

Abstract
Most research linking early pubertal development to substance use has focused on the effects of pubertal timing (age at which a certain stage of pubertal development is reached or pubertal status at a particular age—related to the maturation disparity hypothesis), but little research has focused on pubertal tempo (rate of growth through pubertal stages—related to the maturation compression hypothesis). However, both timing and tempo have not only been identified as important components of pubertal development, with different predictors, but have also been shown to be independently associated with other adolescent psychopathologies. Using latent growth-curve modeling, this study examined how pubertal status at age 12 and pubertal tempo (between 11 and 13 years) related to substance use from 15 to 16 years in boys from low socioeconomic backgrounds (N = 871). Results showed that both pubertal status at age 12 and tempo were significant predictors of increased levels of substance use and problems in mid to late adolescence. In an attempt to identify mechanisms that may explain the association between pubertal development and substance use it was found that sensation seeking partially mediated the association between pubertal status at age 12 and substance use behaviors. Impulse control was found to moderate the association sensation seeking had with marijuana use frequency, with high sensation-seeking scores predicting higher marijuana use frequency only at low levels of impulse control. These findings highlight the importance of considering multiple sources of individual variability in the pubertal development of boys and provide support for both the maturational disparity and compression hypotheses.
Keywords: adolescence, puberty, substance use, impulsivity, sensation seeking
Adolescence is an important developmental period for the onset of substance use and misuse, with some considering exploratory drug use as normative during this period (e.g., Shedler & Block, 1990). Some Canadian statistics show that 42% of adolescents attending Grades 9 through 11 (or 3–5 of high school) have used cannabis in the last year, and by Grade 11, 86% of them were drinking alcohol (Dubé et al., 2009). Similarly, epidemiologic studies in the United States show that up to 50% of high school students report binge drinking, and around 25% report having tried an illicit substance (Office of National Statistics, 2008; U.S. Department of Health and Human Services, 2007). Youth substance use is also prevalent in Europe, with almost half of all young people in the United Kingdom trying an illegal drug by the age of 16 years and around one third of adolescents between 13 and 17 years drinking alcohol at least once a week (The Information Centre, 2008). Short-term consequences of early onset drinking and drug use include poor grades; school drop-out; higher risk for assault; suicide; homicide; accidental injuries, including death from alcohol poisoning; and psychosocial immaturity, with longer term consequences, including a range of behavioral and mental health problems (Chassin et al., 2010; Grant & Dawson, 1998; King, Meehan, Trim, & Chassin, 2006; Odgers et al., 2008; Single, Rehm, Robson, & Van Truong, 2000). Given these serious consequences and the increased risk for adult substance abuse and dependence observed as the age of substance use onset decreases (Grant & Dawson, 1998), identifying factors in childhood and adolescence related to substance use initiation and frequency is essential for developing evidence-based targeted prevention and clinical practice guidelines.
Although the development of substance misuse has been shown to be multidetermined, and multiple risk factors for substance misuse have been identified, recent research has highlighted the important role of early pubertal development. A number of studies have shown that puberty is a sensitive period that is associated with the onset, increase, or both, of emotional and behavioral problems, including depression (e.g., Mendle, Harden, Brooks-Gunn, & Graber, 2010), externalizing behaviors such as aggression and delinquency (e.g., Felson & Haynie, 2002; Harden & Mendle, 2012; Lynne, Graber, Nichols, Brooks-Gunn, & Botvin, 2007), and substance use (e.g., Costello, 2007; Hayatbakhsh, Najman, McGee, Bor, & O’Callaghan, 2009; Patton et al., 2004; Westling, Andrews, Hampson, & Peterson, 2008).
Much of the research linking early pubertal development and problem behaviors, including substance use, was conducted in girls, with findings showing that early maturing girls also initiated smoking and drinking earlier (Wiesner & Ittel, 2002; Wilson et al., 1994) and were more likely to smoke marijuana and experiment with other illegal substances (Magnusson, Stattin, & Allen, 1985; Prokopcakova, 1998). Although it is recognized that early maturation has different implications for boys and girls, with some studies showing that boys and their peers tend to view their early development more positively than girls (Petersen & Crockett, 1985), interest in the link between early pubertal development and substance use and other problem behaviors in boys has increased in recent years. Many of these recent studies have shown that early pubertal maturation is also significantly associated with substance use in boys (Hayatbakhsh et al., 2009; Tschann et al., 1994; Westling et al., 2008), with one exception (Ge et al., 2006), whose discrepant findings might be due to the restricted range of puberty levels in the sample.
Pubertal Timing and Tempo
Although there is much literature linking early pubertal development to substance use, most of the studies assessed pubertal development at only one time point. However, such an approach does not provide an account of individual variability in the rate of pubertal development. This variability may also be relevant to the development of substance use during adolescence. Pubertal development is often indexed using a categorical system devised by Marshall and Tanner (1969, 1970). Marshall and Tanner categorized secondary sexual changes occurring during puberty (e.g., facial and body hair and genital development in boys) into five stages of pubertal development ranging from prepubertal (no signs of maturation, stage 1) to postpubertal (full level of maturation, stage 5; Marshall & Tanner, 1969, 1970). Although all youth go through puberty, considerable variability in their onset of puberty and progression through these stages can be observed. In the literature, the age at which a certain stage of pubertal development is reached, or, still, the pubertal stage–status reached at a given age, is generally referred to as pubertal timing, whereas the rate across time taken to pass through the various stages of maturation is generally referred to as pubertal tempo (Marshall & Tanner, 1969, 1970). The relevance of both pubertal timing and tempo to developmental psychopathology may be illustrated by studies of depression. First, Mendle et al. (2010) used latent-growth curve models to examine how pubertal timing and tempo were associated with depressive symptoms. They were the first to include puberty measures at four time points, enabling the assessment of pubertal tempo in a reliable way. Mendle et al. (2010) showed that while pubertal timing, but not tempo, was significantly associated with depressive symptoms in girls across ages 8 to 13 years, both pubertal timing and tempo were important predictors for the development of these symptoms in boys across ages 8 to 14 years. These findings highlight the importance of considering multiple sources of individual variability in pubertal development.
Although the literature linking substance use and externalizing problems to pubertal timing in adolescence, reviewed above, is extensive, much less is known about the link with pubertal tempo. One recent study by Marceau, Ram, Houts, Grimm, and Susman (2011) modeled pubertal timing and tempo in boys and girls and examined their associations with a range of problems, including externalizing problems in adolescence. They showed that while pubertal tempo was an important correlate of externalizing problems in 15-year-old girls, this association was less consistent in 15-year-old boys (Marceau et al., 2011). In the specific case for substance use, to our knowledge, only one study has previously assessed puberty at more than one time point. Dick, Rose, Pulk-kinen, and Kaprio (2001) assessed puberty at both 12 and 14 years of age, which allowed them to measure change or stability in pubertal scores across these ages. They showed that prevalence rates of alcohol use and smoking at 14 years were higher in individuals whose pubertal development remained consistently advanced, at both 12 and 14 years, compared with same-aged peers who exhibited advanced maturation at only one of these time points. Although two assessments of puberty cannot provide a reliable estimate of pubertal tempo and significance of the difference across pubertal development groups was not tested, these findings provide preliminary evidence that both pubertal timing and change (and potentially tempo) may be important predictors of substance use behaviors.
Although both early pubertal timing and fast tempo have been associated with environmental stress, recent work has shown that pubertal tempo has unique contextual and biological antecedents that are distinct from those of pubertal timing (e.g., Ellis, Shirtcliff, Boyce, Deardorff, & Essex, 2011). For example, whereas pubertal timing has been shown to be influenced by genes, environmental toxins, nutrition, prepubertal fat, and body weight (Belsky et al., 2007), faster pubertal tempo in early adolescence has been related to adverse family factors (e.g., low-quality parent– child relationship) and lower cortisol activation (Ellis, 2004; Ellis et al., 2011). This suggests that the mechanisms linking pubertal tempo with psychopathology may be different than those linking pubertal timing with psychopathology. This has yet to be tested in the context of substance use research. However, determining first if pubertal tempo is uniquely associated with substance use in adolescence, independently from effects of pubertal timing, would provide necessary initial evidence that both are important correlates of substance use problems and that different biological and psychosocial mechanisms may be involved in how they confer risk for substance use problems.
Models Linking Pubertal Timing and Tempo to Psychopathology
Although there is some evidence that early pubertal timing and possibly fast tempo are associated with substance use, the mechanisms that may explain these associations are less well understood. We note two theoretical accounts relevant to this question: One related to timing, the other to tempo. The maturation disparity hypothesis relates to timing and posits that earlier maturing children are forced to face a range of new challenges and stressors with fewer resources than peers who reach the same maturational stage at a later chronological age (Ge, Conger, & Elder, 2001; Ge, Jin, & Natsuaki, 2009; Petersen & Crockett, 1985). Such challenges and stressors may be hormone-related emotional liability, shifting peer and family relationships, and new parental and societal expectations.
The maturation compression proposed by Mendle et al. (2010) in their study of depression provides a possible explanation as to why fast pubertal tempo may be associated with emotional and behavioral problems. This model follows a similar logic to the maturation disparity hypothesis and states that a faster developmental tempo may reduce the time a child has to (a) complete important developmental tasks characteristic of the pre-adolescent period, and (b) understand and adapt to the new biological and social challenges that come with puberty. Furthermore, children who experience a faster progression through puberty may attract unwanted attention from peers and adults. The generalizability of this model to substance use is unknown.
The primary objective of this study was to examine whether pubertal timing, as measured by the status reached in preadolescence, and pubertal tempo were independently associated with substance use and problems in adolescent boys and in doing so to test both the maturation disparity and compression hypotheses in the prediction of adolescent substance use problems.
Personality and the Link Between Pubertal Development and Substance Use
A secondary question is whether personality characteristics may explain the link between pubertal development and substance use (Patton et al., 2004). Personality characteristics, such as sensation seeking and poor impulse control have been prospectively implicated in the later development of substance misuse (e.g., Castellanos-Ryan & Conrod, 2011; Conrod, Castellanos-Ryan, & Strang, 2010; Crawford, Pentz, Chou, Li, & Dwyer, 2003; Masse & Tremblay, 1997), showing that the higher the sensation seeking and lower the impulse control in childhood and early adolescence, the higher the substance use problems later during adolescence.
Beyond possible direct associations with substance use, the link between sensation seeking and pubertal development, even after controlling for chronological age is supported by a number of human studies (Canals, Vigil-Colet, Chico, & Marti-Henneberg, 2005; Martin et al., 2002; Steinberg et al., 2008). Animal studies also indicate that increases in reward seeking coincide with the onset of pubertal development (e.g., Spear, 2000). Although sensation seeking has been identified theoretically as an important factor that may explain the association between puberty and increased risk-taking behaviors, only one study that we know of has shown a significant indirect effect from puberty to increased risky or problem behaviors through sensation seeking. That study showed that sensation seeking and other disinhibited traits, such as positive and negative urgency, were associated with early pubertal timing (pubertal status at 11 years; Gunn & Smith, 2010). Furthermore, significant indirect paths from pubertal status at 11 years to drinking behaviors were found through disinhibited traits and positively reinforcing alcohol expectancies (e.g., the expectancy that alcohol makes people friendly, social, or wild; Gunn & Smith, 2010). However, although these findings are consistent with the hypothesis proposing that sensation seeking may explain the link between pubertal timing and substance use, they do not provide definite support for it because of the cross-sectional nature of the data. A test of this hypothesis is further challenging because some studies have shown that drinking and substance use in early adulthood were associated with concurrent and later changes in sensation seeking and impulsivity (e.g., Littlefield, Verges, Wood, & Sher, 2012; Littlefield, Wood, & Sher, 2009; Quinn, Stappen-beck, & Fromme, 2011), suggesting that the association between personality and substance use may actually be bidirectional. Therefore, a stronger test of the theory requires longitudinal data in which pubertal staging and personality are measured before substance use has become frequent in youth.
