

Abstract
Colonoscopy is a widely used diagnostic and therapeutic modality with a relatively low morbidity. However, given the large volume of procedures performed, awareness of the infrequent complications is essential. Perforation is an established complication of colonoscopy, and can range from 0.2%-3% depending on the series, population and modality of colonoscopy. Acute appendicitis after colonoscopy is an extremely rare event, and a cause-effect relationship between the colonoscopy and the appendicitis is not well documented. In addition, awareness of this condition can aid in prompt diagnosis. Relatively mild symptoms and exclusion of bowel perforation by contrast studies do not exclude appendicitis from the differential diagnosis for post-colonoscopy pain. In addition to the difficult diagnosis inherent to postcolonoscopy appendicitis, treatment strategies have varied greatly. This paper reviews these approaches. We also expand upon prior articles by giving guidance for the role of nonoperative management in these patients. This case and review of the literature will help to create awareness about this complication, and guide optimal treatment of pericolonoscopy appendicitis.
Keywords: Colonoscopy complications, Appendicitis
Core tip: The manuscript highlights a recent interesting case from our institution demonstrating appendicitis after colonoscopy, which was managed surgically. This paper reviews the relevant literature including all related previously published cases, and makes recommendations about defining the syndrome of post-colonoscopy appendicitis and how it should be managed.
INTRODUCTION
Colonoscopy is a widely used diagnostic and therapeutic procedure. Thousands of colonoscopies are performed yearly in the United States alone. Although the risk and complications are low, the high volume of cases makes awareness of these rare complications imperative. Bleeding and perforation are by far the most common complications of colonoscopies; these complications can range from 0.2%-3% depending on the series, population and modality of colonoscopy[1]. Acute appendicitis after colonoscopy is an extremely rare event, and a cause-effect relationship between the colonoscopy and the appendicitis is not well documented. In addition, awareness of this condition can aid in prompt diagnosis. Some degree of mild cramping or gas pain can be normal following colonoscopy, but providers and patients must remain vigilant for unusual symptoms that signal complications of this procedure. Relatively mild symptoms and exclusion of bowel perforation by contrast studies do not exclude appendicitis from the differential diagnosis for post-colonoscopy pain. This case and review of the literature will help to create awareness about this complication, and guide optimal treatment of pericolonoscopy appendicitis.
CASE REPORT
A 67-year-old male was scheduled for colonoscopy for colorectal screening. Colonoscopy and bowel prep were uneventful. Previous to the colonoscopy this patient was asymptomatic. The patient had an unremarkable bowel preparation and denied any abdominal pain, nausea, vomiting or anorexia before the procedure. He underwent colonoscopy without complication. The endoscope was advanced to the cecum and the appendix orifice was visualized. No abnormality was found during the colonoscopy. Twenty-four hours after the endoscopic procedure, the patient developed right lower quadrant pain and nausea. Physical examination demonstrated localized rebound tenderness at McBurney’s point. Computer tomography (CT) scan of the abdomen and pelvis demonstrated a thickened appendix with surrounding fat stranding and an appendicolith (Figure 1). The patient underwent open appendectomy on the day of presentation and convalesced rapidly without further complications. The pathology report was consistent with early acute appendicitis without sign of perforation (Figure 2). The patient recovered from surgery without any other complication.
Figure 1.
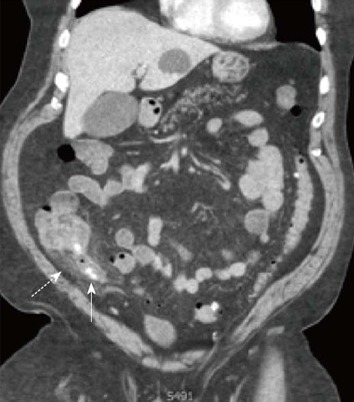
Coronal image of acute appendicitis following colonoscopy. Solid arrow: Appendicolith; Dashed arrow: Appendix.
Figure 2.
