

Abstract
The overhead pitching motion is described as a coordinated sequence of body movements and muscular forces that have an ultimate goal of achieving high ball velocity and target accuracy. An understanding of the dynamic overhead throwing motion outlined in this clinical commentary can assist the clinician in addressing the unique injuries experienced by the pitcher. The potential biomechanical sources for injury have been studied utilizing videography and electromyographic techniques due to the rapid pace with which the pitching motion occurs. This clinical comentary will describe what is widely accepted as the six phases of the pitching motion and the relationship to the kinetic chain theory as well as outline the common mechanical faults that can lead to increased tissue stress and potential injury.
Level of Evidence:
5
Keywords: baseball, overhead athlete, pitching mechanics
INTRODUCTION
The repetitive overhead motion in baseball places extraordinary stress on the musculoskeletal system. Shoulder and elbow forces and torques have been extensively studied and suggest that injuries are primarily thought to be related to repetitive soft tissue microtrauma experienced at the extremes of motion during the pitching motion.1,2,3,4 An understanding of pitching mechanics and their effect on the kinetic chain is an essential component to allow sports medicine practitioners to return an athlete to maximum performance following injury. The kinetic chain in pitching can be thought of as an interaction of body segments, each upon the other, in a sequential pattern from the ground up. Evaluating the segments of the kinetic chain can therefore permit the clinician to accurately design an evaluation methodology that identifies potential sources of biomechanical stress related to injury development. There is a common belief among sports medicine professionals that proper pitching mechanics, taught early, may help reduce the risk of injury by minimizing the detrimental forces placed on the segments of the kinetic chain from the foot to the hand.
There is a growing body of knowledge reporting on the biomechanical differences and/or similarities of the adult and adolescent pitching motion. Several authors have indicated that pitch mechanics, muscular fatigue, pitch type and count are all risk factors for injury in the young pitcher.5,6,7,8,9,10,11 Comparing normal pitch mechanics to those following muscular fatigue in a simulated game (between 105 and 135 throws), revealed only moderate strength decreases in the shoulder internal rotators and flexors and little deviation of pitching form. However sports medicine professionals report that fatigue reduces the pitchers ability to reach maximum external rotation in late cocking and has been shown to reduce knee flexion angle at ball release, negatively affecting ball velocity.12,13,14 Many authors have suggested that pitch type, namely the curve ball, in adolescent athletes may contribute to an increased risk of shoulder and elbow injuries.5,6,7 Nissen et al15 reported lower shoulder and elbow moments throwing a curveball when compared to the fastball, concluding that increased injury rates in young pitchers is not caused by the curveball. A thorough understanding of the potential biomechanical sources for injury has enabled the development of effective treatment and rehabilitation regimens, often allowing baseball pitchers to return to their sport at their previous levels of competition. The purpose of this clinical commentary is to describe the widely accepted six phases of the pitching motion and their relationship to the kinetic chain and potential for injury.
Pitching Mechanics
Pitching mechanics can be described as a coordinated sequence of body movements and muscular forces that have an ultimate goal of high ball velocity and target accuracy. An effective pitching motion is dictated by an intricate relationship of increasing the speed of body segments speed starting from the ground up. The lower extremity, pelvis, and trunk are responsible for initiating kinetic force development and establish a base of support that serves to transfer potential energy to the subsequent segments, primarily the shoulder complex and elbow that in turn impart force to the baseball. This linkage system can be described as the sequential acceleration and deceleration of anatomical segments from the ground up with each transferring its energy to the more distal segment until the point of ball release and deceleration.5 The acceleration and deceleration components each place unique stresses on the soft tissues surrounding the glenohumeral joint.
The six phases of pitching include the wind‐up, stride (early cocking), late cocking, acceleration, deceleration, and follow through. Within each phase are sub‐segment movement patterns that are necessary for coordinated movement. The wind‐up phase has components of balance and initial forward movement while the stride encompasses arm path, foot placement/contact, stride length, stride angle, arm position at foot contact and the relationship of speed and timing between the lead leg hips and dominant shoulder segment. Late cocking incorporates elbow position in flexion, shoulder external rotation and trunk inclination, while acceleration includes shoulder internal rotation velocity, trunk forward movement towards target, and body position at ball release. Deceleration and follow through include trunk positioning, lead leg extension, and dissipation of force through upper extremity horizontal adduction. High speed video analysis has enabled an accurate dissection and description of these sub‐segments of the major phases and aids the sports medicine clinician in developing specific neuromuscular exercises, and range of motion and strength tests to design prevention of injury strategies and return to play parameters. Each of the phases of pitching will now be described in greater detail in the following sections.