Although sensation seeking and poor impulse control are both considered disinhibited traits and, thus, are related, a number of studies have shown that impulsivity and sensation seeking are distinct traits that can be measured independently from each other (e.g., Whiteside & Lynam, 2001). Furthermore, they have been shown to have different genetic, neurobiological, cognitive, and motivational correlates (e.g., Belin, Mar, Dalley, Robbins, & Everitt, 2008; Castellanos-Ryan & Conrod, 2012; Finn, Sharkansky, Brandt, & Turcotte, 2000; Mustanski, Viken, Kaprio, & Rose, 2003) and follow distinct developmental courses (Harden & Tucker-Drob, 2011). More important to note, in contrast to sensation seeking, the development of impulse control has been shown to be independent of pubertal development (Steinberg et al., 2008; see also Paus, 2005, for a review). This would suggest that impulse control, contrary to sensation seeking, could not explain or mediate the link between pubertal timing and possibly tempo and risky or problem behaviors. Indeed Steinberg (2007, 2008) and Steinberg et al. (2008) described the dual-systems model, which suggests that heightened risky behaviors observed in adolescence, including substance use, are the product of a relatively higher puberty-driven inclination to seek out sensations and excitement and a relatively immature ability to control impulses. The fact that impulse control typically develops slowly through adolescence and only reaches full maturity in early adulthood (Luna, Padmanabhan, & O’Hearn, 2010; Steinberg, 2010) suggests that early pubertal onset or faster pubertal tempo outpaces the capacity of the still immature impulse-control system to regulate puberty-driven sensation seeking. This hypothetical process results in a higher vulnerability to risk-taking and problem behaviors. Thus, individuals’ predisposition to poor impulse control may enhance the effect of pubertal timing and tempo on substance use, identifying this trait as a moderator rather than a mediator.
Therefore a secondary objective of this study was to examine the role of sensation seeking and poor impulse control in the puberty–substance use link. Specifically, we wanted to examine whether sensation seeking partly explained the link between pubertal status reached in preadolescence and substance use problems and whether the association between pubertal status reached in preadolescence, fast pubertal tempo, and high sensation seeking in pre- and early adolescence and substance use behaviors in mid to late adolescence were exacerbated by poor impulse control.
The Current Study
In sum, this study has two objectives. First, as previously stated, it aims to clarify the roles of pubertal status (operationalized here as the level of pubertal development attained by the age of 12 years) and tempo (operationalized as rate of change in pubertal development across 11–13 years) in the development of substance use in adolescent boys. Four substance use outcomes were investigated across adolescence: two frequency measures assessed across 15 to 16 years (i.e., frequency of alcohol use and marijuana use), one tapping drug use experimentation (or diversity) across 15 to 16 years (e.g., no. of different drugs tried), and another tapping substance use problems assessed across 15 to 16 years. The use of these different longitudinal measures allowed testing whether pubertal development was differentially associated with distinct dimensions of adolescent substance use (Oliva, Keyes, Iacono, & McGue, 2012; Shedler & Block, 1990). In this way, this study will examine for the first time whether pubertal status at age 12 and tempo are both independently associated with substance use and problems in adolescence. In doing so, this study will be the first to test whether the maturation compression hypothesis can be supported in the prediction of adolescent substance use and problems in boys. This first objective will be met to the extent that we also establish whether the link between pubertal development and substance use is independent of other developmental factors and demographic variables, such as early substance use history, childhood disruptive behaviors, and socioeconomic factors, shown to be important risk factors for future substance use problems (Grant & Dawson, 1998; Lillehoj, Trudeau, Spoth, & Madon, 2005; Masse & Tremblay, 1997).
As our secondary objective, this study also aims to clarify the role of two personality traits in the puberty–substance use link. That is, this study aims to test whether sensation seeking is associated with pubertal development and can partly explain the link between early pubertal maturation and substance use, and whether poor impulse control exacerbates that link. Although some evidence for both mediation and moderation models exists, no prospective studies have tested the association between these factors in the development of substance use and problems in adolescence.
Within this context, the primary and secondary hypotheses of the current study are the following:
Hypothesis 1: More advanced pubertal status and fast pubertal tempo will predict higher substance use in mid to late adolescence, independent of previous substance use history, childhood disruptive behaviors, and socioeconomic factors.
Hypothesis 2a: Sensation seeking will explain (mediate) the prospective association between pubertal status and substance use.
Hypothesis 2b: Poor impulse control will moderate the association pubertal status and tempo, as well as their potential putative mediator, that is, sensation seeking, have with substance use in mid to late adolescence.
Method
Participants and Procedure
The 871 boys who participated in this study were a subsample of an ongoing longitudinal study entitled the Montreal Longitudinal and Experimental Study of Low SES boys. One thousand thirty-seven French-speaking Caucasian boys were originally recruited in 1984, when they were 6 years old (SD = 0.31), from kindergartens in low socioeconomic neighborhoods of Montreal, Quebec, Canada. (For further information on recruitment and selection criteria, please see Vitaro, Brendgen, & Tremblay, 1999; Séguin, Pihl, Harden, Tremblay, & Boulerice, 1995; and Tremblay, Pihl, Vitaro, & Dobkin, 1994.) Ethnicity and socioeconomic status (SES) were homogeneous as a result of the selection procedure. At their first assessment in kindergarten, 67% of the boys lived with both parents, whereas 24% lived with their mothers only. The mean number of school years completed by the parents was 10.5 (SD = 2.8) for the mothers and 10.7 (SD = 3.2) for the fathers. The mean age of parents at birth of their first child was 25.4 years (SD = 4.8) for mothers and 28.4 years (SD = 5.6) for fathers.
Boys were assessed annually from ages 10 to 17 years by self-report questionnaires. The 871 boys included in this study are those for whom substance use, puberty data, or both, were collected at least once during the yearly assessments: for substance use at ages 15 to 17 years and for puberty at ages 11 to 13 years. These 871 boys are considered representative of the overall sample as they did not differ from the remaining, unselected boys on demographic variables (maternal age at birth, maternal education, and family structure, all at p > .28; data was available for all 166 remaining boys), on whether they had used alcohol or marijuana by the age of 10 years (p = .25; available for 134 unselected boys), or on puberty scores at 11 years (p = .76; available only for 45 unselected boys).
Measures
All measures were administered in French. Instruments that were only available in English were translated into French and back-translated into English. The back-translations were evaluated and compared with the original versions of the questionnaires to verify that the original meaning was maintained.
Measures in mid to late adolescence (outcomes)
Four substance use outcomes were assessed: alcohol use frequency, marijuana use frequency, number of drugs tried, and substance use problems. Both alcohol and marijuana use frequency were assessed annually with the Self-Reported Delinquency Questionnaire (SRDQ; LeBlanc & Fréchette, 1989) at ages 15 and 16 years. This 25-item questionnaire includes three substance use items (alcohol use, marijuana use and drunkenness frequency), which are rated on a 4-point scale (never, once or twice, often, and very often). For this study, alcohol use and drunkenness were averaged at each year to create a composite alcohol use frequency score (αs = .82 at 15 years and .81 at 16 years). Also, at 15 and 16 years of age, boys were also asked to report whether they used any of the following substances over the last 12-month period: alcohol, marijuana, amphetamines, cocaine, psychedelics, barbiturates, tranquilizers, heroine, inhalants, and other drugs. At each year, these dichotomous items were summed to create a “number of drugs tried” score. Each of these outcomes assessed at 15 to 16 years were averaged to create composite scores at 15–16 years of alcohol frequency (test–retest = .74), marijuana use frequency (test–retest = .79), and number of drugs tried (test–retest = .54). Finally, substance use problems were assessed at 15 and 16 years by using the Personal Experience Screening Questionnaire (PESQ; Winters, 1992). This self-report measure was specifically designed for assessing substance use problems in adolescents. This questionnaire includes 18 items that measure the frequency of problems related to alcohol and drug use (e.g., used alcohol or other drugs when at school; made excuses to teachers about your alcohol or drug use) on a 4-point scale (never, once or twice, sometimes, and often). This measure has demonstrated good internal consistency and discriminant validity across a number of samples (Winters, 1992). In this sample, the alpha coefficient for this measure was .92 at 16 years.
Measures in early adolescence (putative mediators or moderators)
Sensation seeking and poor impulse control were assessed through self-reports at ages 13 and 14, using a French translation of the Eysenck Impulsiveness-Venturesomeness-Empathy scale (IVE7, Eysenck, Easting, & Pearson, 1984; Eysenck & Eysenck, 1978). For this study, only five items for each subscale were used, that is, those that had the highest factor loadings in the original scales (Eysenck & Eysenck, 1978; Eysenck et al., 1984): Impulsiveness: “Do you generally do and say things without stopping to think?” “Do you often get into trouble because you do things without thinking?” “Are you an impulsive person?” Do you usually think carefully before doing anything?” and “Do you mostly speak before thinking things through?” (Cronbach’s α = .72 at 13 years and .71 at 14 years; interitem correlation = .33 at 13 years and .32 at 14 years); and Venturesomeness (considered to be sensation seeking in this article): “Do you quite enjoy taking risks?” “Would you like to water ski?” “Would you like to skydive?” “Would you like to scuba-dive?” “Do you find it difficult to understand people who risk their lives climbing mountains?” (Cronbach’s α = .61 at 13 and .69 at 14 years; interitem correlation = .24 at 13 years and .29 at 14 years). To improve reliability of these self-report measures, subscales assessed at 13 and 14 years were averaged to create composite scores across 13–14 years of sensation seeking (test–retest = .67; Cronbach’s α, 10 items = .72) and poor impulse-control (test–retest = .67; Cronbach’s α, 10 items = .79).
In early adolescence, substance use frequency averaged across 13 and 14 years was also assessed. For this, a composite of alcohol use frequency and marijuana use frequency, assessed with the SRDQ (LeBlanc & Fréchette, 1989) annually at ages 13 and 14 years, was used. Individual measures of alcohol and marijuana use were not used because, although alcohol use frequency at 13–14 years was normally distributed (skew = 0.69, kurtosis = 0.16), marijuana use frequency at ages 13–14 years (skew = 4.05, kurtosis = 18.31) was not. In order to include some information on drug use behavior, the composite alcohol and marijuana use frequency measure (Cronbach’s α, four items = .71) was favored. Although not normally distributed (skew = 1.70, kurtosis = 3.90), this composite variable possessed acceptable levels of skewness and kurtosis for the use of maximum likelihood estimation (i.e., below 2 and 7, respectively; Curran, West, & Finch, 1996).
