

Abstract
An 18-year-old German woman presented with progressive cerebellar ataxia since early childhood, delayed cognitive development, and hypogonadotropic hypogonadism. MRI demonstrated diffuse cerebral hypomyelination, cerebellar atrophy, and thin corpus callosum; X-ray revealed persistent milk teeth and hypoplastic crowns and roots (figure), indicative of 4H syndrome (hypomyelination, hypodontia, hypogonadotropic hypogonadism). POLR3B sequencing1 revealed 2 compound heterozygous mutations (C527R [C.1579T>C] and the common ancestral V523E [C.1568T>A]2).
An 18-year-old German woman presented with progressive cerebellar ataxia since early childhood, delayed cognitive development, and hypogonadotropic hypogonadism. MRI demonstrated diffuse cerebral hypomyelination, cerebellar atrophy, and thin corpus callosum; x-ray revealed persistent milk teeth and hypoplastic crowns and roots (figure), indicative of 4H syndrome (hypomyelination, hypodontia, hypogonadotropic hypogonadism). POLR3B sequencing1 revealed 2 compound heterozygous mutations (C527R [C.1579T>C] and the common ancestral V523E [C.1568T>A]2).
Figure. T2-weighted MRI and dental X-ray.
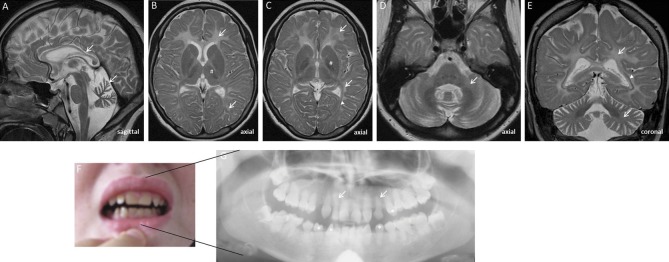
MRI shows diffuse hyperintense cerebral and cerebellar hypomyelination (B–E; arrows), relatively sparing the (hypointense) anterolateral thalami, globi pallidi (B, C; number sign), and optic radiations (C, E; arrowhead), as well as vermian cerebellar atrophy and thin corpus callosum (A; arrows). X-ray specifies teeth abnormalities (F), revealing persistent milk teeth (arrows) and hypoplastic crowns and roots (G; asterisks).
These characteristic MRI and dental findings1 help to identify Pol-III–associated leukodystrophies in the substantial share of patients with unexplained leukodystrophy and facilitate straightforward genetic diagnostics. POLR3A and POLR3B mutations are common in hypomyelinating leukodystrophies, even when hypogonadotropic hypogonadism or hypodontia is absent.2
Supplementary Material
Footnotes
Download teaching slides: www.neurology.org
AUTHOR CONTRIBUTIONS
Dr. Synofzik: acquisition of data, design and conceptualization of the study, revising the manuscript. Dr. Bernard: acquisition of data, revising the manuscript. Dr. Lindig: acquisition of data, revising the manuscript. Dr Gburek-Augustat: acquisition of data, revising the manuscript.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
M. Synofzik received research grants by the Volkswagen Stiftung, the Robert Bosch Stiftung, and UK ataxia, and honoraria from Actelion Pharmaceuticals. G. Bernard has received honoraria from Santhera Pharmaceuticals and Actelion Pharmaceuticals. T. Lindig and J. Gburek-Augustat report no disclosures. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Tetreault M, Choquet K, Orcesi S, et al. Recessive mutations in POLR3B, encoding the second largest subunit of Pol III, cause a rare hypomyelinating leukodystrophy. Am J Hum Genet 2011;89:652–655 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Daoud H, Tetreault M, Gibson W, et al. Mutations in POLR3A and POLR3B are a major cause of hypomyelinating leukodystrophies with or without dental abnormalities and/or hypogonadotropic hypogonadism. J Med Genet 2013;50:194–197 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.