Wind‐up
The wind‐up phase begins with the pitchers first movement from the static position of facing the batter with both feet on the rubber and is completed when the lead leg (target side) reaches maximum knee height. This phase of the pitching motion exhibits relatively low muscle activity as reported through indwelling electromyography to be below 21% MVC for the rotator cuff, scapular stabilizers and deltoid musculature.16 The final position of the wind‐up is referred to as the “balance point” at which time the pitcher starts to remove the ball from the glove in order to initiate the subsequent phase. (Figure 1) The wind‐up sets the timing pattern and tone for the remainder of the pitching motion. It is estimated that the wind‐up phase lasts between 0.5 and 1.3 seconds.17,18 The risk of injury during the wind‐up phase is low in comparison to the remainder of the pitching motion. While in the balance point position the pitchers shoulders should be aligned between home plate and second base with the hands together at roughly chest height demonstrating a stable center of gravity (COG). If the COG is positioned to far posteriorly or anteriorly the body segment sequence timing and transfer of torque in the kinetic chain will be transferred to the upper extremity thus predisposing the shoulder and elbow to injury. Several factors can contribute to faulty wind‐up mechanics; poor balance at maximum lead knee height secondary to reduced lower extremity strength and trunk control, premature forward movement towards home plate before reaching the balance point, tilting the COG posteriorly, and a high hand placement with shoulder in greater than 90° of abduction.
Figure 1.
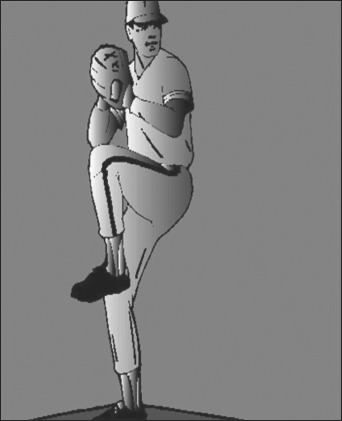
Balance Point‐Demonstrating a stable center of gravity (COG).
Stride (Early Cocking)
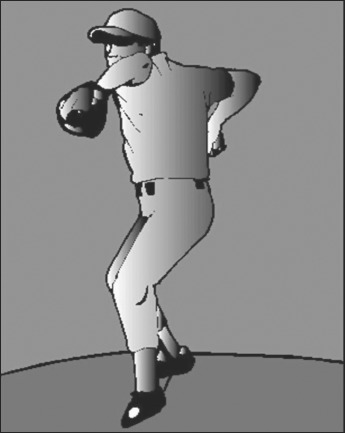
The stride is initiated from the point of maximum lead knee height to the point of foot contact. (Figure 2) Approximately 50% of ball velocity in the pitching motion is the resultant forces accumulated in the stride and trunk rotation.19 Once stabilization of the COG is achieved at wind‐up it must subsequently be lowered and accelerated towards home plate during the stride phase of pitching.
Figure 2.

Stride Phase‐Pelvis rotates towards target while the upper quarter remains quiet in a closed position producing spinal rotation.
The stride position is responsible for the proper positioning of the trunk and lower extremity in the transfer of energy to the upper extremity by increasing the distance and time that the trunk can rotate. A short stride would decrease potential force development via reduced trunk rotation potential. A key factor limiting stride length is soft tissue flexibility restrictions in the lead leg hamstrings and stance leg hip flexors or rotators. The knee and hip extensors of the lead leg act eccentrically to complete the stride to foot contact position. Hip external rotation range of motion and strength of the lead leg and internal rotation for the stance leg are crucial for an adequate stride length to be achieved. Lead leg hip control is facilitated through the gluteus maximus and minimus, piriformis and obterator internus musculature while stance hip internal rotation control is attributed to the tensor fascia latae, gluteus medius and the hamstrings.
During the stride phase the pelvis rotates at velocities between 400–700°/second while the upper quarter remains relatively quiet in a closed position thus producing spinal rotation.20 Spinal rotation produces a summation of force development between the lead leg/pelvis and the upper body through the development of muscular tension. (Figure 2) Youth pitchers exhibit a common stride fault associated with initiating trunk rotation prior to proper positioning of the scapula.21 Other common faults related to pitch mechanics in the stride phase are inadequate lead leg foot contact direction, stride length, stride angle and knee flexion angle.