Measures in preadolescence
Pubertal development was assessed using the Pubertal Development Scale (Petersen, Crockett, Richards, & Boxer, 1988; Verlaan, Cantin, & Boivin, 2001) answered yearly by participants at ages 11–13. This three-item measure required boys to assess the status of their growth spurt, body and facial hair development, skin and voice changes, based on an ordinal scale: 1 (no development), 2 (beginning development), 3 (additional development), and 4 (development has already past). Scores were combined to create a puberty raw score at each time point. The reliability and validity of this measure has been previously assessed by Petersen et al. (1988) and others (Arim, Shapka, Dahinten, & Willms, 2007; Bond et al., 2006; Schmitz et al., 2004), showing that this scale is reliable and valid for both girls and boys. Although puberty scores were used in all analyses, Table 1 shows how these scores relate to Tanner stages (i.e., the range of scores that fall within each stage; based on Petersen et al., 1988) and the prevalence of each Tanner stage at each time point in this sample, showing that 99% boys had initiated puberty by age 13, but none had completed pubertal development. Table 2 shows means and standard deviations of puberty scores.
Table 1.
Pubertal Stage by Age
| Tanner stages (corresponding puberty scores) | 11 years | 12 years | 13 years |
|---|---|---|---|
| I. Prepubertal (3) | 21% | 7% | 1% |
| II. Beginning puberty (4–5) | 53% | 40% | 24% |
| III. Mid puberty (6–8) | 25% | 49% | 66% |
| IV. Advanced puberty (9–11) | 1% | 3% | 9% |
| V. Postpubertal (12) | 0% | 0% | 0% |
Table 2.
Correlations and Descriptive Statistics for Study Variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Alcohol use at 15–16 | — | |||||||||||||||
| 2. Marijuana use at 15–16 | 0.55* | — | ||||||||||||||
| 3. Drugs tried at 15–16 | 0.63* | 0.81* | — | |||||||||||||
| 4. SU problems at 15–16 | 0.67* | 0.82* | 0.78* | — | ||||||||||||
| 5. Puberty score at 11 | 0.13* | 0.07 | 0.08* | 0.12* | — | |||||||||||
| 6. Puberty score at 12 | 0.19* | 0.19* | 0.17* | 0.22* | 0.66* | — | ||||||||||
| 7. Puberty score at 13 | 0.19* | 0.16* | 0.18* | 0.20* | 0.47* | 0.70* | — | |||||||||
| 8. SS at 13–14 | 0.28* | 0.21* | 0.23* | 0.24* | 0.13* | 0.12* | 0.09* | — | ||||||||
| 9. IMP at 13–14 | 0.18* | 0.18* | 0.22* | 0.23* | 0.04 | 0.05 | 0.02 | 0.16* | — | |||||||
| 10. SU frequency at 13–14 | 0.56* | 0.49* | 0.47* | 0.53* | 0.16* | 0.22* | 0.18* | 0.28* | 0.21* | — | ||||||
| 11. SS Jesness at 10–11 | 0.13* | 0.09* | 0.13* | 0.10* | 0.06 | 0.08* | 0.02 | 0.19* | 0.09* | 0.13* | — | |||||
| 12. Teacher-rated IMP at 12 | 0.13* | 0.18* | 0.16* | 0.23* | 0.03 | 0.02 | 0.01 | 0.07 | 0.19* | 0.12* | 0.18* | — | ||||
| 13. Any SU by 12 | 0.26* | 0.22* | 0.18* | 0.25* | 0.14* | 0.16* | 0.11* | 0.15* | 0.14* | 0.43* | 0.07 | 0.03 | — | |||
| 14. Disruptive behaviors at 6 | 0.01 | 0.07 | 0.08* | 0.03 | 0.03 | 0.02 | −0.01 | 0.05 | 0.16* | 0.12* | 0.15* | 0.28* | 0.05 | — | ||
| 15. Maternal age at birth | −0.08* | −0.05 | −0.05 | −0.05 | −0.02 | −0.01 | −0.01 | 0.00 | −0.10* | −0.05 | −0.08* | −0.12* | −0.04 | −0.13* | — | |
| 16. Maternal education | 0.08* | 0.05 | 0.03 | 0.04 | −0.05 | −0.01 | 0.05 | 0.09* | −0.07* | 0.04 | −0.10* | −0.07 | −0.01 | −0.11* | 0.20* | — |
| M | 2.37 | 1.66 | 1.45 | 24.65 | 4.75 | 5.73 | 6.49 | 4.48 | 1.74 | 2.94 | 3.93 | 3.43 | 0.33a | 6.09 | 23.24 | 10.57 |
| SD | 0.91 | 0.96 | 1.22 | 8.35 | 1.41 | 1.53 | 1.46 | 1.42 | 1.55 | 0.99 | 1.52 | 3.72 | 0.47a | 6.26 | 3.99 | 2.79 |
| Skewness | 0.12 | 1.27 | 1.64 | 1.69 | 0.68 | 0.24 | 0.04 | 0.69 | 0.55 | 1.70 | 0.46 | 0.95 | 0.72a | 1.09 | 0.81 | 0.18 |
| Kurtosis | 0.97 | 0.29 | 3.84 | 1.47 | 0.00 | 0.40 | 0.29 | 0.40 | 0.81 | 3.90 | 0.45 | 0.13 | 1.48a | 0.44 | 1.02 | 1.49 |
Note. N = 871. SS = sensation seeking; IMP = poor impulse control; SU = substance use.
Any substance use by age 12 is a dichotomous measure, endorsed by 33% of boys.
p < .05.
Early substance use history
Any substance use by the age of 12 was assessed with a dichotomous variable identifying those adolescents who reported any alcohol, marijuana, or any other drug use by the age of 12 years, with 33% of boys in this sample reporting having tried a substance at least once by the age of 12. A dichotomous variable was used in preadolescence because of the low variability and high skewness of continuous substance use measures at this developmental period (data available for these boys from ages 10–12 years).
Early personality scores
A preadolescent proxy for sensation seeking was computed using items from the Jesness inventory (Jesness, 1983) at 10 and 11 years of age to assess whether pubertal development was associated with change in sensation seeking across early adolescence (i.e., once preadolescent sensation seeking was controlled for). Three items were identified that reflected sensation-seeking tendencies: “Some day I would like to drive a race car,” “It would be interesting to work in a carnival,” and “At night when I have nothing to do I like to go out and find a little excitement.” A composite score was created by summing these three items at 10 and 11 years (test–retest = .63; Cronbach’s α = .61, 6 items; interitem correlation = .21). Preadolescent poor impulse control was assessed at 12 years of age using items from the Social Behavior Questionnaire (Tremblay et al., 1991). Teachers were asked on a 3-point scale (never to often) whether the child (a) is restless, runs about, jumps up and down; (b) is squirmy or fidgety; (c) jumps from one activity to another; (d) is irritable and loses his temper easily; (e) attracts attention by shouting; (f) has trouble sitting still; (g) acts without thinking. Reliability was good for these items (α = .89; interitem correlation = .41).
Measures in childhood (covariates)
Sociodemographic information and childhood disruptive behaviors were entered as covariates, to control for some of the effects these variables can have in shaping future substance use problems (Lillehoj, Trudeau, Spoth, & Madon, 2005; Masse & Tremblay, 1997).
Boys’ childhood disruptive behavior was assessed using the teacher-rated Social Behavior Questionnaire (Tremblay et al., 1991), which included items on child’s aggression (three items), oppositional behavior (five items), and hyperactivity (two items) in kindergarten (at age 6; α = .93). When boys were 6 years of age, mothers were asked to complete sociodemographic information, which included questions on parents’ education level and their age when their first child was born. See Table 2 for correlations and descriptive statistics of all variables (including skewness and kurtosis).
Analysis
To test the assumption that both pubertal status and tempo can be modeled in boys, as well as the study’s hypotheses, four models or stages of analyses were conducted. First, a latent-growth curve model (LGCM) based on the modeling strategy used by Mendle et al. (2010) to examine pubertal status and tempo was conducted to examine pubertal development. One of the benefits of analyzing longitudinal data with LGCM is that it allows examining intraindividual change and interindividual differences in change across time (McArdle & Nesselroade, 2002). Once change in puberty was modeled, the LGCM for puberty was combined with substance use outcomes and covariates, as well as early substance use history (by age 12), into one multivariate model to test the relationship between pubertal development and substance use. This was followed by mediation analyses, in which indirect effects from potential mediators (sensation seeking, poor impulse control, and substance use frequency in early adolescence) were tested. Significance of indirect effects was tested using the product of coefficients method (sometimes referred to as the Delta method) recommended by MacKinnon et al. (MacKinnon, Lockwood, Hoffman, West, & Sheets, 2002; MacKinnon, Lockwood, & Williams, 2004). The product of coefficients of paths implicated in an indirect effect (e.g., pubertal status to sensation seeking [path a] and sensation seeking to substance use slope [path b]) are labeled “ab” in the text. The Sobel test was used to compute the standard errors of indirect effects. Finally, to test for moderation, interaction terms were created using model constraint in Mplus 5.21 (Muthén & Muthén, 1998–2009), which allows the creation of interaction terms between latent and observed variables and their inclusion in models testing indirect effects (Lau & Cheung, 2012). Interaction terms were created between impulse control and pubertal status, pubertal tempo, and sensation seeking, in the prediction of all substance use outcomes in mid to late adolescence. The method and results using “model constraint” to create the interactions are equivalent to the latent moderated structural equations (LMS) approach developed by Klein and Moosbrugger (2000).
All analyses were carried out using Mplus version 5.21 (Muthén & Muthén, 1998 to 2009). Maximum likelihood with robust standard errors (MLR) estimation was used in all analyses. MLR estimation differs from standard ML in the approach it uses to estimate standard errors. Although ML uses the second-order derivatives of the observed log-likelihood to estimate standard errors and depends on the assumption of normality, MLR is a sandwich estimator that uses both the first-order approximation of the asymptotic covariance matrix and the second-order derivatives of the observed log-likelihood to produce the correct asymptotic covariance matrix of the estimates that are not dependent on the assumption of normality (Kaplan, Kim, & Kim, 2009). Thus, compared with ML, MLR has been shown to perform better when modeling low prevalent behaviors or nonnormal data (Asparouhov & Muthén, 2005). Full information maximum likelihood (FIML) was used to account for missing data.
Tests of goodness of fit included the comparative fit index (CFI; Bentler, 1990), Tucker-Lewis index (TLI), root-mean-square error of approximation (RMSEA; Browne & Cudeck, 1993), and standardized root-mean residual (SRMR). Finally, The Benjamini-Hochberg procedure (Thissen, Steinberg, & Kuang, 2002) was used to correct for multiple testing in all analyses.
Results
Verifying Model Assumptions: Is There Significant Variability in Pubertal Status and Pubertal Tempo in Boys Across 11 and 13 Years?
First, to establish whether the boys in this sample demonstrated significant individual differences in change in pubertal development (pubertal status and tempo), a linear LGCM was conducted with pubertal scores from ages 11–13, and centered at 11 years. In this model, residual variances were constrained to be equal across time, with all other parameters in the model freely estimated. This model did not fit the data well, χ2(3, N = 871) = 42.14; CFI = 0.96; TLI = 0.96; RMSEA = .12; SRMR = .14, with modification indices indicating that model fit would substantially improve if the residual variance for the puberty score at 12 years was allowed to be freely estimated. Once the constraint on this residual variance was freed (while puberty scores at 11 and 13 years were still constrained to be equal), the linear latent growth curve model fit the data well according to all fit criteria, χ2(2, N = 871) = 1.00; CFI = 1.00; TLI = 1.00; RMSEA = .00; SRMR = .01 (see Figure 1). This model explained 65% of the variance in pubertal scores at 12 years (R2 = .65), and most of the variance in pubertal scores at 11 and 13 years (R2 = .98 for both; all at p < .001).
Figure 1.