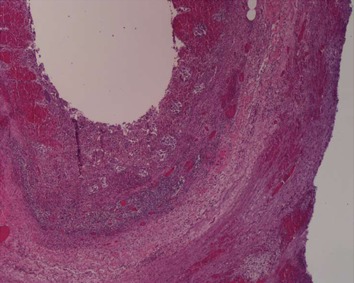
Histology slide of acute appendicitis.
The search strategy employed for identifying articles for this review involved using PubMed. Specifically, to identify the articles of interest we used terms (‘‘Colonoscopy’’ AND ‘‘appendicitis’’ AND ’’complication’’) to produce 14 results, 9 of which were germane to our study. The terms (‘‘postcolonoscopy’’ ‘‘appendicitis’’) were then used, producing 6 total results and only 2 additional references. We used references from these papers to identify additional papers, identifying 21 articles describing cases of postcolonoscopy appendicitis. Additional articles were used for supporting structure to the topic review. PRISMA guidelines were followed.
Inclusion criteria for the review include literature describing cases of appendicitis with a temporal relationship to colonoscopy, and only papers written entirely in English were included. Of the twenty original papers identified using the original search terms above, only 5 were excluded as they involved topics outside of the scope of this review.
Data was extracted independently. Patient characteristics such as age, gender, treatment, and time to presentation were extracted and summarized in Table 1.
Table 1.
Case reports of pericolonoscopy appendicitis
| Author | Age | Gender | Time to diagnosis | Treatment | Perforation? | Postcolonoscopy?1 |
| April et al[18] | 52 | M | 8 h | Appendectomy | Nonperforated | Postcolonoscopy |
| Bachir et al[14] | 28 | M | 2 d | Appendectomy | Nonperforated | Postcolonoscopy |
| Moorman et al[19] | 71 | F | Next morning | NS | Perforated | Postcolonoscopy |
| Moorman et al[19] | 47 | M | 27 h | Laparotomy, appendectomy | Perforated | Postcolonoscopy |
| Moorman et al[19] | 84 | M | 4 h | Laparotomy, appendectomy | Acute appendicitis | Postcolonoscopy |
| Pellish et al[17] | 50 | M | Immediate | Laparoscopic appendectomy | nonperforated | Postcolonoscopy |
| Volchok et al[30] | 60 | M | 16 h | Appendectomy | Nonperforated | Postcolonoscopy |
| Johnston et al[20] | 55 | M | 16 h | Appendectomy | Perforated | Postcolonoscopy |
| Chae et al[21] | 48 | F | 4 d | Appendectomy | No perforation | Postcolonoscopy |
| Izzedine et al[22] | 61 | M | 1 d | Antibiotics->appendectomy | Perforation | Postcolonoscopy |
| Petro et al[7] | 53 | M | Immediate | Open appendectomy | No perforation | Precolonoscopy |
| Rosen et al[23] | 24 | M | 48 h | Laparotomy, appendectomy | NS | Postcolonoscopy |
| Rosen et al[23] | 55 | M | Several hours | Antibiotics only | NS | Postcolonoscopy |
| Srivastava et al[9] | 65 | M | 10 d | Laparotomy, appendectomy | Appendiceal abscess | Postcolonoscopy |
| Takagi et al[24] | 56 | M | 72 h | Laparotomy, appendectomy | Phlegmonous appendix | Postcolonoscopy |
| Lipton et al[25] | 69 | M | 96 h | Laparotomy, Appendectomy | Gangrenous appendix | Postcolonoscopy |
| Hirata et al[26] | 69 | M | 12 h | Laparotomy, appendectomy | Acute appendicitis | Postcolonoscopy |
| Vender et al[4] | 44 | F | Several hours | Laparotomy, appendectomy | NS | Postcolonoscopy |
| Vender et al[4] | 55 | M | 48 h | Antibiotics | NS | Postcolonoscopy |
| Vender et al[4] | 57 | F | Immediate | Laparotomy, appendectomy | Acute appendicitis | Postcolonoscopy |
| Brandt et al[27] | 65 | F | 48 h | Laparotomy, appendectomy | NS | Postcolonoscopy |
| Houghton et al[28] | 35 | M | 8 h | Laparotomy, appendectomy | Acute appendicitis | Postcolonoscopy |
| Musielak et al[29] | 33 | M | 6 h | Laparosopic appendectomy | Acute Appendicitis | Postcolonoscopy |
| Musielak et al[29] | 45 | F | 4 h | Laparosopic appendectomy | Perforated | Postcolonoscopy |
| Penkov et al[10] | 50 | F | 7 d | Laparoscopic appendectomy | appendicitis | Postcolonoscopy |
| Horimatsu et al[31] | 68 | M | 1 d | Antibiotics | NS | Postcolonoscopy with EMR |
| Kothari et al[11] | 27 | F | Immediate | Laparoscopic appendectomy | Purulent erosive appendicitis | Precolonoscopy |
Postcolonoscopy appendicitis defined above in text. M/F: Male/female; NS: Not specified; EMR: Endoscopic mucosal resection.