Stride foot contact direction should be towards home plate or what is termed slightly “closed” towards third base side for a right handed pitcher. (Figure 3) Restricted lead leg hip external rotation and stance hip internal rotation can contribute to altered foot placement of the stride foot. An excessively closed foot contact position towards the third base side for a right handed pitcher results in the arm being ahead of the shoulder rotation and having to throw across the body to reach the strike zone effectively. This foot position “locks off” the lead side pelvis and hip thus not allowing the efficient transfer of energy to the arm for pitch velocity. The arm in turn has to speed up, after loosing momentum, to get to the appropriate ball release point thus placing excessive stress on the anterior shoulder, scapular stabilizers and medial elbow.
Figure 3.
Stride Foot Contact‐Direction should be towards home plate or “closed” towards third base side.
An open foot contact position can produce reduced ball velocity secondary to early pelvic rotation. Open foot positioning towards the first base side can alter the temporal rotation relationship on the upper torso and lower torso and increase stress on the anterior shoulder tissues in the late cocking to ball release phases of the pitch mechanics. A common problem with an open contact foot position is that the throwing arm is lagging behind the body rotation thus placing and increased valgus load on the medial elbow from subsequent late cocking through the acceleration phase. Other common causes for an open foot contact position are a short stride length, and rushing the delivery from the balance point with reduced lead leg knee height.
The stride angle is measured as the angle between the lead leg and stance leg at maximum foot contact. This angle is often measured when the pitcher reaches the foot flat position of the lead leg. The stride angle can give the clinician a general indication of hip flexibility. A short stride angle can be an indicator of a pitcher that may experience excessive abdominal muscle strains secondary to the increased demands on the oblique trunk musculature to accelerate the trunk and eventually the upper extremity in the transverse plane thus reducing the power generated by the lower quarter. As the pitcher initiates the stride movement towards the plate, the foot contact will abruptly stop the forward motion of the lower quarter to allow for the upper body to “whip” toward the target at ball release. Stride length remains a controversial subject normally relegated to pitching coach preference. Stride length is a measurement of distance at foot contact between the lead leg foot and stance leg foot with a measurement between 85–100% of the pitchers height as being in the normal range. A decreased stride length can reduce pitch velocity without changing accuracy while an increased stride is reported to improve velocity.22
During the stride the dynamic (rotator cuff and scapular stabilizers), and static stabilizers (capsuloligamentous tissue) of the shoulder must work in synchrony to allow for proper positioning of the scapular glenoid and the humeral head in order to minimize physiological tissue overload. The scapula must rotate upward and assume a retracted position to allow the rotator cuff and deltoid to abduct the arm in preparation for early cocking. An indication that there is reduced muscular strength or endurance in the scapular stabilizers is often observed in the pitcher demonstrating a lower elbow position in relation to shoulder height in the late cocking phase. The static stabilizers, primarily the inferior glenohumeral ligament act as check reins in restricting detrimental positions of excessive anterior and posterior humeral head translation in relation to the glenoid. The arm path from wind‐up to stride is initiated with the ball being removed from the glove with a smooth transition downward to a position where the hand is below the right hip and then subsequently up to an elbow height at or above the shoulder with an elbow flexion angle between 80°–100°. The hand position is in slight pronation with the fingers on top of the ball facing between second and third base. A common problem in young pitchers is initiating an arm path with the hand under the ball rather than on top thus placing the shoulder into early external rotation prior to achieving late cocking and maximum rotation. Other mechanical faults identified in the early cocking phase are an abnormally long arm path referred to as “long‐arming”, or an excessively flexed position of the wrist called “wrist hooking”. It is imperative that the early phases of the pitching motion (wind‐up and stride) must be evaluated carefully by the clinician as biomechanical flaws in these movement patterns potentially amplify stress to the static and dynamic stabilizers in subsequent phases which account for the majority of injuries in the pitcher.