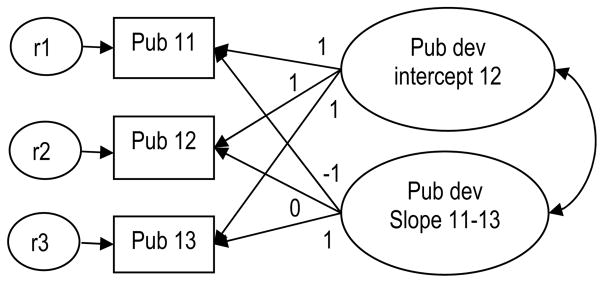
Univariate latent-growth model of self-reported puberty from 11 to 13 years, centered at 12 years. Pub dev = pubertal development; r = residual variance.
Growth curve factor means (i.e., intercept = 4.75; slope = 0.97) were all significantly different from zero at p < .001 and showed that there was an overall tendency for puberty to increase from 11 to 13 years of age. It is more important to note that the growth curve factor variances were also significant at p < .001 (i.e., intercept = 1.95; slope = 0.66), indicating that there was significant individual variability in the intercept and pattern of puberty change over time. The intercorrelation between these latent factors was high (r = −.50, p < .001), suggesting that the more developed or higher the pubertal score at 11 years, the lower the increase in pubertal scores across time (most likely due to ceiling effects). As these two latent factors were going to be entered as the main predictors in subsequent models, the high intercorrelation was of concern due to the potential of multicollinearity among these factors, which could affect the interpretability of findings. Thus, the intercept was recentered at the middle point (12 years), which reduced the intercorrelation between these factors (r = .08, p = .045). When centering the intercept of a linear growth curve at different time points, the model fit, mean and variance of the slope, and residual variances remain unchanged. Besides the intercorrelation between latent factors, the only other parameters that changed in the model were the mean and variance of the intercept, to reflect scores at the time point used to center the model (i.e., 12 years: M = 5.72, variance = 1.52, both at p < .001).
In these analyses, the latent intercept factor represents pubertal status, that is, higher scores on this variable represent greater maturation or higher pubertal scores at 12 years. The latent linear factor represents pubertal tempo, that is, high scores on this variable represent faster progress across pubertal stages (regardless of pubertal score reached by the age of 12 years). Inversely, lower scores on the slope represent slower progression through pubertal stages. It is important to note that lower scores could reflect slower progression either because boys had not begun puberty or because they had completed puberty. However, no boy in the current sample had completed pubertal development (stage 5), only 1% of the sample were prepubertal by age 13 (see Table 1), and only 47 boys (5% of the sample) showed no increases in pubertal scores from 11 to 13 years. Although these 47 boys would obviously score low on the slope, for the most part low scores on the slope represent the slow progression through stages one to four of pubertal development.
In summary, results showed that in this sample of boys there was significant variability in both the level of pubertal score in preadolescence (equivalent to the intercept), conceptualized here as pubertal status, and in change in pubertal scores across time (slope), conceptualized here as pubertal tempo.
Testing Hypothesis 1: Do Status and Tempo of Puberty Predict Substance Use in Mid to Late Adolescence?
The univariate growth model for puberty, described above, was included in a model with the substance use outcomes (alcohol frequency, marijuana frequency, and no. of drugs tried and substance use problems at 15–16 years), to test the relationship between pubertal status at age 12 and pubertal tempo and substance use across adolescence, controlling for childhood disruptiveness, demographic variables (age of mother at the birth of her first child and mother’s education) and preadolescent substance use history (by age 12). Thus, regression paths from the intercept and linear slope latent factors for puberty to these self-reported substance use variables were included in this model. This model fit the data well, χ2(19, N = 871) = 29.87; CFI = 1.00; TLI = .99; RMSEA = .03; SRMR = .02. Table 3 (Model I) shows regression coefficients from puberty intercept and slope variables to substance use outcomes. Results indicated that, controlling for preadolescent substance use history and covariates, pubertal status at age 12 (intercept) significantly predicted all substance use outcomes, whereas pubertal tempo significantly predicted marijuana use frequency, number of drugs tried, and substance use problems at 15–16 years. Covariates and variables assessed within the same developmental period (e.g., preadolescence and mid–late adolescence) were allowed to covary. In this model, any substance use history by the age of 12 significantly correlated with pubertal status at age 12 (r = .14, p < .001) but not pubertal tempo (r = −.03, p = .46).
Table 3.
Puberty and Mediators Predicting Substance Use in Mid to Late Adolescence
| Alcohol use freq at 15–16 years
|
Marijuana use freq at 15–16 years
|
No. of drugs at 15–16 years
|
SU problems at 15–16 years
|
|||||
|---|---|---|---|---|---|---|---|---|
| B | SE | B | SE | B | SE | B | SE | |
| Model I | ||||||||
| Puberty intercept | .16*** | .04 | .11*** | .04 | .13** | .03 | .16*** | .03 |
| Puberty slope | .06 | .04 | .08* | .04 | .10** | .04 | .08* | .04 |
| Model II | ||||||||
| Puberty intercept | .07* | .03 | .04 | .03 | .05 | .03 | .08* | .03 |
| Puberty slope | .05 | .03 | .08* | .03 | .10** | .03 | .08* | .03 |
| Sensation seeking at 13–14 | .13*** | .03 | .07 | .04 | .08* | .03 | .08** | .03 |
| IMP at 13–14 | .07* | .03 | .09* | .04 | .11** | .03 | .12** | .03 |
| SU frequency at 13–14 | .49*** | .03 | .41*** | .04 | .43*** | .03 | .46*** | .04 |
| Model III | ||||||||
| Puberty intercept × IMP | −.019 | .015 | −.029 | .017 | −.017 | .022 | −.212 | .316 |
| Puberty slope × IMP | .023 | .022 | .014 | .026 | .017 | .032 | −.097 | .413 |
| Sensation-seeking × IMP | −.028 | .018 | .040* | .020 | .033 | .020 | .379 | .325 |
Note. IMP = poor impulse control. Standardized coefficients are reported for Models I and II; unstandardized coefficients are reported for interaction terms in Model III. Puberty scores were used in the modeling of puberty intercept and slope. Effects are controlled for boys’ substance use history by age 12 and disruptiveness in childhood, age of mother at the birth of her 1st child, and mother’s education (Models I, II, & III), and Jesness sensation seeking at 10 –11 years and teacher-rated impulse-control problems at 12 years (Models II & III only). (The Benjamini-Hochberg procedure was used to correct for multiple testing) Model fit for Model I: χ2(19, N = 871) = 29.87; CFI = 1.00; TLI = .99; RMSEA = .03; SRMR = .02; Model II: χ2(51, 871) = 151.17; CFI = .97; TLI = .94; RMSEA = .05; SRMR = .04. In Model I, pubertal timing (r = .14, p < .001), but not pubertal tempo (r = −.03, p = .46), significantly correlated with substance use history by the age of 12; Substance use by the age of 12 significantly predicted alcohol use frequency (β = .25, p < .001), marijuana use frequency (β = .16, p < .001), no. of drugs (β = .20, p < .001), and substance use problems (β = .23, p < .001) at 15–16 years. In Model II, pubertal timing was significantly associated with sensation seeking (β = .10, p < .05) and substance use frequency (β = .15, p < 001), but not impulsivity (β = .01, p = .80) in mid adolescence. Pubertal tempo was not significantly associated with any personality or substance use outcomes in early adolescence (all ps > .36). In all models, variables assessed within the same developmental period (e.g., preadolescence, early adolescence, and mid–late adolescence) were allowed to covary.
p < .05.
p < .01.
p < .001.
Testing Hypothesis 2a: Does Sensation-Seeking Explain the Association Between Pubertal Status and Substance Use in Mid to Late Adolescence?
Potential indirect effects from pubertal development to substance use in mid to late adolescence through personality characteristics were examined by including adolescent self-reported personality into the previously described model. A measure of substance use in early adolescence (i.e., substance use frequency at 13–14 years) was also entered into the model, along with personality characteristics, for two reasons: (a) to test whether personality characteristics in early adolescence predicted substance use later in adolescence even after accounting for substance use in early adolescence; and (b) to test whether the effects pubertal status at age 12 and pubertal tempo had on substance use in mid to late adolescence could be explained by more proximal effects on substance use in early adolescence. Thus, regression paths leading from puberty status at age 12 and pubertal tempo to self-reported sensation seeking, poor impulse control and substance use frequency at 13–14 years, and from these measures to substance use outcomes, were included in the model. Also, in an attempt to control for early, preadolescent sensation seeking and poor impulse-control tendencies, self-reported sensation seeking as measured by items from the Jesness inventory (averaged across ages 10 and 11 years) and teacher-reported poor impulse control (at 12 years) were included in the model. See Figure 2 for all variables included in this model by developmental stage (preadolescence, early adolescence, mid–late adolescence). This model fit the data well, χ2(51, 871) = 151.17; CFI = .97; TLI = .94; RMSEA = .05; SRMR = .04.
Figure 2.

All variables included in the final mediation model (Model II), with significant direct paths from pubertal development to substance use outcomes in mid–late adolescence, as well as indirect paths through early adolescent variables, highlighted. Other significant direct effects across time are shown with broken arrows without coefficients. IMP = poor impulse control; SS = sensation seeking; SU = substance use; Pub dev = pubertal development based on puberty scores. Other significant longitudinal paths (shown with broken arrows in figure) were: Any substance use by 12 years was associated with SU frequency at 13–14 (β = .40, p < .001), SS at 13–14 (β = .12, p < .001), and IMP at 13–14 (β = .13, p < .001); Sensation-seeking proxy at 10 –11 years (Jesness) was significantly associated with sensation seeking at 13–14 (β = .18, p < .001); Teacher-rated impulsivity at 12 years was significantly associated with IMP at 13–14 (β = .16, p < .001) and SU frequency at 13–14 (β = .10, p < .01); IMP at 13–14 years was significantly associated with alcohol use frequency at 15–16 (β = .07, p < .05), marijuana use frequency at 15–16 (β = .09, p < .05), drugs tried at 15–16 (β = .11, p < .01), and SU problems at 15–16 (β = .12, p < .01). Although only significant paths and correlations are shown, covariates were regressed on mid to late adolescent variables, and all variables assessed within the same developmental period were allowed to covary. All paths and covariances modeled are shown in Table S1 in the online Supplementary materials.
Main effects
Results showed that substance use frequency in early adolescence strongly predicted all substance use outcomes in mid to late adolescence (βs ranged between .41 and .49). Even after controlling for these strong effects and correcting for multiple testing, early adolescent self-reported poor impulse control and sensation seeking at 13–14 years significantly predicted a higher number of drugs tried and substance use problems in mid–late adolescence, and more frequent alcohol use at 15–16 years (see Table 3, Model II). Poor impulse control, but not sensation seeking, at 13–14 years predicted more frequent marijuana use at 15–16 years. Results also showed that, after taking into account early adolescent personality and substance use measures, pubertal status at age 12 only predicted mid to late adolescence alcohol use frequency and substance use problems. In contrast, the effect of pubertal tempo on marijuana use frequency, number of drugs tried, and substance use problems in mid to late adolescence at 15–16 years was unchanged with the inclusion of early adolescent variables. Furthermore, pubertal status at age 12 was significantly associated with sensation seeking at 13–14 years (β = .10, p < .05), even after controlling for the significant preadolescent effects that sensation seeking at 10 –11 years (Jesness, β = .18, p < .001) and early substance use history (by age 12, β = .12, p < .001) had on early adolescent sensation seeking at 13–14 years (teacher-rated impulse-control at age 12 did not significantly predict sensation seeking at ages 13–14 years, β = .05, p = .15). In this model, pubertal status at age 12 also significantly predicted substance use frequency in early adolescence at ages 13–14 years (β = .15, p < .001) but not poor impulse control (β = .01, p = .80), ruling out poor impulse control as a putative mediator of pubertal status at age 12. Pubertal tempo did not predict any of the key variables in early adolescence: sensation seeking (β = −.03, p = .36), poor impulse control (β = −.01, p = .67), or substance use frequency (β = .03, p = .47), ruling them all out as putative mediators of pubertal tempo. See Figure 2 for other significant associations between variables across developmental stages (e.g., preadolescence and early adolescence). Of note are findings showing that preadolescent substance use history by age 12 predicted higher sensation seeking and lower impulse control in early adolescence, and that personality measures in preadolescence and early adolescence predicted higher substance use measures at later time points, suggesting that the effects of substance use and personality are bidirectional or reciprocal across time.
