

Abstract
Objective
The purpose of this study was to examine the causality and severity of maxillofacial trauma (MFT) among patients referred to a tertiary heath care center in the Southern Aseer region of Saudi Arabia.
Materials and methods
The charts of all MFT patients referred to the tertiary care center from September 2010 to November 2011 were retrospectively reviewed. Pertinent data, including patient age, gender, and cause of injury, were obtained from 101 selected charts.
Results
Male patients comprised 91% of the 101 selected cases. The highest percentage of MFT cases (88.7%) were caused by road traffic accidents (RTAs) while physical altercations and sports injuries accounted for approximately 6% and 2.8% of MFT cases, respectively. A high fracture: patient ratio of 2.4:1 was observed, which was likely due to vehicular speeding (high energy trauma) involved in RTAs in the mountain regions.
Conclusion
RTAs are a major cause of MFT in the southern region of Saudi. These accidents cause a heavy burden on the health care sector.
Keywords: Road traffic accidents, Maxillofacial fractures, Trauma, Causes
1. Introduction
Road traffic accidents (RTAs) are a major cause of death in Saudi Arabia (Shanks et al., 1994; Alahmed et al., 2004), particularly in the southern region, due to its unique geographic character. Aseer Southern Saudi Arabia is a mountainous and hilly region (2000–2300 m above sea level) of approximately 81,000 km2 in area, with an estimated population of 1,563,000. Reckless driving, failure to follow traffic rules, and driving by unlicensed teenager and elderly individuals contribute heavily to the high incidence of RTAs in the region.
Aseer Central Hospital is the major tertiary health care center (THCC) in the southern region of Saudi Arabia, where more than 4 million individuals reside. Aseer Central Hospital is located in the capital city of Abha, which is home to many major academic, economic, and health care centers. Many individuals in the smaller cities and villages around Abha hold agricultural and commercial occupations. These cities and villages are mainly located on mountainsides and connected by intercity roads, and residents frequently use pick-up vehicles to transport goods for their families and farms. Unlicensed youth and elderly males are not uncommon drivers in the region (Ansari et al., 2000).
The causality and prevalence of maxillofacial trauma (MFT) vary among different regions in the world. Multiple factors contribute to the causality and severity and, hence, the direct effect on the health care sector. We performed a study to investigate the causality and severity of MFT cases in the Southern Aseer mountain region of Saudi Arabia.
2. Methods
Ethical approval for this retrospective and descriptive study was obtained from the local institutional review board. All of the protocols for this study were performed in accordance with the Declaration of Helsinki. None of the authors have any conflicts of interest related to this study. The charts of all outpatients, inpatients, and emergency department patients at the THCC from September 2010 to November 2011 were reviewed. After charts with incomplete information or missing details were eliminated, 101 cases were included in this study. All pertinent data to examine the causality and severity of MFT, including the patient’s age, gender, and mechanism of injury, were recorded.
3. Results
RTAs were responsible for the largest percentage of MFT cases (90 cases, 89.1%), followed by physical altercations (8 cases, 7.9%) and sports injuries (3 cases, 2.9%) (P < 0.0001 by chi-square test, Fig. 1). There was a male predilection for MFT (males: 92 cases, 91%, females: 3 cases, 9%; P < 0.0001 by chi-square test, Fig. 2). Table 1 presents the incidence of MFT patterns. Mandible fracture was the most common pattern (50.6% of cases), followed by fracture of the zygoma maxillary orbital complex (28%). In mandible fractures, the condyle was involved in 31% of cases, the parasymphysis in 29%, and the angle in 18%. We observed 243 fractures in 101 patients. Forty patients (39%) presented with one fractured site, and 62 patients (61%) presented with two or more fractured sites.
Figure 1.
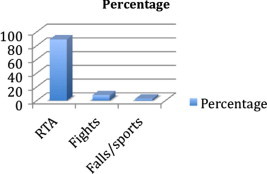
A bar graph showing that RTA form the major etiology of maxillofacial trauma compared to other causes.
Figure 2.
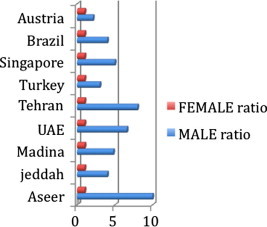
A graph showing that the Southern Aseer region has an extremely high-traumatized male to female ratio compared to other surrounding regions.
Table 1.