Late Cocking
The late cocking phase is initiated as the lead foot contacts the ground and ends with the maximum external rotation (MER) position of the throwing shoulder.23 The focus of the pitching motion in late cocking is on the trunk, shoulder and elbow movement patterns. The trunk initiates a derotation pattern back towards the plate initiated by the lead side pelvis. Trunk rotation is accomplished through contraction of the lead side internal oblique and erector spinae and is coupled with stance side external oblique muscle activity. The lead side knee moves from a flexed position at foot contact towards extension during trunk derotation in order to form a solid base of support for the trunk to begin forward flexion towards the target. Lumbopelvic and hip stability is controlled through gluteal muscular contraction. The gluteus maximus of the stance leg demonstrates a muscular contraction greater than 100% of the MVIC while externally rotating the hip during late cocking and arm acceleration. The stride leg gluteus medius in turn contracts to internally rotate the hip and exhibits a muscle contraction of approximately 145% MVIC from foot contact to ball release.24
The scapula must assume a retracted position in the scapular plane as the shoulder moves into abduction and external rotation. The shoulder is abducted 90° to 110° and externally rotates between 50° and 185°.19,25 Scapular upward rotation is accomplished through contraction of the serratus anterior and trapezius force couple is essential to maintain the subacromial space and reduce the risk of impingement and potential rotator cuff pathology.26 The shoulder abduction range previously described is maintained throughout the late cocking phase while the shoulder approaches MER. The rotator cuff, long head of the biceps and the deltoid musculature are responsible for compression of the humeral head in the glenoid fossa. During late cocking the subscapularis, latissimus dorsi and pectoralis major eccentrically contract while the infraspinatus and teres minor concentrically aid the deltoid in attaining extreme external rotation. The long head of the biceps acts to further aid in humeral head compression and stability as humeral external rotation increases past 60° in the late cocking position as it works to actively flex the elbow at MER.27,28 External rotation range is further restricted by the contribution of a varus torque produced by the ulnar collateral ligament (UCL) and the forearm pronators and writ flexors.29
The stride foot contact position can also contribute to the soft tissue stress placed on the upper extremity in late cocking. An open foot contact position (towards the first base side of the target line) indicated by reduced trunk flexion and rotation causes the upper extremity to lag behind the trunk and be positioned posterior to the scapular plane.30 Increased horizontal abduction of the shoulder posterior to the scapular plane is potentially deleterious to the anterior capsular structures as is the eccentric action of the subscapularis, pectoralis major and latissimus dorsi at maximal external rotation. Younger pitchers often experience impingement symptoms when there is anterior instability of the throwing shoulder. Athletes with anterior shoulder instability exhibit increased muscular activity of the long head of the biceps as it attempts to aid in reducing humeral head translation at MER.31 The anterior deltoid and pectoralis major act to horizontally adduct the humerus in the sagital plane approximately 20° during MER.32 The triceps act eccentrically in late cocking and act as a check rein against excessive elbow flexion. However, the triceps reverses its action concentrically as the elbow extends during the acceleration phase until ball release.33 Late cocking phase ends with MER. At MER the shoulder is abducted 90° to 100° and horizontally adducted up to 20° with approximately 90° of elbow flexion. (Figure 4)
Figure 4.

Late Cocking Phase‐Position of MER with shoulder abducted 90° to 100°, horizontally adducted up to 20° and 90°of elbow flexion.
Acceleration
The arm acceleration phase of the pitching motion is initiated at the point of MER and ends at ball release. Arm acceleration constitutes between 42–58 ms of the total pitch temporal sequence, making it one of the fastest human physical movements in sports activity.32 Amateur pitchers exhibit up to three times greater biceps and rotator cuff muscular activity than professional pitchers during the acceleration phase.34 The higher muscle activity may be a contributory factor to cuff overuse injuries in the younger pitcher. Trunk rotation and lateral flexion plays a critical role in maintenance of the abduction angle of the humerus at ball release. Excessive lateral trunk flexion can cause an over‐the‐top ball release point while a decreased angle has an inherent risk of releasing the ball with a sidearm throwing mechanism.32 Sidearm tracking of the arm through acceleration can contribute to an cumulative microtrauma placed on the medial elbow structures, primarily the UCL.
During this phase, the trunk has a highly stable base of support as both lead and stance (trail) feet are in contact with the ground during this phase. The anterior inclination angle of the trunk averages between 32° and 55° prior to ball release.35 (Figure 5) The kinetic chain from the stance (trail) leg to the hand in MER will demonstrate a reverse “C” position demonstrated in Figure 4. The latissimus dorsi, given its origin and insertion anatomic position and contraction through the lumbopelvic kinetic chain linkage, generates the greatest force during acceleration and positively increases ball velocity.36
Figure 5.

