

Abstract
Botulinum toxin type A (BoNT-A) has been reported as an effective treatment for chronic migraine. When BoNT-A is injected on the frontalis muscle for chronic migraine, an unexpected clinical side effect called the "Mephisto sign" may occur. The aim of this article is to propose a method to eliminate or prevent the Mephisto sign side effect. A 25-year-old female patient visited the hospital and was diagnosed with chronic migraine. A total of 155 U of BoNT-A was injected into 31 sites. 2-weeks later, and the patient developed the Mephisto sign. An additional 2-U dose was administered bilaterally to the lateral-most point of the frontalis muscles, and the eyebrow morphology returned to normal within 2-3 weeks. We propose that the development of the Mephisto sign may be prevented with an additional BoNT-A injection of 2-4 U bilaterally to the lateral most point of the frontalis muscles during the primary injection process.
Keywords: Migraine disorders, botulinum toxin type A, eyebrows
INTRODUCTION
Botulinum toxin type A (BoNT-A) has been used to treat many diseases, including strabismus, blepharospasm, dystonia, glabella wrinkle, hyperhidrosis and cerebral palsy. In 2010, the United States Food and Drug Administration approved the use of BoNT-A (BOTOX, Allergan, Irvine, CA, USA) to prevent chronic migraine in adult patients, and it emerged as a second choice of treatment for chronic migraine patients who did not respond to the existing pharmacotherapy. The approval was made based on the double-blind, randomized, placebo-controlled phases of the Phase III Research Evaluating Migraine Prophylaxis Therapy (PREEMT) clinical program.1,2
BoNT-A injection has been reported as an effective treatment for chronic migraine. According to Blumenfeld, et al.,3 a minimum of 155 U of BoNT-A is recommended for chronic migraine to be injected in a total of 31 sites. It has been reported that 5 U each of BoNT-A should be injected in 4 sites of the frontalis muscle. The medial injection sites are located at a point with an invisible line drawn up about 1.5 cm from the medial end of the eyebrow from the corrugator injection site. The lateral injection sites are about 1.5 cm lateral and parallel to the medial injections sites explained previously.
When BoNT-A is injected to treat chronic migraine, an unexpected clinical side effect may occur. The "Mephisto sign" may develop as a side effect of BoNT-A injection into the frontalis muscle, whereby the outer end of the eyebrow is located above the inner end, possibly producing an intimidating impression. It is also referred to as a "quizzical look", "Spock's eyebrow", "a sinister look" or "'joker' face".4 Although temporary, this is a concerning result for both clinicians and patients, since the effect may last for at least 3 months.
CASE REPORT
A 25-year-old female patient visited the hospital due to frequent headaches, and was diagnosed with chronic migraine. There was no specific medical history. She did not effectively respond to various types of pharmacotherapy, and BoNT-A injection was indicated. BoNT-A injections were performed as described above, so that a total of 155 U was injected into 31 sites. At the follow-up appointment 2 weeks later, the patient reported a change in eyebrow morphology, showing the Mephisto sign. An additional BoNT-A dose of 2 U each was administered to the lateral-most point of the frontalis muscle bilaterally. However, the morphology of eyebrow became normalized within 2-3 weeks after this additional injection.
DISCUSSION
As described herein, when BoNT-A is injected to the original sites proposed for chronic migraine, a side effect may occur in eyebrow morphology. After injection, the distal ends of the eyebrows-which are normally positioned below the height of the eyebrow contour (Fig. 1A)-become raised so that they are in a more superior position compared to the rest of the eyebrow, pointing upwards, forming the Mephisto sign (Fig. 1B). This condition occurs when the lateral fibers of the frontalis muscles, which raise eyebrows, are not sufficiently paralyzed compared to the medial fibers. Consequently, the inner end of the eyebrow falls and the outer end raises because of paralysis of the medial fibers and hyperactivity of the lateral fibers, resulting in brow malposition to make a hook shape.4,5
Fig. 1.
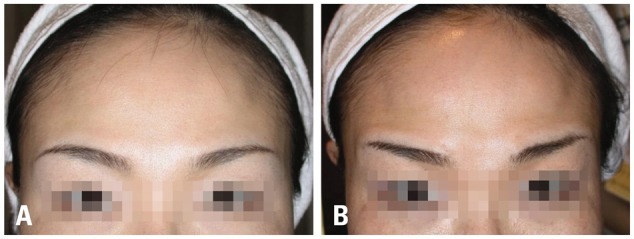
(A) Before BoNT-A injection, (B) 2 weeks after BoNT-A injection. BoNT-A, botulinum toxin type A.
