastolic dysfunction may be an early marker of an increased risk of symptomatic heart failure [3].
An estimated 1.3 billion people smoke worldwide [4]. Many smokers, even those who smoke more than 40 cigarettes per day, do not consider smoking as harmful [5]. Smoking is an independent major risk factor for coronary heart disease CHD, cerebrovascular disease, and total atherosclerotic cardiovascular disease [6]. The incidence of an MI is increased sixfold in women and threefold in men who smoke at least 20 cigarettes per day compared to subjects who never smoked [7]. Cigarette smoking increases all causes of cardiovascular morbidity and mortality, and among patients with left ventricular dysfunction (left ventricular ejection fraction ⩽35%) [8]. In the last few years, interest regarding the effect of smoking on the cardiac diastolic function has increased, and echocardiographic evidence of diastolic dysfunction has been demonstrated during acute cigarette smoking in patients with coronary artery disease, [9] while other studies in healthy patients have shown conflicting results [10–12]. Few studies have investigated the acute effect of cigarette smoking on right ventricular function, particularly in healthy nonsmokers [13]. Our study aimed to assess the acute effect of cigarette smoking on ventricular diastolic functions (LV and RV) in healthy, slim, and young light smokers.
Methods
Study setting and subjects
The study was conducted in the College of Applied Medical Sciences in collaboration with the King Fahd Teaching Hospital in Dammam from March 2011 to February 2012. Thirty recent smokers of less than two cigarettes per day were recruited in the study after a public advertisement at Dammam University. The initial goal was to include only non-smokers; but because of ethical concerns in asking non-smokers to smoke for the study, we opted to include recent smokers on a maximum of two cigarettes per day. All participants signed an informed consent form. The University Committee for Biological and Medical Ethics approved the study and the study was conducted in compliance with the principles of the Declaration of Helsinki.
Because of their effect on the diastolic function of the heart, individuals with the following characteristics were excluded from the study: obesity (BMI ⩾ 30), alcoholics, those with hypertension, diabetes mellitus, rheumatic heart disease, ischemic heart disease, echocardiographic evidence of LV hypertrophy, systolic dysfunction, wall motion abnormalities, infiltrative diseases or pericardial disease. Smokers under smoking cessation programs or previous heavy smokers were also excluded from the study. All participants were examined at study entry for pulse, temperature, blood pressure, body weight, height, body mass index, random blood sugar, and resting ECG. The investigator asked the participants to hold smoking for at least two days before examination. On the day of study, echocardiographic examination was done before and immediately after smoking one cigarette containing at least 0.4 mg nicotine.
Echocardiographic measurements
Conventional echocardiography
Two dimensional echocardiography was performed in the parasternal long and short axis views and apical two and four chamber views. LV diameters and area were measured according to the criteria provided by the American Society of Echocardiography [14]. LV ejection fraction was estimated according to LV volumes evaluated by biplane method of disks (modified Simpson’s rule).
Conventional Doppler echocardiography
In the apical four chamber view, a 3 mm sample gate was positioned at the tips of the mitral and tricuspid valves. All measurements were made at end expiration. The following pulsed Doppler transmitral and transtricuspid flow velocity parameters were evaluated: peak E, peak A, and E/A ratio, and averaged over three consecutive cardiac cycles [15].
Pulsed wave TDI
Pulsed wave TDI was performed in the apical two and four chamber views. The 2 mm pulsed Doppler sample volume was placed in two regions of the mitral annulus (lateral and septal) and also within the lateral aspect of the tricuspid annulus, ensuring best alignment between wall motion and the ultrasound beam. The following measurements were taken: peak systolic velocity (S′), peak early diastolic (E′), peak late diastolic (A′), and E′/A′ ratio. Further pulsed Doppler and TDI data were combined in the calculation of the E/E′ ratio.
Color M-mode Doppler study
Recordings was obtained by placing the M-mode cursor through the center of the mitral inflow region in the apical four-chamber view as parallel as possible to flow obtained by color Doppler flow imaging and the Doppler color scale was adjusted for aliasing. Vp value was obtained by measuring the slope delineated by first aliasing velocity from the mitral tips toward the apex. LVFvp was calculated according to the formula LVFvp = 5.9(E/Vp) + 2.5 mmHg [16].