Acceleration‐Demonstrating humeral adduction, trunk inclination between 32° and 55° prior to ball release towards home plate and an extending lead leg.
The explosive nature of the shift from MER to rapid shoulder internal rotation and horizontal adduction occurs at over 9000°/second while the elbow reaches 2251 to 2728°/second in the scapular plane.22 Internal rotation and forced adduction of the humerus in late acceleration to ball release often is implicated as contributory to impingement complaints in the pitcher. At the ball release position, the scapula demonstrates high muscular activity, and should have maintained its orientation of abduction between 90° to 100° in relation to the trunk but now assumes a protracted orientation to maintain a stable base of support for the humeral head. The serratus anterior demonstrates high muscular activity during this phase to aid in scapular protraction.34 The latissimus dorsi and pectoralis major are responsible for rapid shoulder internal rotation during acceleration. The acceleration phase is marked by elbow extension to 25°, shoulder internal rotation, wrist flexion and pronation to 90° and lead leg knee extension.37
Deceleration (Follow Through)
The deceleration phase begins at ball release and culminates with maximal dominant shoulder internal rotation and 35° of horizontal adduction.38 The pitcher should assume a fielding ready position at the completion of the follow through phase where shoulder and elbow muscular activity are minimal as compared to the previous phases of the pitching motion. The stance side foot is completely off the ground during follow through and the trunk rotates over the extending lead leg as the trunk is descending down the mound towards home plate. (Figure 6) Lead side hip internal rotation range and flexibility will contribute to the pitchers ability to reach a balanced fielding position after follow through. Commonly, a pitcher that completes follow through in an “off‐balance” position has early mechanical problems in the stride direction phase of the motion. The teres minor, infraspinatus and posterior deltoid muscles act eccentrically as a restraint to humeral head translation while the serratus and rhomboids aid in scapular stability during deceleration as the arm is extended towards home plate during the follow through.16 It has been suggested by several authors that the eccentric action of the posterior musculature and capsular soft tissue required to dissipate the extreme rotational and distraction forces may contribute to the development of glenohumeral internal rotation deficiency (GIRD).16 The bicep is reported to reach peak eccentric muscular activity during follow through in order to decelerate the extending elbow and forearm as it pronates.39
Figure 6.
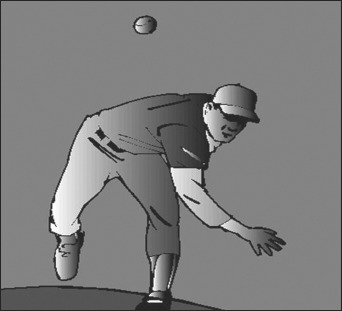
Deceleration (Follow Through)‐Demonstrates maximal dominant shoulder internal rotation and 35° of horizontal adduction.
CONCLUSION
The overhead throwing motion in baseball pitching is a complex interaction of body segment movements from the feet to the hand. Each segment contributes to the increased velocity of the subsequent segment to allow the ballistic action of throwing a baseball to be accomplished in an efficient manner. The summation of segmental speed imparts supra‐physiological stress on the soft tissue of the kinetic chain. The highly repetitive nature of the pitching motion predisposes the pitcher to microtrauma for both the static and dynamic stabilizers of the shoulder and elbow. The pitching motion is divided into six phases. The wind‐up and early cocking phase are responsible for setting the tone and timing of the body segment movements for the pitching motion. The balance point during wind‐up will give the clinician an indication of trunk control and the ability of the pitcher to coil and un‐coil in a controlled manner prior to the stride. Stride faults in direction and length can affect trunk rotation velocity and inclination and contribute to the throwing arm lagging behind the scapular plane and increase stress on the shoulder and elbow. The late cocking and acceleration phases generate the highest segmental velocities and these phases are implicated in the majority of pitching injuries. Poor pitching mechanics can compound the effect of repetitive stress placed on the soft tissues surrounding the scapulothoracis and glenohumeral joint and has been implicated as a potential risk factor for injury. The clinicians understanding of the pitching motion and biomechanical stress placed on the soft tissue will assure the completion of a comprehensive evaluation, appropriate rehabilitation, and the reduced incidence of future injuries through the development of injury prevention programs.