Indirect effects
Figure 2 shows that significant indirect effects through substance use frequency in early adolescence at 13–14 years were found between pubertal status at age 12 and all substance use outcomes in mid to late adolescence: alcohol use frequency (unstandardized ab = .051, SE = 0.012, p < .001; standardized ab = .071), marijuana use frequency (unstandardized ab = .046, SE = 0.012, p < .001; standardized ab = .060), number of drugs tried (unstandardized ab = .061, SE = 0.015, p < .001; standardized ab = .062), and substance use problems (unstandardized ab = .888, SE = 0.222, p < .001; standardized ab = .067). Closer to our hypothesis, we found significant indirect effects through sensation seeking in early adolescence between pubertal status at age 12 and alcohol use frequency (unstandardized ab = .009, SE = 0.004, p < .05; standardized ab = .013), number of drugs tried (unstandardized ab = .008, SE = 0.003, p < .05; standardized ab = .008), and substance use problems (unstandardized ab = .110, SE = 0.054, p < .05; standardized ab = .008). Table 3 (Model II) shows that a substantial proportion of the total effects from pubertal status at age 12 to alcohol use frequency (56%), marijuana frequency (64%), number of drugs tried (62%) and substance use problems (50%) were mediated by substance use and sensation seeking in early adolescence. Of the mediated effects from pubertal status at age 12 to alcohol use frequency, number of drugs tried, and to substance use problems, the indirect effects through sensation seeking accounted, respectively, for 14%, 11%, and 18% of the mediated effect.
Testing Hypothesis 2b: Does Poor Impulse-Control Moderate the Association Between Pubertal Development, Sensation Seeking, and Substance Use During Adolescence?
Analyses were finally conducted to test whether self-reported poor impulse control at 13–14 years moderated the effects of pubertal development and sensation seeking on substance use behaviors in mid to late adolescence. To test this hypothesis, interaction terms were created between poor impulse control and pubertal status at age 12, pubertal tempo, and sensation seeking, in the prediction of all substance use outcomes. This model (Model III) fit the data marginally better than the previous model (model II, same model but with no interactions; log-likelihood ratio = 20.12, Δdf = 12, p = .064), suggesting the presence of a significant interaction. Table 3 (Model III) shows the effects (unstandardized coefficients) of these interactions on substance use outcomes in mid to late adolescence. Only the interaction between sensation seeking and poor impulse control in the prediction of marijuana use frequency was significant, showing that sensation seeking was associated with higher marijuana use only at low levels of impulse control (see Figure 3).
Figure 3.
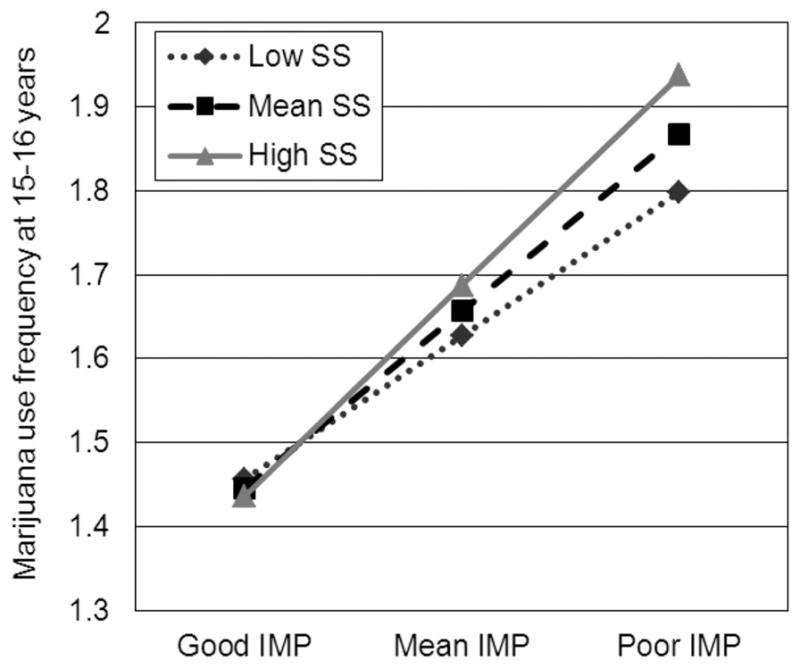
Marijuana use frequency at 15–16 years by sensation seeking (SS) and impulse control (IMP) at 13–14 years.
Discussion
This study highlights that individual differences not only in pubertal status (i.e., level of pubertal development reached by the age of 12) but also in pubertal tempo (i.e., how quickly children progress through pubertal stages between 11 to 13 years) are important factors in the onset and increase in substance use in adolescent boys. Although there was already evidence that boys whose pubertal status was ahead of others also reported higher rates of substance use across adolescence, this longitudinal study extends these findings by showing the importance of pubertal status for the development of substance use problems in adolescence. This is important as adolescent substance use problems have been shown to be strongly associated with substance use disorders in adulthood (e.g., Rohde et al., 2001) and, thus, thought to be a clearer sign of clinical difficulties than adolescent substance use quantity or frequency. It also revealed the important role of pubertal tempo. More specifically, the faster boys progressed through puberty, the greater the marijuana use frequency, number of drugs tried and substance use problems. Although there had been earlier suggestions to examine how rate of change in puberty was related to substance use in early adolescence (Dick et al., 2001), this study is the first to show specific association between pubertal tempo and substance use in adolescent boys.
These are important findings as very few studies on pubertal development are conducted in boys, and those that do, have yielded inconsistent findings. Our findings, together with those of Mendle et al. (2010) in their study of depression, provide support for the maturation compression hypothesis and suggest that a more comprehensive account of pubertal maturation that moves beyond a simple consideration of timing or status is needed to understand its association with substance use and other psychopathology. In addition, findings showing that both pubertal status and tempo were associated with substance use problems in boys add to the growing literature indicating that the previous perspective suggesting that early or more advanced maturation in boys is generally associated with positive social, emotional, and behavioral outcomes is in need of revision (Ge et al., 2001).
Moreover, this study clarifies the role of two related but distinct personality traits in the puberty–substance use link. The level of pubertal development reached by 12 years was significantly associated with sensation seeking but not with poor impulse control, which is consistent with previous findings (Martin et al., 2002; Steinberg et al., 2008). Further, pubertal tempo was not associated with sensation seeking (or poor impulse control). Together these findings suggest that it is pubertal status, rather than the rate of progression across stages of puberty, which may be driving increases in sensation seeking in early adolescence. Thus, there would be at least two distinct developmental pathways by which pubertal maturation affects adolescent substance use: one characterized by differences in the level of pubertal maturation at a particular age (e.g., by age 12), which is indirectly associated with substance use partly through increases in sensation seeking and another characterized by fast pubertal tempo, which is independent from personality. These independent pathways support both the maturational disparity and maturational compression hypotheses, suggesting that being more mature than your peers in preadolescence as well as experiencing a fast progression through pubertal development both demand a quick adaptation to not only the biological but social milestones that characterize puberty.
In our study, the small effect sizes and the fact that sensation seeking only partially mediated the associations between pubertal status and alcohol use frequency, substance experimentation, and problems, suggests that other factors may be important in explaining these links. Potential social factors mediating these effects were clarified in a recent study by Mendle, Harden, Brooks-Gunn, and Graber (2012), which suggests the possibility that the pathways from pubertal status and tempo to emotional and behavioral problems may be at least partly explained by social mechanisms such as peer relationships, at least for depression. Aside from poor peer relationships (Mendle et al., 2012) and affiliation with more deviant peers (e.g., Patton et al., 2004), another factor identified in the literature that could potentially explain this link is the rise in adrenal and gonadal hormones during puberty, which have effects on other brain regions like the hypothalamus and sensory and association regions of the brain (e.g., Angold et al., 1999). That said, the finding identifying sensation seeking as a factor that partially explained the link between pubertal status at 12 years and substance use in adolescence provides some indirect support for the dual-systems model. According to this model, risky behavior during puberty and early adolescence increases due to the relatively rapid development of the socioemotional brain system, which brings with it increased levels of dopaminergic activity, and leads, in turn, to increased sensation seeking during this period (Steinberg, 2008).
The dual-systems model also posits that the cognitive control brain system, involved in impulse control and regulation, matures more gradually during adolescence relative to the rapid development of the socioemotional system. This maturational gap is hypothesized to lead to increased vulnerability to risk-taking behaviors, such as substance use. Thus, we had hypothesized that vulnerability to adolescent substance use would increase as a function of poor impulse control. Our findings are in agreement with this hypothesis insofar as we show that impulse control significantly moderated the association between sensation seeking and marijuana use frequency in mid to late adolescence. Specifically, higher sensation-seeking scores significantly predicted more frequent marijuana use only at low levels of impulse control. Thus, these results lend some support to the idea that the unique association between sensation seeking and frequent marijuana use in boys increases with poor impulse control. However, poor impulse control did not significantly moderate the link between sensation seeking and other substance use outcomes, or the link between substance use outcomes and pubertal status and tempo, as hypothesized. The fact that most of the effects reported in the current study are small in size gives rise to the possibility that the lack of other significant moderation results could stem from being underpowered.
Therefore the current findings provide support for the maturational disparity and compression hypotheses, but only partial and indirect support for the dual-systems model, and do not completely discount other models that attempt to explain the link between early pubertal development and risky behavior, behavioral problems, or both, during adolescence. For example, some authors have suggested that pubertal development may not be the “trigger” initiating adolescents in substance use, but rather that puberty may exacerbate previous individual differences in psychosocial functioning (Caspi & Moffitt, 1991). Sometimes referred to as the “accentuation hypothesis,” this model suggests that preexisting individual differences, such as poor impulse control, may make some adolescents vulnerable to negative behavioral outcomes during puberty, as the stress associated with the transition to adolescence makes individual differences more pronounced. Although not directly tested in this study, our findings do not rule out this model (which is still compatible with the maturational disparity and compression hypotheses, and dual-systems model). A fuller test of these relevant models would require sensation seeking and poor-impulse control, or other indices of the socioemotional and cognitive control systems, to be assessed and modeled longitudinally and interactively so that the joint trajectories of these two systems and consequently of the maturational gap can be more accurately examined. Relatedly, the main limitation to this study is the lack of longitudinal personality data, that is, the use of different measures for pre- and postpubertal sensation seeking and poor impulse control (e.g., although there is some overlap between items, the preadolescent measure of poor impulse control represents mostly hyperactive tendencies, whereas the adolescent measure of poor impulse control represents mostly lack of planning and urgency), as well as the inclusion of only two time points. We were, thus, unable to model the development of impulse control and sensation seeking across adolescence and test whether these traits increased, decreased, or remained stable during adolescence in this sample of boys. However, results showed that early maturation was significantly associated with the early adolescence (age 13–14) mean sensation-seeking score, suggesting that changes in sensation seeking over time reported in previous studies (e.g., Lynne-Landsman, Graber, Nichols, & Botvin, 2011; Zuckerman, 2007) may be associated with pubertal maturation, its biological and social correlates, or both.