The incidence of maxillofacial fractures.
| Site | Percentage (%) |
|---|---|
| Mandible | 50.68 |
| Condyle | 31.08 |
| Coronoid | 2.70 |
| Ramus | 1.35 |
| Angle | 18.91 |
| Body | 8.10 |
| Parasymphysis | 29.72 |
| Symphysis | 1.35 |
| Dentoalveolar | 6.75 |
| ZMOC | 27.39 |
| Frontal, NOE | 21.91 |
ZMOC, Zygoma Maxilla Orbital complex; NOE, Naso ethmoid orbital complex.
4. Discussion
RTAs are responsible for many traumatic injuries in Saudi Arabia, particularly in rural regions and among young individuals. Most of the RTAs are preventable occurrences. The annual incidence of MFT recorded in the THCC in the present study is comparable to that in other studies, which have reported about 140 MFT cases per year, and the incidence of RTAs is similar to those in other developing countries (Shanks et al., 1994; Adeyemo et al., 2005). Most MFT patients were 20–30 years of age, similar to the age range reported in surrounding regions (Bener and Crundall, 2005; Ashar et al., 1999; Klenk and Kovacs, 2003).
The male:female ratio of 10:1 is relatively high compared to ratios in other regions in Saudi Arabia. For example, the reported male: female ratio for MFT in Jeddah city was 4:1 (Shanks et al., 1994) and for Almadina was 4.8:1 (Rabi and Khateery, 2002) (Fig. 2). The increased incidence might be attributed to the culture in the region. Whereas females spend much of their time at home, males spend more time on motor vehicles as a primary means of transport and entertainment. We found a similar situation when we compared the ratio in southern Saudi Arabia to those in neighboring and international countries (Fig. 2). For example, the male: female ratio for MFT was reported as 3:1 in Turkey (Aksoy et al., 2002; Ozkaya et al., 2009), 3:1 in Jordan (Bataineh, 1998), 6.6:1 in Alain city of the United Arab Emirates (Bener and Crundall, 2005; Ashar et al., 1999; Klenk and Kovacs, 2003), 8:1 in Tehran (Motamedi, 2003), 5:1 in Singapore (Tan and Lim, 1999), 4:1 in Brazil (Brasileiro and Passeri, 2006), 2.1:1 in Austria (Gassner et al., 2003), 2.3:1 in South Africa (Bamjee et al., 1996), and 2.7:1 in Nigeria (Adeyemo et al., 2005; Ajike et al., 2005).
The high rates of involvement of the condyle and parasymphysis in RTA-related MFTs can be explained by the mechanism of injury in RTA. Frequently, the patient is injured while speeding and not wearing a seat belt. This situation can result in anterior–posterior-directed injury to the chin/parasymphysis region, with the forces transmitted directly to both condyles, causing parasymphyseal and condylar fracture. The incidence of condyle fracture found here (31.08%) is close to the incidence rates reported in Iran (32%) (Motamedi, 2003), Nigeria (25%) (Adeyemo et al., 2005), and the United Arab Emirates (32%) (Ashar et al., 1999; Alahmed et al., 2004). However, we observed a higher incidence of zygoma maxillo-orbital complex fractures compared to other regions (Fig. 3).
Figure 3.
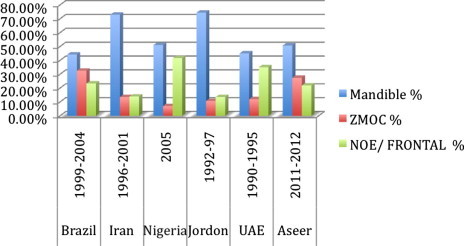
A graph showing the variability of mandible, ZMOC, and NOE/Frontal fractures in Aseer compared to other regions showing the high incidence of midface and upper face fractures.
5. Conclusion
The results of the study presented in this paper clearly indicate that RTAs are a major health care threat in the southern region of Saudi Arabia including Aseer. RTAs are the major cause of general trauma and MFT in the region. Younger drivers, careless driving, speeding, and lack of seat belt use are major contributors to RTA rates. Males were 10 times more likely to be affected by MFT than females. The magnitude and the severity of these preventable injuries indicate that they are a major threat to the community and health care system in terms of hospital resources, time, and cost, as well as the impacts on the patients and their families. These findings can be used to alert the community and authorities about this issue, leading to the development of community awareness and educational programs. We recommend that traffic laws in the region be enforced more strongly through speed control strategies, helicopter surveillance, street surveillance cameras, and the control of heavy truck traffic.
Acknowledgments
The author would like to thank Dr. Mobarak Asiri (ACH-Med. Director), Dr. Shakeel Ahmad (OMS–ACH), Dr. Sara Bukhari (BDS – King Abdulaziz University), Prof. Adel Mostafa (Prosthodontics – King Khalid University), and the Maxillofacial Research Center in King Khalid University for their help in conducting this research as dedicated to the family’s of all the college students who were lost by RTAs in Saudi Arabia.