REFERENCES
- 1. Chen FS, Diaz VA, Loebenberg M, Rosen JE. Shoulder and elbow injuries in the skeletally immature athlete. J Am Acad Orthop Surg. 2005;13:172–185 [DOI] [PubMed] [Google Scholar]
- 2. Grana WA, Rashkin A. Pitcher’s elbow in adolescents. Am J Sports Med. 1980;8:333–336 [DOI] [PubMed] [Google Scholar]
- 3. Limpisvasti O, ElAttrache NS, Jobe FW. Understanding shoulder and elbow injuries in baseball. J Am Acad Orthop Surg. 2007;15:139–147 [DOI] [PubMed] [Google Scholar]
- 4. Olsen SJ II, Fleisig GS, Dun S, Loftice J, Andrews JR. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med. 2006;34:905–912 [DOI] [PubMed] [Google Scholar]
- 5. Fleisig G, Andrews J, Dillman C, Escamilla R. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23:233–239 [DOI] [PubMed] [Google Scholar]
- 6. Lyman S, Andrews J, Fleisig G. Youth pitching injuries: first‐ever examination sheds light on arm injuries in youth baseball. Sports Med Update. 1998;13:4–9 [Google Scholar]
- 7. Lyman S, Fleisig G, Andrews JR, Osinski ED. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30:463–468 [DOI] [PubMed] [Google Scholar]
- 8. Lyman S, Fleisig G, Waterbor J, et al. Longitudinal study of elbow and shoulder pain in youth pitchers. Med Sci Sports Exerc. 2001;33:1803–1810 [DOI] [PubMed] [Google Scholar]
- 9. Petty DH, Andrews JR, Fleisig GS, Cain EL. Ulnar collateral ligament reconstruction in high school baseball players: clinical results and injury risk factors. Am J Sports Med. 2004;32:1158–1164 [DOI] [PubMed] [Google Scholar]
- 10. Sabick M, Torry M, Lawton R, Hawkins R. Valgus torque in youth baseball pitchers: a biomechanical study. J Shoulder Elbow Surg. 2004;13:349–355 [DOI] [PubMed] [Google Scholar]
- 11. Sabick MB, Kim YK, Torry MR, et al. Biomechanics of the shoulder in youth baseball pitchers: implications for the development of proximal humeral epiphysiolysis and humeral retroversion. Am J Sports Med. 2005;33:1716–1722 [DOI] [PubMed] [Google Scholar]
- 12. Escamilla RF, Barrentine SW, Fleisig GS, et al. Pitching biomechanics as a pitcher approaches muscular fatigue during a simulated baseball game. Am J Sports Med. 2007;35:23–33 [DOI] [PubMed] [Google Scholar]
- 13. Mullaney MJ, McHugh MP, Donofrio TM, et al. Upper and lower muscle fatigue after a baseball pitching performance. Am J Sports Med. 2005;33:108–113 [DOI] [PubMed] [Google Scholar]
- 14. Murray TA, Cook TD, Werner SL, et al. The effects of extended play on professional baseball pitchers. Am J Sports Med. 2001;29:137–142 [DOI] [PubMed] [Google Scholar]
- 15. Nissen CW, Westwell M, Ounpuu S, et al. A biomechanical comparison of the fastball and curveball in adolescent baseball pitchers. Am J Sports Med. 2009;37:1492–1498 [DOI] [PubMed] [Google Scholar]
- 16. DiGiovine NM, Jobe FW, Pink M, Perry J. An electromyographic analysis of the upper extremity in pitching. J Shoulder Elbow Surg. 1992;1:15–20 [DOI] [PubMed] [Google Scholar]
- 17. Braatz MA, Gogia PP. The mechanics of pitching. J Ortho Sports Phys Ther. 1987;9:56–69 [DOI] [PubMed] [Google Scholar]
- 18. Nicholas JA, Grossman RB, Hershman EB. The importance of a simplified classification of motion in sports in relation to performance. Orthop Clin North Am. 1977;8:499–532 [PubMed] [Google Scholar]
- 19. Toyoshima S, Hoshikawa T, Miyashita M, et al. Contribution of the body parts to throwing performance. Biomechanics IV. Blatimore, University Park Press, 1974;169–174 [Google Scholar]