Statistical analysis
Individual characteristics in the form of ECG and echocardiographic were presented as mean and standard deviation. Paired t-test was used to compare echocardiographic parameters before and after one cigarette smoked. A P-value of <0.003 was considered to be statistically significant to adjust for multiple comparisons.
Results
Baseline clinical characteristics of study group are shown in Table 1. Our study group consisted of young subjects with a mean age of 21 (SD, 3) years, duration of smoking was 1.3 (SD, 0.6) years and mean number of cigarettes smoked per day was 1.5 (SD, 0.53). Baseline M-mode and two dimensional echocardiographic data are shown in Table 2. Left ventricle (LV) ejection fractions were within normal limits.
Table 1.
Baseline clinical characteristics of study group.
| Parameters | The study group |
|---|---|
| Age mean (SD) | 21 (3) |
| Sex (Male/Female) | 30/0 |
| Systolic blood pressure (mmHg) | 113 ± 6 |
| Diastolic blood pressure (mmHg) | 80 ± 8 |
| Heart rate (bpm) | 83 ± 4 |
| Duration of smoking; mean (SD) | 1.3 (0.6) |
| Number of cigarettes/day, mean (SD) | 1.5 (0.53) |
Table 2.
Baseline M-mode and two dimensional echocardiographic data.
| Parameters | The study group |
|---|---|
| IVSa | 8.9 ± 0.5 |
| LDEDDb | 46 ± 3 |
| LVESDc | 26 ± 4 |
| Post. walld | 8.7 ± 0.2 |
| LV EFe | 67 ± 7 |
Interventricular septum.
Left ventricular end diastolic dimensions.
Left ventricular end systolic dimensions.
Posterior wall.
Left ventricular ejection function.
Cigarette smoking was found to affect the LV diastolic functions in the form of significant changes in the mitral inflow with tendency towards abnormal relaxation. There were no changes in the LV systolic functions. All changes were statistically significant at <0.001. Fig. 1 presents the percentage of changes of the Doppler parameters in the LV functions from the baseline after a single cigarette was smoked.
Figure 1.
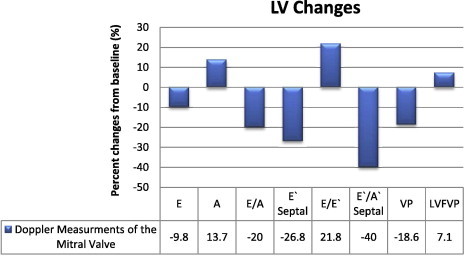
Percent changes in the left ventricular diastolic function parameters from the baseline after single cigarette smoking.
Doppler findings of mitral valve
We observed a significant reduction in trans-mitral early inflow velocity (E wave) after smoking from 82.7 ± 10.4 to 74.6 ± 10.4 with P value < 0.001.
On the other hand, the late inflow velocity (A wave) increased significantly from 54.1 ± 7.8 to 61.5 ± 7.6 after smoking with P value < 0.001, which in turn lead to significant reduction in the E/A ratio from 1.5 ± 0.3 to 1.2 ± 0.2 which is still within normal range but trending towards impaired diastolic filling.
Tissue Doppler findings on the mitral valve
The E′ septal is significantly decreased from 15.3 ± 2.4 to 11.2 ± 1.1 after smoking with P value < 0.001. The A’ increased from 10.7 ± 2.4 before smoking to 13.2 ± 2.6 after smoking with P value < 0.001 which is reflected in E′/A′ septal ratio which also showed significant reduction from 1.5 ± 0.3 before smoking to 0.9 ± 0.2 after smoking with P value < 0.001. E/E′ ratio, which is a predictor of LV filling pressure, significantly increased from 5.5 ± 1.1 before smoking to 6.7 ± 1.1 after smoking. Such changes, despite being within normal range, indicate tendency towards impaired LV relaxation. Fig. 2 shows individual lines presenting the E/E′ ratio changes before and after smoking.
Figure 2.
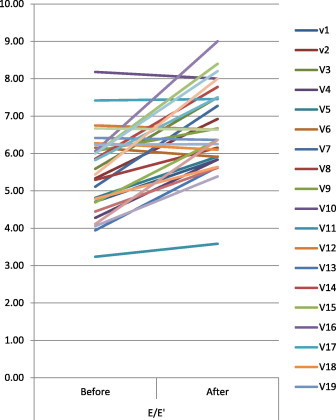
Individual lines showing the Doppler changes of the mitral valve before and after smoking.