A second limitation is that specific correlates of pubertal tempo which have also been shown to predict substance use problems were not included in the models tested. One example could be adverse parent– child relationship. Not only has adverse parent–child relationship been associated with fast pubertal tempo in early adolescence (Ellis, 2004; Ellis et al., 2011), but also with personality and substance use disorders in adulthood (Brook, Brook, Zhang. & Cohen, 2009). Future studies should examine the role of adverse parent– child relationship in the link between pubertal tempo and substance use, and the potential reciprocal effects between pubertal tempo, parent– child relationship and substance use across development.
A third limitation is that all data presented in this study, except for childhood disruptiveness and poor impulse control at 12 years, were gathered through self-report, which is susceptible to bias and may limit the experimental validity of the data. This said, several studies have shown that self-reports are reliable when assessing personality (e.g., De Fruyt, Mervielde, Hoekstra, & Rolland, 2000), as well as substance use or other behavioral problems in adolescence (Clark & Winters, 2002; Crowley, Mikulich, Ehlers, Whitmore, & MacDonald, 2001), and hence are useful for clinical practice and research. This, together with guaranteed confidentiality to participants, should contribute to the reliability and validity of these data. Pubertal development was also self-reported, so the self-perception of pubertal development rather than actual pubertal development was assessed. However, the Pubertal Development Scale is widely used and has been shown to possess good reliability and validity in boys as well as girls (Arim et al., 2007; Bond et al., 2006; Petersen et al., 1988; Schmitz et al., 2004).
A fourth limitation is that this study investigated pubertal development across 3 years, from 11 to 13 years of age. Although three time points across this age span are sufficient to capture linear pubertal tempo, they do not allow capturing quadratic growth (or the decreasing trend in growth experienced as pubertal development nears completion). Ideally, future studies should model pubertal development from middle childhood to mid to late adolescence to capture the full spectrum of pubertal development. Relatedly, most boys (79%) reported pubertal onset before the age of 11 years. Thus, these data do not capture and, thus, cannot be generalizable to very early maturing boys. It is more important to note that because of this, this study was unable to test the effects of the timing of pubertal onset and instead used the level or stage of pubertal development reached by the age of 12 years as a measure of pubertal status. It would be important for future research to test the effects of timing of pubertal onset and test whether the findings reported here can be replicated. Finally, the current sample was made up entirely of French-speaking boys of European American origin living in low SES neighborhoods in Montreal. Thus, replication of these findings in girls and more diverse populations are needed to establish the generalizability of these findings. Despite these limitations, the present findings provide support for considering not only pubertal status but also pubertal tempo when examining individual differences in pubertal maturation and their association with emotional and behavioral outcomes in boys. Although it is clear that risk taking is for the most part normative during adolescence, it is also clear that adolescents vary in their maturation and in their impulse-control and sensation seeking, all of which are associated with increased levels of substance use and problems and possibly risky behaviors in general.
The current findings have implications for the refinement of evidence-based clinical intervention and prevention approaches. Selective approaches targeting pubertal and personality liability factors in childhood or early adolescence rather than the behavior or problems later in adolescence, have shown very promising results. For example, one approach that targets disruptive behaviors and impulse control in childhood has been shown to have long-term effects on adolescent substance use (e.g., Castellanos-Ryan, Séguin, Vitaro, Parent & Tremblay (accepted); Castellanos-Ryan, O’Leary-Barrett, & Conrod, 2013; Stormshak et al., 2011; van Lier, Huizink, & Crijnen, 2009; Zonnevylle-Bender, Matthys, van de Wiel, & Lochman, 2007). A second promising selective approach is a personality-based model targeting four personality risk factors for early onset drinking or illicit drug use in early adolescence, including impulse control and sensation seeking. This school-based program has now been shown to prevent adolescent alcohol and substance misuse in three separate trials across Canada (Conrod, Stewart, Comeau, & Maclean, 2006) and the United Kingdom (Conrod, Castellanos, & Mackie, 2008; Conrod, Castellanos-Ryan, & Mackie, 2011; Conrod et al., 2010; O’Leary-Barrett, Mackie, Castellanos-Ryan, Al-Khudhairy, & Conrod, 2010). In this way, implementing targeted clinical interventions prior to initial exposure to drugs prevents or reduces the adverse impact from substance use on the developing brain and other potential harms, as well as reduces some of the huge financial costs of addiction treatment in adulthood. There are also now a number of school-based interventions targeting the risk presented by early pubertal timing that are showing some beneficial effects (e.g., Botvin, Griffin, & Nichols, 2006; Eddy, Reif, & Fetrow, 2000). The current findings raise the possibility that one could reduce the known vulnerability presented by a more advanced pubertal status on boy’s adolescent substance use and problems by targeting sensation seeking and poor impulse control in early adolescence (or even in late childhood). Moreover, the current findings suggest that these interventions could be further enhanced by adding a component that would address individual variability not only in pubertal timing or status but also in tempo. This added component would specifically target the stress and adaptation required to cope with the greater rapidity of changes linked to puberty that some youth face, making these interventions more relevant and effective for boys. It is estimated that rates of adult substance abuse and dependence could be reduced by up to 10% with every year that onset of substance use is delayed in adolescence (Grant & Dawson, 1998). Thus, delaying early onset of substance use or preventing problematic use is particularly important, and understanding the mechanisms by which variation in these factors are associated with substance use, as we have shown, can inform clinical prevention and intervention strategies.
Supplementary Material
Acknowledgments
We thank the boys, their families, and teachers for their long-term commitment to this project. We also wish to thank Lyse Desmarais-Gervais, Hélène Beaumont, Charles-Édouard Giguère, the many research assistants, and the Research Unit on Children’s Psychosocial Maladjustment staff. This research was made possible by Fellowship 149169 to NC-R from The Fonds Québécois de la Recherche sur la Nature et les Technologies, grants from the Canadian Institutes of Health Research (MOP-97910), the Social Science and Humanities Research Council of Canada, the National Health Research and Development Program, the Fonds Québécois de Recherche sur la Société et la Culture, and the Fonds Québécois de Recherche en Santé. These Funding agencies had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication.
Footnotes
The authors report no potential conflicts of interest.
Contributor Information
Natalie Castellanos-Ryan, Department of Psychiatry, Université de Montréal, Quebec, Canada, and CHU Ste-Justine Research Center, Montreal, Quebec, Canada.
Sophie Parent, Department of Psychoeducation, Université de Montréal, Quebec, Canada.
Frank Vitaro, CHU Ste-Justine Research Center, Montreal, Quebec, Canada, and Department of Psychoeducation, Université de Montréal, Quebec, Canada.
Richard E. Tremblay, Departments of Psychology and Pediatrics, Université de Montréal, Quebec, Canada; School of Public Health and Population Sciences, University College Dublin, Ireland
Jean R. Séguin, Department of Psychiatry, Université de Montréal, Quebec, Canada, and CHU Ste-Justine Research Center, Montreal, Quebec, Canada
References
- Arim RG, Shapka JD, Dahinten VS, Willms JD. Patterns and correlates of pubertal development in Canadian youth: Effects of family context. Canadian Journal of Public Health Revue canadienne de santé publique. 2007;98:91–96. doi: 10.1007/BF03404316. Retrieved from http://journal.cpha.ca/index.php/cjph/index. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Asparouhov T, Muthén B. Multivariate statistical modeling with survey data. Paper presented at the Federal Committee on Statistical Methodology (FCSM) Research Conference; Arlington, VA. 2005. Nov, [Google Scholar]
- Belin D, Mar AC, Dalley JW, Robbins TW, Everitt BJ. High impulsivity predicts the switch to compulsive cocaine-taking. Science. 2008;320:1352–1355. doi: 10.1126/science.1158136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belsky J, Steinberg L, Houts RM, Friedman SL, DeHart G, Cauffman E NICHD Early Child Care Research Network. Family rearing antecedents of pubertal timing. Child Development. 2007;78:1302–1321. doi: 10.1111/j.1467-8624.2007.01067.x. [DOI] [PubMed] [Google Scholar]
- Bentler PM. Comparative fit indexes in structural models. Psychological Bulletin. 1990;107:238–246. doi: 10.1037/0033-2909.107.2.238. [DOI] [PubMed] [Google Scholar]
- Bond L, Clements J, Bertalli N, Evans-Whipp T, McMorris BJ, Patton GC, Catalano RF. A comparison of self-reported puberty using the Pubertal Development Scale and the Sexual Maturation Scale in a school-based epidemiologic survey. Journal of Adolescence. 2006;29:709–720. doi: 10.1016/j.adolescence.2005.10.001. [DOI] [PubMed] [Google Scholar]
- Botvin GJ, Griffin KW, Nichols TR. Preventing youth violence and delinquency through a universal school-based prevention approach. Prevention Science. 2006;7:403– 408. doi: 10.1007/s11121-006-0057-y. [DOI] [PubMed] [Google Scholar]
- Brook JS, Brook DW, Zheng C, Cohen P. Pathways from adolescent parent-child conflict to substance use disorders in the fourth decade of life. The American Journal on Addictions. 2009;18:235–242. doi: 10.1080/10550490902786793. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Browne MW, Cudeck R. Alternative ways of assessing model fit. In: Bollen KA, Long JS, editors. Testing structural equation modeling. Thousand Oaks, CA: Sage; 1993. pp. 136–162. [Google Scholar]
- Canals J, Vigil-Colet A, Chico E, Marti-Henneberg C. Personality changes during adolescence: The role of gender and pubertal development. Personality and Individual Differences. 2005;39:179–188. doi: 10.1016/j.paid.2004.12.012. [DOI] [Google Scholar]
- Caspi A, Moffitt TE. Individual differences are accentuated during periods of social change: The sample case of girls at puberty. Journal of Personality and Social Psychology. 1991;61:157–168. doi: 10.1037/0022-3514.61.1.157. [DOI] [PubMed] [Google Scholar]