- 20. Pink MM. Understanding the linkage system of the upper extremity. Sports Med Arthroscopy Rev. 2001;9:52–60 [Google Scholar]
- 21. Keeley DW, Hackett T, Keirns M, et al. A biomechanical analysis of youth pitching mechanics. J Pediatr Orthop. 2008;28:452–459 [DOI] [PubMed] [Google Scholar]
- 22. Montgomery J, Knudson D. A method to determine stride length in baseball pitching. Appl Res Coaching Athl. 2002;17:75–84 [Google Scholar]
- 23. Pappas AM, Zawacki RM, Sullivan TJ. Biomechanics of baseball pitching, a preliminary report. Am J Sports Med. 1985;4:216–222 [DOI] [PubMed] [Google Scholar]
- 24. Oliver GD, Keeley DW. Gluteal muscle group activation and its relationship with pelvis and torso kinematics in high school baseball pitchers. J Strength Cond Res. 2010;24:3015–3022 [DOI] [PubMed] [Google Scholar]
- 25. Atwater AE. Biomechanics of over arm throwing movements and throwing injuries. Exerc Sports Sci Rev. 1979;7:43–85 [PubMed] [Google Scholar]
- 26. DeWilde L, Plasschaert F, Berghs B, et al. Quantified measurement of subacromial impingement. J Shoulder Elbow Surg. 2003;12:346–349 [DOI] [PubMed] [Google Scholar]
- 27. Itoi E, Kuechle DK, Newman SR, Morrey BF. Stabilizing function of the biceps in stable and unstable shoulders. J Bone Joint Surg. 1993;75B:564–550 [DOI] [PubMed] [Google Scholar]
- 28. Rodosky MW, Harner CW, Fu FH. The role of the long head of the biceps muscle and superior glenoid labrum in anterior stability of the shoulder. Am J Sports Med. 1994;22:121–130 [DOI] [PubMed] [Google Scholar]
- 29. Werner SL, Fleisig GS, Dillman CJ, Andrews JR. Biomechanics of the elbow during baseball pitching. J Orthop Sports Phys Ther. 1993;17:274–278 [DOI] [PubMed] [Google Scholar]
- 30. McKenzie CS. Trunk stability in professional baseball pitchers and it’s correlation to injuries and performance. Med Sci Sport Exerc. 2008;40 (Suppl): S49 [Google Scholar]
- 31. Kim SH, Ha KI, Kim HS, Kim SW. Electromyographic activity of the biceps brachii in shoulder with anterior instability. Arthroscopy. 2001;17:864–868 [DOI] [PubMed] [Google Scholar]
- 32. Dillman CJ, Fleisig GS, Andrews JR. Biomechanics of pitching with emphasis upon shoulder kinematics. J Orthop Sports Phys Ther. 1993;18:402–408 [DOI] [PubMed] [Google Scholar]
- 33. Fleisig GS, Escamilla RF, Barrentine SW. Biomechanics of pitching: mechanism and motion analysis. In: Injuries in Baseball. Philadelphia, PA: Lippincott‐Raven; 1998;3–22 [Google Scholar]
- 34. Gowan ID, Jobe FW, Tibone JE, et al. A comparative electromyographic analysis of the shoulder during pitching: professional versus amateur pitchers. Am J Sports Med. 1987;15:586–590 [DOI] [PubMed] [Google Scholar]
- 35. Matsuo T, Escamilla R, Fleisig GS, et al. Comparison of kinematics and temporal parameters between different pitch velocity groups. J Appl Biomech. 2001;17:1–13 [Google Scholar]
- 36. Bassett RW, Browne AO, Morrey BF. Glenohumeral muscle force and moment mechanics in a position of shoulder instability. J Biomech. 1990;23:405–415 [DOI] [PubMed] [Google Scholar]
- 37. Werner SL, Guido JA, Stewart GW, et al. Relationship between throwing mechanics and shoulder distraction in collegiate baseball pitchers. J Shoulder Elbow Surg. 2007;16:37–42 [DOI] [PubMed] [Google Scholar]
- 38. Meister K. Injuries to the shoulder in the throwing athlete. Am J Sports Med. 2000;28:265–275 [DOI] [PubMed] [Google Scholar]
- 39. Jobe FW, Moynes DR, Tibone JE, et al. An EMG analysis of the shoulder in pitching. Am J Sports Med. 1984;3:218–220 [DOI] [PubMed] [Google Scholar]