Color M-mode propagation velocity Vp
The Vp was markedly reduced from 67.8 ± 8 to 55.2 ± 3.5 after smoking with P value < 0.001. This finding is reflected on the LVFvp which increased from 9.8 ± 1.4 to 10.5 ± 1.3 after smoking with P value < 0.001.
Effect of smoking on the RV
Cigarette smoking was found to affect both the RV systolic and diastolic functions. All changes were statistically significant at P value < 0.001. Fig. 3 presents the percent of changes of the Doppler parameters in the RV from baseline after single cigarette smoked.
Figure 3.
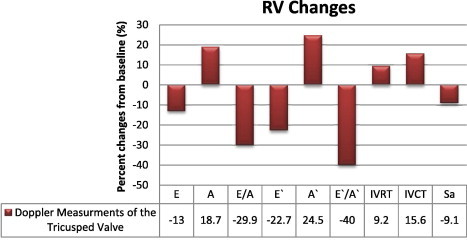
Changes (%) in the right ventricular function from the baseline after single cigarette smoking.
Doppler findings of the tricuspid valve
There is a significant reduction in trans-tricuspid early inflow velocity (E wave) after smoking 60.6 ± 9.7 vs. 52 ± 9.6 after smoking with P value < 0.001. However, late inflow velocity (A wave) increased significantly from 42.2 ± 6.5 to 50.1 ± 6.6 after smoking with P value < 0.001 which in turn reflected as a significant reduction in the E/A ratio from 1.45 ± 0.25 vs. 1.06 ± 0.19 after smoking with P value < 0.001. This is still within normal range but trending towards impaired diastolic filling.
Tissue Doppler findings on the tricuspid valve
The E′ is significantly decreased from 14.1 ± 1.8 before smoking to 10.9 ± 2.4 after smoking. While the A′ is increased from 10.2 ± 2.4 before smoking to 12.7 ± 3.6 after smoking which is reflected on E′/A′ ratio which is also showed significant reduction from 1.5 ± 0.3 before smoking to 0.9 ± 0.3 after smoking. The Sa is markedly decreased from 11 ± 3.1 before smoking to 10 ± 2.5 after smoking. All changes were statistically significant at P value < 0.001. Fig. 4 shows individual lines presenting the E′/A′ ratio changes before and after smoking.
Figure 4.
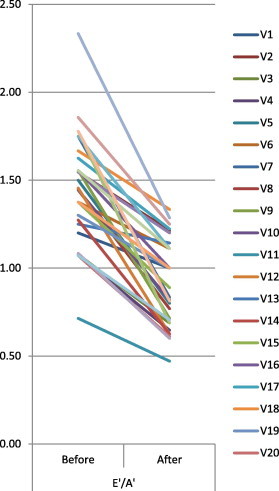
Individual lines showing the Doppler changes of the tricuspid valve before and after smoking.
IVRT
In our study the IVRT of the RV is significantly increased from 62.9 ± 7.5 to 68.7 ± 7.9 after smoking with P value < 0.001. These changes are shown in Fig. 5.
Figure 5.
Individual lines showing the IVRT changes of the RV before and after smoking.
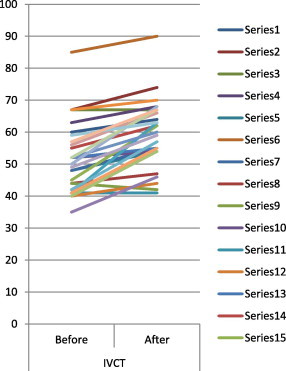
IVCT
The IVCT of the RV is significantly increased from 51.9 ± 10.7 to 60 ± 10.3 after smoking with P value < 0.001.
Discussions
Previous studies revealed that chronic smoking may impair both the LV and RV diastolic functions and this impairment was clearly demonstrated in chronic smokers after smoking one cigarette [17,18]. On the other hand, the acute effect of cigarette smoking on both the LV and RV systolic and diastolic has not been adequately studied.