- Castellanos-Ryan N, Conrod PJ. Personality correlates of the common and unique variance across conduct disorder and substance misuse symptoms in adolescence. Journal of Abnormal Child Psychology. 2011;39:563–576. doi: 10.1007/s10802-010-9481-3. [DOI] [PubMed] [Google Scholar]
- Castellanos-Ryan N, Conrod PJ. Personality and substance misuse: Evidence for a four-factor model of vulnerability. In: Verster J, Brady K, Galanter M, Conrod PJ, editors. Drug abuse and addiction in medical illness: Causes, consequences and treatment. Totowa, NJ: Humana/Springer Press; 2012. pp. 47–62. [DOI] [Google Scholar]
- Castellanos-Ryan N, O’Leary-Barrett M, Conrod PJ. Substance-use in childhood and adolescence: A brief overview of developmental processes and their clinical implications. Journal of the Canadian Academy of Child and Adolescent Psychiatry. 2013;22:41– 46. Retrieved from www.cacap-acpea.org. [PMC free article] [PubMed] [Google Scholar]
- Castellanos-Ryan N, Séguin JR, Vitaro F, Parent S, Tremblay RE. A multimodal intervention for disruptive kindergarten children reduces substance-use across adolescence: A randomized control trial. British Journal of Psychiatry. doi: 10.1192/bjp.bp.112.123182. (accepted) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chassin L, Dmitrieva J, Modecki K, Steinberg L, Cauffman E, Piquero AR, Losoya SH. Does adolescent alcohol and marijuana use predict suppressed growth in psychosocial maturity among male juvenile offenders? Psychology of Addictive Behaviors. 2010;24:4841– 60. doi: 10.1037/a0017692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark DB, Winters KC. Measuring risks and outcomes in substance use disorders prevention research. Journal of Consulting and Clinical Psychology. 2002;70:1207–1223. doi: 10.1037/0022-006X.70.6.1207. [DOI] [PubMed] [Google Scholar]
- Conrod PJ, Castellanos N, Mackie C. Personality-targeted interventions delay the growth of adolescent drinking and binge drinking. Journal of Child Psychology and Psychiatry. 2008;49:181–190. doi: 10.1111/j.1469-7610.2007.01826.x. [DOI] [PubMed] [Google Scholar]
- Conrod PJ, Castellanos-Ryan N, Mackie C. Long-term effects of personality-targeted interventions to reduce alcohol misuse in adolescents. Journal of Consulting and Clinical Psychology. 2011;79:296–306. doi: 10.1037/a0022997. [DOI] [PubMed] [Google Scholar]
- Conrod PJ, Castellanos-Ryan N, Strang J. Brief, personality-targeted coping skills interventions and survival as a non-drug user over a 2-year period during adolescence. Archives of General Psychiatry. 2010;67:85–93. doi: 10.1001/archgenpsychiatry.2009.173. [DOI] [PubMed] [Google Scholar]
- Conrod PJ, Stewart SH, Comeau N, Maclean AM. Preventative efficacy of cognitive behavioral strategies matched to the motivational bases of alcohol misuse in at-risk youth. Journal of Clinical Child and Adolescent Psychology. 2006;35:550–563. doi: 10.1207/s15374424jccp3504_6. [DOI] [PubMed] [Google Scholar]
- Costello EJ. Psychiatric predictors of adolescent and young adult drug use and abuse: What have we learned? Drug and Alcohol Dependence. 2007;88(Suppl 1):S97–99. doi: 10.1016/j.drugalcdep.2006.12.027. [DOI] [PubMed] [Google Scholar]
- Crowley TJ, Mikulich SK, Ehlers KM, Whitmore EA, MacDonald MJ. Validity of structured clinical evaluations in adolescents with conduct and substance problems. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40:265–273. doi: 10.1097/00004583-200103000-00005. [DOI] [PubMed] [Google Scholar]
- Curran PJ, West SG, Finch JF. The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychological Methods. 1996;1:16–29. doi: 10.1037/1082-989X.1.1.16. [DOI] [Google Scholar]
- De Fruyt F, Mervielde I, Hoekstra HA, Rolland JP. Assessing adolescents’ personality with the NEO–PI–R. Assessment. 2000;7:329–345. doi: 10.1177/107319110000700403. [DOI] [PubMed] [Google Scholar]
- Dick DM, Rose RJ, Pulkkinen L, Kaprio J. Measuring puberty and understanding its impact: A longitudinal study of adolescent twins. Journal of Youth and Adolescence. 2001;30:385–399. doi: 10.1023/A:1010471015102. [DOI] [Google Scholar]
- Dubé G, Bordeleau M, Cazale L, Fournier C, Traoré I, Plante N, Camirand J. Enquête québécoise sur le tabac, l’alcool, la drogue et le jeu chez les élèves du secondaire, 2008. Québec, Ontario, Canada: Institut de la statistique du Québec; 2009. [Google Scholar]
- Eddy JM, Reid JB, Fetrow RA. An elementary school based prevention program targeting modifiable antecedents of youth delinquency and violence: Linking the Interests of Families and Teachers (LIFT) Journal of Emotional and Behavioral Disorders. 2000;8:165–176. doi: 10.1177/106342660000800304. [DOI] [Google Scholar]
- Ellis BJ. Timing of pubertal maturation in girls: An integrated life history approach. Psychological Bulletin. 2004;130:920–958. doi: 10.1037/0033-2909.130.6.920. [DOI] [PubMed] [Google Scholar]
- Ellis BJ, Shirtcliff EA, Boyce WT, Deardorff J, Essex MJ. Quality of early family relationships and the timing and tempo of puberty: Effects depend on biological sensitivity to context. Development and Psychopathology. 2011;23:8516–99. doi: 10.1017/S0954579410000660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eysenck SBG, Easting G, Pearson PR. Age norms for impulsiveness, venturesomeness and empathy in children. Personality and Individual Differences. 1984;5:315–321. doi: 10.1016/0191-8869(84)90070-9. [DOI] [Google Scholar]
- Eysenck SB, Eysenck HJ. Impulsiveness and venturesomeness: Their position in a dimensional system of personality description. Psychological Reports. 1978;43:1247–1255. doi: 10.2466/pr0.1978.43.3f.1247. [DOI] [PubMed] [Google Scholar]
- Felson RB, Haynie DL. Pubertal development, social factors, and delinquency among adolescent boys. Criminology. 2002;40:967–988. doi: 10.1111/j.1745-9125.2002.tb00979.x. [DOI] [Google Scholar]
- Finn PR, Sharkansky EJ, Brandt KM, Turcotte N. The effects of familial risk, personality, and expectancies on alcohol use and abuse. Journal of Abnormal Psychology. 2000;109:122–133. doi: 10.1037/0021-843X.109.1.122. [DOI] [PubMed] [Google Scholar]
- Ge X, Conger RD, Elder GH., Jr Pubertal transition, stressful life events, and the emergence of gender differences in adolescent depressive symptoms. Developmental Psychology. 2001;37:404– 417. doi: 10.1037/0012-1649.37.3.404. [DOI] [PubMed] [Google Scholar]
- Ge X, Jin R, Natsuaki MN. In search of explanations for early pubertal timing effects on developmental psychopathology. Current Directions in Psychological Science. 2009;18:327–331. doi: 10.1111/j.1467-8721.2009.01661.x. [DOI] [Google Scholar]
- Ge X, Jin R, Natsuaki MN, Gibbons FX, Brody GH, Cutrona CE, Simons RL. Pubertal maturation and early substance use risks among African American children. Psychology of Addictive Behaviors. 2006;20:404– 414. doi: 10.1037/0893-164X.20.4.404. [DOI] [PubMed] [Google Scholar]
- Grant BF, Dawson DA. Age of onset of drug use and its association with DSM–IV drug abuse and dependence: Results from the national longitudinal alcohol epidemiologic survey. Journal of Substance Abuse. 1998;10:163–173. doi: 10.1016/S0899-3289(99)80131-X. [DOI] [PubMed] [Google Scholar]
- Gunn RL, Smith GT. Risk factors for elementary school drinking: Pubertal status, personality, and alcohol expectancies concurrently predict fifth grade alcohol consumption. Psychology of Addictive Behaviors. 2010;24:617– 627. doi: 10.1037/a0020334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harden KP, Mendle J. Gene environment interplay in the association between pubertal timing and delinquency in adolescent girls. Journal of Abnormal Psychology. 2012;121:731247– 87. doi: 10.1037/a0024160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harden KP, Tucker-Drob EM. Individual differences in the development of sensation seeking and impulsivity during adolescence: Further evidence for a dual systems model. Developmental Psychology. 2011;47:739–746. doi: 10.1037/a0023279. [DOI] [PubMed] [Google Scholar]
- Hayatbakhsh MR, Najman JM, McGee TR, Bor W, O’Callaghan MJ. Early pubertal maturation in the prediction of early adult substance use: A prospective study. Addiction. 2009;104:59– 66. doi: 10.1111/j.1360-0443.2008.02382.x. [DOI] [PubMed] [Google Scholar]
- Jesness CF. The Jesness Inventory. Palo Alto, CA: Consulting Psychologists Press; 1983. (rev. ed.) [Google Scholar]
- Kaplan D, Kim J-S, Kim S-Y. Multilevel latent variable modeling: Current research and recent developments. In: Millsap RE, Maydeu-Olivares A, editors. Handbook of quantitative methods in psychology. Thousand Oaks, CA: Sage; 2009. pp. 592–612. [DOI] [Google Scholar]
- King KM, Meehan BT, Trim RS, Chassin L. Substance use and academic outcomes: Synthesizing findings and future directions. Addiction. 2006;101:1688–1689. doi: 10.1111/j.1360-0443.2006.01695.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein AG, Moosbrugger H. Maximum likelihood estimation of latent interaction effects with the LMS method. Psychometrika. 2000;65:457– 474. doi: 10.1007/BF02296338. [DOI] [Google Scholar]
- Lau RS, Cheung GW. Estimating and comparing specific mediation effects in complex latent variable models. Organizational Research Methods. 2012;15:3–16. doi: 10.1177/1094428110391673. [DOI] [Google Scholar]
- LeBlanc M, Fréchette M. Male criminal activity from childhood through youth: Multilevel and developmental perspective. New York, NY: Springer-Verlag; 1989. [Google Scholar]
- Lillehoj CJ, Trudeau L, Spoth R, Madon S. Externalizing behaviors as predictors of substance initiation trajectories among rural adolescents. Journal of Adolescent Health. 2005;37:493–501. doi: 10.1016/j.jadohealth.2004.09.025. [DOI] [PubMed] [Google Scholar]
- Luna B, Padmanabhan A, O’Hearn K. What has fMRI told us about the development of cognitive control through adolescence? Brain and Cognition. 2010;72:101–113. doi: 10.1016/j.bandc.2009.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynne SD, Graber JA, Nichols TR, Brooks-Gunn J, Botvin GJ. Links between pubertal timing, peer influences, and externalizing behaviors among urban students followed through middle school. Journal of Adolescent Health. 2007;40:e7– e13. doi: 10.1016/j.jadohealth.2006.09.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynne-Landsman SD, Graber JA, Nichols TR, Botvin GJ. Is sensation seeking a stable trait or does it change over time? Journal of Youth and Adolescence. 2011;40:48–58. doi: 10.1007/s10964-010-9529-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychological Methods. 2002;7:83–104. doi: 10.1037/1082-989X.7.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research. 2004;39:99–128. doi: 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Magnusson D, Stattin H, Allen VL. Biological maturation and social development: A longitudinal study of some adjustment processes from mid-adolescence to adulthood. Journal of Youth and Adolescence. 1985;14:267–283. doi: 10.1007/BF02089234. [DOI] [PubMed] [Google Scholar]