Footnotes
Peer review under responsibility of King Saud University.

References
- Adeyemo W.L., Ladeinde A.L., Ogunlewe M.O., James O. Trends and characteristics of oral and maxillofacial injuries in Nigeria: a review of the literature. Head Face Med. 2005;1:7–12. doi: 10.1186/1746-160X-1-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ajike S.O., Adebayo E.T., Amanyiewe E.U., Ononiwu C.N. An epidemiologic survey of maxillofacial fractures and concomitant injuries in Kaduna, Nigeria. Niger. J. Surg. Res. 2005;7(3):251–255. [Google Scholar]
- Aksoy E., Unlü E., Sensöz O. A retrospective study on epidemiology and treatment of maxillofacial fractures. J. Craniofac. Surg. 2002;13(6):772–775. doi: 10.1097/00001665-200211000-00012. [DOI] [PubMed] [Google Scholar]
- Alahmed H.E., Jaber M., Abu Fanas S.H., Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: a review of 230 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2004;98(2):166–170. doi: 10.1016/j.tripleo.2004.01.020. [DOI] [PubMed] [Google Scholar]
- Ansari S., Akhdar F., Mandoorah M., Moutaery K. Causes and effects of road traffic accidents in Saudi Arabia. Public Health. 2000;114(1):37–39. doi: 10.1038/sj.ph.1900610. [DOI] [PubMed] [Google Scholar]
- Ashar A., Khateery S., Kovacs A., Tisza L. Etiology and patterns of facial fractures in alain, United Arab Emirates. Saudi Dent. J. 1999;11(3):109–113. [Google Scholar]
- Bamjee Y., Lownie J.F., Cleaton-Jones P.E., Lownie M.A. Maxillofacial injuries in a group of South Africans under 18 years of age. Br. J. Oral Maxillofac. Surg. 1996;34(4):298–302. doi: 10.1016/s0266-4356(96)90006-6. [DOI] [PubMed] [Google Scholar]
- Bataineh A.B. Etiology and incidence of maxillofacial fractures in the north of Jordan. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998;86(1):31–35. doi: 10.1016/s1079-2104(98)90146-9. [DOI] [PubMed] [Google Scholar]
- Bener A., Crundall D. Road traffic accidents in the United Arab Emirates compared to Western countries. Adv. Transportation Stud. 2005;6:5–12. [Google Scholar]
- Brasileiro B.F., Passeri L.A. Epidemiological analysis of maxillofacial fractures in Brazil: a 5-year prospective study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006;102(1):28–34. doi: 10.1016/j.tripleo.2005.07.023. [DOI] [PubMed] [Google Scholar]
- Gassner R., Tuli T., Hächl O., Rudisch A., Ulmer H. Cranio-maxillofacial trauma: a 10 year review of 9,543 cases with 21,067 injuries. J. Craniomaxillofac. Surg. 2003;31(1):51–61. doi: 10.1016/s1010-5182(02)00168-3. [DOI] [PubMed] [Google Scholar]
- Gusztav Klenk, Adam Kovacs. Etiology and patterns of facial fractures in the United Arab Emirates. J. Craniofac. Surg. 2003;14(1):78–84. doi: 10.1097/00001665-200301000-00014. [DOI] [PubMed] [Google Scholar]
- Motamedi M.H. An assessment of maxillofacial fractures: a 5-year study of 237 patients. J. Oral Maxillofac. Surg. 2003;61(1):61–64. doi: 10.1053/joms.2003.50049. [DOI] [PubMed] [Google Scholar]
- Ozkaya O., Turgut G., Kayali M.U., Uğurlu K., Kuran I., Baş L. A retrospective study on the epidemiology and treatment of maxillofacial fractures. Ulus Travma Acil Cerrahi Derg. 2009;15(3):262–266. [PubMed] [Google Scholar]
- Rabi A.G., Khateery S.M. Maxillofacial trauma in al madina region of Saudi Arabia: a 5-year retrospective study. Asian J. Oral Maxillofac. Surg. 2002;14(1):10–14. [Google Scholar]
- Shanks N.J., Ansari M., Al-Kalai D. Road traffic accidents in Saudi Arabia. Public Health. 1994;108(1):27–34. doi: 10.1016/s0033-3506(05)80032-0. [DOI] [PubMed] [Google Scholar]
- Tan W.K., Lim T.C. Aetiology and distribution of mandibular fractures in the National University Hospital, Singapore. Ann. Acad. Med. Singapore. 1999;28(5):625–629. [PubMed] [Google Scholar]