The results of our study showed that smoking of a single cigarette is associated with an acute alteration of the RV and LV diastolic function towards impaired relaxation and significant changes of RV systolic function with no changes on the LV systolic function. However, Doppler changes in all subjects were not extensive enough to be graded as even grade I diastolic dysfunction.
Previous studies showed a significant association between E′ and LV relaxation [15]. In our study, the E′ septal is significantly decreased from 15.3 ± 2.4 to 11.2 ± 1.1 after smoking. The main hemodynamic determinants of A′ include LA systolic function and LVEDP, such that an increase in LA contractility leads to increased A′ velocity, whereas an increase in LVEDP leads to a decrease in A′ [19]. In our study, the A′ increased from 10.7 ± 2.4 before smoking to 13.2 ± 2.6 after smoking which was reflected on E′/A′ septal ratio which also showed significant reduction from 1.5 ± 0.3 before smoking to 0.9 ± 0.2 after smoking.
Previous studies observed that cigarette smoking containing at least 0.9 mg nicotine [9] or acute administration of 1.35 mg of nicotine [12] produced significant decrease of the E wave and increase of the A wave velocities and increase of the IVRT duration. These results were consistent with our findings where smoking one cigarette containing with at least 0.4 mg nicotine produced changes of the LV diastolic function in the form of reduction of the E wave velocity by 9.8%, and increase of the A wave velocity by 13.7% which, accordingly, resulted in reduction of E/A ratio by 20% from the baseline.
The E/E’ ratio which is a predictor of LV filling pressures [20] significantly increased by 21.8% and the E′/A′ decreased by 40%. In healthy young persons, a Vp greater than 50 cm is associated with normal diastolic function, and E/Vp ⩾ 2.5 predicts PCWP > 15 mmHg with reasonable accuracy [15].
In our study the Vp was markedly reduced by 18.6% after smoking a single cigarette. These finding are consistent with the study done by Alam et al. [10] who studied the acute effects of smoking on left ventricular function in 36 healthy subjects. These authors did not find any smoking-related, acute change in LV systolic function but they observed a significant change in trans-mitral flow measurements and concluded that cigarette smoking significantly changed the LV diastolic function.
Few studies have addressed the acute effect of cigarette smoking on the RV function. Our study revealed that the acute effect of cigarette smoking is associated with RV diastolic impairment expressed as a reduction in the E wave and elevation of the A wave velocities which reflected in the E/A ratio of the tricuspid valve by reduction of 29.9% from the base line while the tissue Doppler examination of the tricuspid valve revealed that after smoking a single cigarette there was a reduction of the E′ velocity by 22.7%, elevated A′ velocity by 24.5% and a marked 40% reduction of the E′/A′ ratio. Our findings are consistent with Lichodziejewska et al. [18] who studied the chronic and acute effects of smoking on left and right ventricular relaxation in young healthy smokers. They found prolonged DT, higher A wave and lower E/A ratio in MVF, and higher S wave and lower S/D ratio in PVF in healthy young smokers in comparison to nonsmokers. These changes were more pronounced after acute inhalation of nicotine. They concluded that smoking one cigarette in healthy chronic smokers produced impairment of both the RV and LV relaxation.
The Sa is a simple and reproducible measure to assess basal RV free wall function and should be used in the assessment of RV systolic function. Sa less than 10 cm should raise the suspicion of an abnormal RV systolic function, particularly in a younger adult [10]. In our study, the Sa is obviously decreased by 9.1% and this strongly correlates with tendency towards impaired RV systolic function. Our finding is in contrast to Onur Akpınar, [21] regarding the acute effect of smoking on RV systolic function and LV diastolic function but it is consistent with it regarding the acute effect of smoking on the RV diastolic function. Onur [21] and his colleagues studied the acute effects of smoking on right and left ventricular function on twenty healthy young males. Results at baseline and at minutes 5, 15, 30, 60 consecutively after smoking were compared. They found that both the right and left ventricular diastolic functions were impaired significantly with tissue Doppler echocardiography but there was no change in systolic functions. All changes seen after smoking a cigarette almost returned to baseline levels after 30 min.