- Marceau K, Ram N, Houts RM, Grimm KJ, Susman EJ. Individual differences in boys’ and girls’ timing and tempo of puberty: Modeling development with nonlinear growth models. Developmental Psychology. 2011;47:1389–1409. doi: 10.1037/a0023838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls. Archives of Disease in Childhood. 1969;44:291–303. doi: 10.1136/adc.44.235.291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Archives of Disease in Childhood. 1970;45:13–23. doi: 10.1136/adc.45.239.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martin CA, Kelly TH, Rayens MK, Brogli BR, Brenzel A, Smith WJ, Omar HA. Sensation seeking, puberty, and nicotine, alcohol, and marijuana use in adolescence. Journal of the American Academy of Child & Adolescent Psychiatry. 2002;41:1495–1502. doi: 10.1097/00004583-200212000-00022. [DOI] [PubMed] [Google Scholar]
- Masse LC, Tremblay RE. Behavior of boys in kindergarten and the onset of substance use during adolescence. Archives of General Psychiatry. 1997;54:62– 68. doi: 10.1001/archpsyc.1997.01830130068014. [DOI] [PubMed] [Google Scholar]
- McArdle JJ, Nesselroade JR. Growth curve analysis in contemporary psychological research. In: Schinka JA, Velicer WF, editors. Handbook of psychology: Research methods in psychology. Vol. 2. Hobokan, NJ: Wiley; 2002. pp. 447–480. [Google Scholar]
- Mendle J, Harden KP, Brooks-Gunn J, Graber JA. Development’s tortoise and hare: Pubertal timing, pubertal tempo, and depressive symptoms in boys and girls. Developmental Psychology. 2010;46:1341–1353. doi: 10.1037/a0020205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mendle J, Harden KP, Brooks-Gunn J, Graber JA. Peer relationships and depressive symptomatology in boys at puberty. Developmental Psychology. 2012;48:429– 435. doi: 10.1037/a0026425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mustanski BS, Viken RJ, Kaprio J, Rose RJ. Genetic influences on the association between personality risk factors and alcohol use and abuse. Journal of Abnormal Psychology. 2003;112:282–289. doi: 10.1037/0021-843X.112.2.282. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide. Los Angeles, CA: Muthén & Muthén; 1998–2009. [Google Scholar]
- Odgers CL, Caspi A, Nagin DS, Piquero AR, Slutske WS, Milne BJ, Moffitt TE. Is it important to prevent early exposure to drugs and alcohol among adolescents? Psychological Science. 2008;19:1037–1044. doi: 10.1111/j.1467-9280.2008.02196.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Office of National Statistics. Drug use, smoking and drinking among young people in England in 2007. NHS Health and Social Care Information Centre; 2008. [Google Scholar]
- O’Leary-Barrett M, Mackie CJ, Castellanos-Ryan N, Al-Khudhairy N, Conrod PJ. Personality-targeted interventions delay uptake of drinking and decrease risk of alcohol-related problems when delivered by teachers. Journal of the American Academy of Child and Adolescent Psychiatry. 2010;49:954–963. doi: 10.1016/j.jaac.2010.04.011. [DOI] [PubMed] [Google Scholar]
- Oliva EM, Keyes M, Iacono WG, McGue M. Adolescent substance use groups: Antecedent and concurrent personality differences in a longitudinal study. Journal of Personality. 2012;80:769–793. doi: 10.1111/j.1467-6494.2011.00746.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patton GC, McMorris BJ, Toumbourou JW, Hemphill SA, Donath S, Catalano RF. Puberty and the onset of substance use and abuse. Pediatrics. 2004;114:e300– e306. doi: 10.1542/peds.2003-0626-F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paus T. Mapping brain maturation and cognitive development during adolescence. Trends in Cognitive Sciences. 2005;9:60– 68. doi: 10.1016/j.tics.2004.12.008. [DOI] [PubMed] [Google Scholar]
- Petersen AC, Crockett L. Pubertal timing and grade effects on adjustment. Journal of Youth and Adolescence. 1985;14:191–206. doi: 10.1007/BF02090318. [DOI] [PubMed] [Google Scholar]
- Petersen AC, Crockett L, Richards M, Boxer A. A self-report measure of pubertal status: Reliability, validity, and initial norms. Journal of Youth and Adolescence. 1988;17:117–133. doi: 10.1007/BF01537962. [DOI] [PubMed] [Google Scholar]
- Prokopcakova A. Drug experimenting and pubertal maturation in girls. Studia Psychologica. 1998;40:287–290. Retrieved from http://psychologia.sav.sk/sp/ [Google Scholar]
- Rohde P, Lewinsohn PM, Kahler CW, Seeley JR, Brown RA. Natural course of alcohol use disorders from adolescence to young adulthood. Journal of the American Academy of Child & Adolescent Psychiatry. 2001;40:83–90. doi: 10.1097/00004583-200101000-00020. [DOI] [PubMed] [Google Scholar]
- Schmitz KE, Hovell MF, Nichols JF, Irvin VL, Keating K, Simon GM, Jones KL. A validation study of early adolescents’ pubertal self-assessments. The Journal of Early Adolescence. 2004;24:357–384. doi: 10.1177/0272431604268531. [DOI] [Google Scholar]
- Séguin JR, Pihl RO, Harden PW, Tremblay RE, Boulerice B. Cognitive and neuropsychological characteristics of physically aggressive boys. Journal of Abnormal Psychology. 1995;104:614– 624. doi: 10.1037/0021-843X.104.4.614. [DOI] [PubMed] [Google Scholar]
- Shedler J, Block J. Adolescent drug use and psychological health. A longitudinal inquiry. American Psychologist. 1990;45:612– 630. doi: 10.1037/0003-066X.45.5.612. [DOI] [PubMed] [Google Scholar]
- Single E, Rehm J, Robson L, Van Truong M. The relative risks and etiologic fractions of different causes of death and disease attributable to alcohol, tobacco and illicit drug use in Canada. CMAJ. 2000;162:1669–1675. Retrieved from http://www.cmaj.ca/ [PMC free article] [PubMed] [Google Scholar]
- Spear LP. The adolescent brain and age-related behavioral manifestations. Neuroscience and Biobehavioral Reviews. 2000;24:417– 463. doi: 10.1016/S0149-7634(00)00014-2. [DOI] [PubMed] [Google Scholar]
- Steinberg L. Risk taking in adolescence: New perspectives from brain and behavioral science. Current Directions in Psychological Science. 2007;16:55–59. doi: 10.1111/j.1467-8721.2007.00475.x. [DOI] [Google Scholar]
- Steinberg L. A social neuroscience perspective on adolescent risk-taking. Developmental Review. 2008;28:78–106. doi: 10.1016/j.dr.2007.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L. A dual systems model of adolescent risk-taking. Developmental Psychobiology. 2010;52:216–224. doi: 10.1002/dev.20445. [DOI] [PubMed] [Google Scholar]
- Steinberg L, Albert D, Cauffman E, Banich M, Graham S, Woolard J. Age differences in sensation seeking and impulsivity as indexed by behavior and self-report: Evidence for a dual systems model. Developmental Psychology. 2008;44:1764–1778. doi: 10.1037/a0012955. [DOI] [PubMed] [Google Scholar]
- Stormshak EA, Connell AM, Veronneau MH, Myers MW, Dishion TJ, Kavanagh K, Caruthers AS. An ecological approach to promoting early adolescent mental health and social adaptation: Family-centered intervention in public middle schools. Child Development. 2011;82:209–225. doi: 10.1111/j.1467-8624.2010.01551.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Information Centre. Drug use, smoking, and drinking among young people 2007. Leeds, England: The Health and Social Care Information Centre; 2008. [Google Scholar]
- Thissen D, Steinberg L, Kuang D. Quick and easy implementation of the Benjamini-Hochberg procedure for controlling the false positive rate in multiple comparisons. Journal of Educational and Behavioral Statistics. 2002;27:77– 83. doi: 10.3102/10769986027001077. [DOI] [Google Scholar]
- Tremblay RE, Loeber R, Gagnon C, Charlebois P, Larivee S, LeBlanc M. Disruptive boys with stable and unstable high fighting behavior patterns during junior elementary school. Journal of Abnormal Child Psychology. 1991;19:285–300. doi: 10.1007/BF00911232. [DOI] [PubMed] [Google Scholar]
- Tremblay RE, Pihl RO, Vitaro F, Dobkin PL. Predicting early onset of male antisocial behavior from preschool behavior. Archives of General Psychiatry. 1994;51:732–739. doi: 10.1001/archpsyc.1994.03950090064009. [DOI] [PubMed] [Google Scholar]
- Tschann JM, Adler NE, Irwin CE, Jr, Millstein SG, Turner RA, Kegeles SM. Initiation of substance use in early adolescence: The roles of pubertal timing and emotional distress. Health Psychology. 1994;13:326–333. doi: 10.1037/0278-6133.13.4.326. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. The Surgeon General’s call to action to prevent and reduce underage drinking. Rockville, MD: U. S. Department of Health and Human Services; 2007. [Google Scholar]
- van Lier PAC, Huizink A, Crijnen A. Impact of a preventive intervention targeting childhood disruptive behavior problems on tobacco and alcohol initiation from age 10 to 13 years. Drug and Alcohol Dependence. 2009;100:228–233. doi: 10.1016/j.drugalcdep.2008.10.004. [DOI] [PubMed] [Google Scholar]
- Verlaan P, Cantin S, Boivin M. L’Échelle de développement pubertaire: Équivalence en langue française du Pubertal Development Scale. Canadian Journal of Behavioural Science/Revue canadienne des sciences du comportement. 2001;33:143–147. doi: 10.1037/h0087136. [DOI] [Google Scholar]
- Vitaro F, Brendgen M, Tremblay RE. Prevention of school dropout through the reduction of disruptive behaviors and school failure in elementary school. Journal of School Psychology. 1999;37:205–226. doi: 10.1016/S0022-4405(99)00006-0. [DOI] [Google Scholar]
- Westling E, Andrews JA, Hampson SE, Peterson M. Pubertal timing and substance use: The effects of gender, parental monitoring and deviant peers. Journal of Adolescent Health. 2008;42:555–563. doi: 10.1016/j.jadohealth.2007.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whiteside SP, Lynam DR. The five-factor model and impulsivity: Using a structural model of personality to understand impulsivity. Personality and Individual Differences. 2001;30:669– 689. doi: 10.1016/S0191-8869(00)00064-7. [DOI] [Google Scholar]
- Wiesner M, Ittel A. Relations of pubertal timing and depressive symptoms to substance use in early adolescence. The Journal of Early Adolescence. 2002;22:5–23. doi: 10.1177/0272431602022001001. [DOI] [Google Scholar]
- Wilson DM, Killen JD, Hayward C, Robinson TN, Hammer LD, Kraemer HC, Taylor CB. Timing and rate of sexual maturation and the onset of cigarette and alcohol use among teenage girls. Archives of Pediatrics and Adolescent Medicine. 1994;148:789–795. doi: 10.1001/archpedi.1994.02170080019004. [DOI] [PubMed] [Google Scholar]
- Winters KC. Development of an adolescent alcohol and other drug abuse screening scale: Personal Experience Screening Questionnaire. Addictive Behaviors. 1992;17:479– 490. doi: 10.1016/0306-4603(92)90008-J. [DOI] [PubMed] [Google Scholar]
- Zonnevylle-Bender MJS, Matthys W, van de Wiel NMH, Lochman JE. Preventive effects of treatment of disruptive behavior disorder in middle childhood on substance use and delinquent behavior. Journal of the American Academy of Child & Adolescent Psychiatry. 2007;46:33–39. doi: 10.1097/01.chi.0000246051.53297.57. [DOI] [PubMed] [Google Scholar]
- Zuckerman M. Sensation seeking and risky behavior. Washington, DC: American Psychological Association; 2007. [DOI] [Google Scholar]
- Zuckerman M, Kuhlman DM, Thornquist M, Kiers H. Five (or three) robust questionnaire scale factors of personality without culture. Personality and Individual Differences. 1991;12:929–941. doi: 10.1016/0191-8869(91)90182-B. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.