In the case described herein, this condition was relieved via an additional injection of BoNT-A at the 2-week follow-up appointment. It is quite likely that the additional injection paralyzed the lateral fibers of the frontalis muscle that were not fully paralyzed earlier, thereby evenly reducing muscle tone on the entire frontalis muscle and resulting in an even location maintenance of eyebrow morphology. While the Mephisto sign may be relieved by an additional injection, it might also be prevented entirely by simply adding this procedure during the primary injection, taking into account the underlying anatomy. When injecting BoNT-A at the four predetermined sites in the frontalis muscle, 2 to 4 U of additional BoNT-A injection at the lateral-most point of the frontalis muscle (Fig. 2) will paralyze the frontalis muscle fully,6 thus preventing the appearance of the Mephisto sign.
Fig. 2.
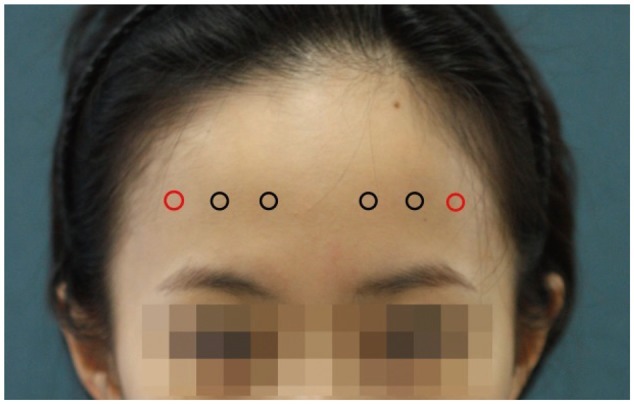
Proposed injection points of BoNT-A on the frontalis muscle in chronic migraine, with additional injection points marked in red. BoNT-A, botulinum toxin type A.
A detailed and accurate knowledge of the anatomy of the muscles that raise and lower the eyebrows is important for predicting the interaction between the muscles after BoNT-A injection in chronic migraine. The probability of the occurrence of the Mephisto sign may vary depending on the length, structure and morphology of the frontalis muscle and injection skills of clinician. Nevertheless, it is difficult to predict the chances of outbreak.
If the Mephisto sign occurs, it is likely that patients develop troubles in social life because of negative impression which may lead to poor relationship between clinicians and patients. An additional BoNT-A injection at a later date on the position mentioned above may improve the eyebrow, however, unsettling the trust issues. It is also uneconomical, considering additional visit of the patients and a need to open an additional new bottle of BoNT-A and using only 2 to 4 U.
A well-controlled research with a larger number of subjects to confirm the benefit/risk ratio of the injection is needed. Nevertheless, an additional injection using the leftover BoNT-A during the primary injection for chronic migraine is expected to be efficient, prevents the side effects and causes minimum additional discomfort to patients. On the other hand, occurrence of risk factors of an additional injection including eyebrow ptosis, eyelid ptosis and upper eyelid swelling should be more accurately estimated.
In conclusion, we propose this simple method to prevent the Mephisto sign after BoNT-A injection for chronic migraine: injection of an additional 2-4 U of BoNT-A into the distal end of the frontalis muscle either prophylactically at the primary injection, or at the follow-up appointment if necessary. This is a proposal based on our own limited experiences, and further well-designed studies are required to confirm its efficacy.
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Aurora SK, Dodick DW, Turkel CC, DeGryse RE, Silberstein SD, Lipton RB, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia. 2010;30:793–803. doi: 10.1177/0333102410364676. [DOI] [PubMed] [Google Scholar]
- 2.Diener HC, Dodick DW, Aurora SK, Turkel CC, DeGryse RE, Lipton RB, et al. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia. 2010;30:804–814. doi: 10.1177/0333102410364677. [DOI] [PubMed] [Google Scholar]
- 3.Blumenfeld A, Silberstein SD, Dodick DW, Aurora SK, Turkel CC, Binder WJ. Method of injection of onabotulinumtoxinA for chronic migraine: a safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache. 2010;50:1406–1418. doi: 10.1111/j.1526-4610.2010.01766.x. [DOI] [PubMed] [Google Scholar]
- 4.De Maio M, Rzany B. Botulinum Toxin in Aesthetic Medicine. Berlin, Heidelberg: Springer-Verlag; 2007. Safety of Botulinum Toxin in Aesthetic Medicine; p. 123. [Google Scholar]
- 5.Carruthers A, Carruthers J. Using Botulinum Toxins Cosmetically: a Practical Guide. Boca Raton: Taylor & Francis Group; 2003. Horizontal forehead lines; p. 35. [Google Scholar]
- 6.Carruthers A, Carruthers J. Botulinum Toxin. Philadelphia: Elsevier Saunders; 2005. Upper face treatment; p. 36. [Google Scholar]