Impaired myocardial relaxation leads to slow and prolonged fall in the RV pressure, which results in a longer time interval before it drops below RA pressure [22]. Therefore, tricuspid valve opening is delayed, and the IVRT is prolonged. In our study, the IVRT of the RV significantly increased from 62.9 ± 7.5 to 68.7 ± 7.9 after smoking with a percentage increase of 9.2% while the IVCT of the RV significantly increased by 15.6% from 51.9 ± 10.7 before smoking to 60 ± 10.3 after smoking. This is consistent with Storke et al. [9] who found an increase of the IVRT duration after smoking one cigarette but these in contrast to Kyriakides et al. [12] who investigated 20 smokers with coronary artery disease compared to 20 healthy smokers. After acute administration of 1.35 mg of nicotine, there was no change in IVRT, DT, or A-wave velocity and no changes were found in any Doppler echocardiographic filling parameter.
Limitations of the study
First, we intended to assess the acute effect of cigarette smoking on healthy non-smokers, but due to ethical issues, we conducted our study on recent light smokers. We assumed the acute effect of single cigarette smoking would be similar for either groups, but due to the results of the study we concluded that the acute effect of cigarette smoking on the non-smoker will be stronger. Second, long term follow up is needed to assess the prevalence of clinically evident diastolic heart failure in acute and chronic smokers and the long term effect on mortality.
Conclusions
Our study reveals that acute smoking alters the diastolic functions in both ventricles and results in the impairment of the RV systolic function that declares itself in the form of reduction of the Sa value through the TDI of the tricuspid valve.
These findings are relevant clinically since they might explain the impairment of diastolic function seen in recent smokers and may also indicate that smoking can explain some episodes of acute diastolic heart failure.
Conflict of Interest
Funding of this study was provided by the University of Dammam’s deanship of research.
Footnotes
Funding of this study was provided by the University of Dammam’s deanship of research

References
- 1.Poelaert J., Skarvan K., editors. Transoesophageal echocardiography in anaesthesia and intensive care medicine. 2nd ed. BMJ Books; 2004. [Google Scholar]
- 2.Halley C.M., Houghtaling P.L., Khalil M.K., Thomas J.D., Jaber W.A. Mortality rate in patients with diastolic dysfunction and normal systolic function. Arch Intern Med. 2011;171(12):1082–1087. doi: 10.1001/archinternmed.2011.244. [DOI] [PubMed] [Google Scholar]
- 3.Mureddu G.F., Agabiti N., Rizzello V. Prevalence of preclinical and clinical heart failure in the elderly. A population-based study in Central Italy. Eur J Heart Fail. 2012;14(7):718–729. doi: 10.1093/eurjhf/hfs052. [DOI] [PubMed] [Google Scholar]
- 4.AHA/ACCF Secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 Update. A Guideline from the American Heart Association and American College of Cardiology Foundation. http://circ.ahajournals. [DOI] [PubMed]
- 5.Ayanian J.Z., Cleary P.D. Perceived risks of heart disease and cancer among cigarette smokers. JAMA. 1999;281:1019–1021. doi: 10.1001/jama.281.11.1019. [DOI] [PubMed] [Google Scholar]
- 6.Jee S.H., Suh I., Kim I.S., Appel L.J. Smoking and atherosclerotic cardiovascular disease in men with low levels of serum cholesterol: the Korea Medical Insurance Corporation Study. JAMA. 1999;282(22):2149–2155. doi: 10.1001/jama.282.22.2149. [DOI] [PubMed] [Google Scholar]
- 7.Njølstad I., Arnesen E., Lund-Larsen P.G. Smoking, serum lipids, blood pressure and sex differences in myocardial infarction. Circulation. 1996;93(3):450–456. doi: 10.1161/01.cir.93.3.450. [DOI] [PubMed] [Google Scholar]
- 8.Suskin N., Sheth T., Negassa A., Yusuf S. Relationship of current and past smoking to mortality and morbidity in patients with left ventricular dysfunction. J Am Coll Cardiol. 2001;37(6):1677–1682. doi: 10.1016/s0735-1097(01)01195-0. [DOI] [PubMed] [Google Scholar]
- 9.Störk T., Eichstädt H., Möckel M., Bortfeldt R., Müller R., Hochrein H. Changes of diastolic function induced by cigarette smoking: an echocardiographic study in patients with coronary artery disease. Clin Cardiol. 1992;15(2):80–86. doi: 10.1002/clc.4960150205. [DOI] [PubMed] [Google Scholar]
- 10.Alam M., Samad B.A., Wardell J., Andersson E., Höglund C., Nordlander R. Acute effects of smoking on diastolic function in healthy participants: studies by conventional Doppler echocardiography and Doppler tissue imaging. J Am Soc Echocardiogr. 2002;15(10, Pt 2):1232–1237. doi: 10.1067/mje.2002.124006. [DOI] [PubMed] [Google Scholar]
- 11.Störk T., Danne O., Müller R., Möckel M., Hochrein H. Effect of smoking on relaxation and filling behavior of the left ventricle in healthy probands. An echocardiography study. Article in German. Med Klin (Munich) 1991;86(4):173–179. [PubMed] [Google Scholar]
- 12.Kyriakides Z.S., Kremastinos D.T., Rentoukas E., Mavrogheni S., Kremastinos D.I., Toutouzas P. Acute effects of cigarette smoking on left ventricular diastolic function. Eur Heart J. 1992;13(6):743–748. doi: 10.1093/oxfordjournals.eurheartj.a060250. [DOI] [PubMed] [Google Scholar]
- 13.Barutcu I., Esen A.M., Kaya D. Effect of acute cigarette smoking on left and right ventricle filling parameters: a conventional and tissue Doppler echocardiographic study in healthy participants. Angiology. 2008;59(3):312–316. doi: 10.1177/0003319707304882. [DOI] [PubMed] [Google Scholar]
- 14.Lang R.M., Bierig M., Devereux R.B. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s guidelines and standards committee and the chamber quantification writing group, developed in conjunction with the European association of echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18(12):1440–1463. doi: 10.1016/j.echo.2005.10.005. [DOI] [PubMed] [Google Scholar]
- 15.Nagueh S.F., Appleton C.P., Gillebert T.C., Marino P.N. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22(2):107–133. doi: 10.1016/j.echo.2008.11.023. [DOI] [PubMed] [Google Scholar]
- 16.Tumuklu M.M., Ildizli M., Ceyhan K., Cinar C.S. Alterations in left ventricular structure and diastolic function in professional football players: assessment by tissue Doppler imaging and left ventricular flow propagation velocity. Echocardiography. 2007;24(2):140–148. doi: 10.1111/j.1540-8175.2007.00367.x. [DOI] [PubMed] [Google Scholar]
- 17.Karakaya O., Barutcu I., Esen A.M. Acute smoking induced alterations in Doppler echocardiographic measurements in chronic smokers. Tex Heart Inst J. 2006;33(2):134–138. [PMC free article] [PubMed] [Google Scholar]
- 18.Lichodziejewska B., Kurnicka K., Grudzka K., Malysz J., Ciurzynski M., Liszewska-Pfejfer D. Chronic and acute effects of smoking on left and right ventricular relaxation in young healthy smokers. Chest. 2007;131(4):1142–1148. doi: 10.1378/chest.06-2056. [DOI] [PubMed] [Google Scholar]
- 19.Nagueh S.F., Sun H., Kopelen H.A., Middleton K.J., Khoury D.S. Hemodynamic determinants of mitral annulus diastolic velocities by tissue Doppler. J Am Coll Cardiol. 2001;37(1):278–285. doi: 10.1016/s0735-1097(00)01056-1. [DOI] [PubMed] [Google Scholar]
- 20.Hillis G.S., Møller J.E., Pellikka P.A. Noninvasive estimation of left ventricular filling pressure by E/e’ is a powerful predictor of survival after acute myocardial infarction. J Am Coll Cardiol. 2004;43(3):360–367. doi: 10.1016/j.jacc.2003.07.044. [DOI] [PubMed] [Google Scholar]
- 21.Akpınar O., Ilgenli T.F. Acute effects of smoking on right ventricular function; a tissue Doppler imaging study on healthy subjects. Swiss Med Wkly. 2007;137(5–6):91–96. doi: 10.4414/smw.2007.11375. [DOI] [PubMed] [Google Scholar]
- 22.Rudski L.G., Lai W.W., Afilalo J. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23(7):685–713. doi: 10.1016/j.echo.2010.05.010. [DOI] [PubMed] [Google Scholar]