DISCUSSION
Colonoscopy is a widely used diagnostic and therapeutic procedure. It is relatively safe but is not exempt from risk. Mechanical complications following diagnostic colonoscopy are rare, and bowel perforation in particular has an extremely low incidence (0.3%)[1,2]. Some of these complications can be serious and can lead to surgical intervention. Although exceedingly rare, 27 cases of pericolonoscopy acute appendicitis have been reported.
While it seems possible that the development of appendicitis after colonoscopy could be a coincidence, Occam’s razor might suggest a more causal relationship. The pathophysiology of this condition is not completely understood. Several possible mechanisms have been proposed based on the endoscopic findings and timing of presentation. These include barotrauma from overinsufflation[2], compression of stool into the appendix leading to obstruction and/or inflammation[3], direct trauma by inadvertent intubation of the appendiceal lumen[4] and exacerbation of pre-existing preclinical disease[5]. In addition, a case of acute appendicitis has been recently reported twelve hours after virtual colonoscopy, in which carbon dioxide is used to insufflate the colon prior to high resolution CT scanning[6]. Diagnosis of this complication has ranged from immediate presentation[7,8] to ten days following colonoscopy[9]. When diagnosed during colonoscopy, the trademark findings include erythema and edema around the appendiceal orifice[7]; late diagnosis can contribute to peritonitis and death[9].
Taken together, these reports can be classified as pericolonoscopy acute appendicitis. This is indeed a heterogenous group. Clearly occasional patients have visible appendicitis at the time of colonoscopy[7], and some other patients might also have been beginning to develop appendicitis at the time of colonoscopy without obvious mucosal findings at the orifice and with only subtle or variant symptoms when presenting for their procedure. This also raises the question of when pericolonoscopy appendicitis could be a coincidence as opposed to a complication. Penkov raises this question, and stresses the importance of prompt imaging to facilitate treatment[10].
Given the mechanisms proposed above, we suggest trying to distinguish appendicitis diagnosed at colonoscopy or appendicitis that might have begun before colonoscopy from “true” postcolonoscopy appendicitis. Appendicitis diagnosed during colonoscopy likely stems from a process beginning prior to the colonoscopy with attenuated or atypical signs, as in the case described by Kothari et al[11] with a lower Gastrointestinal (GI) bleed. In contrast, the mechanisms hypothesized to cause postcolonoscopy appendicitis should result in either immediate symptoms or symptoms beginning after a short delay if proceeding via the classical mechanism of intraluminal obstruction and distension. Thus, we propose to define post colonoscopy appendicitis as appendicitis diagnosed by standard criteria with symptoms that begin after the procedure but within 72 h following the colonoscopy, and in the absence of any endoscopic evidence of appendicitis or cecal inflammation at the time of the initial procedure. These criteria should help limit the potential for mere coincidence.
Based on cases reported in the literature, acute appendicitis after colonoscopy appears to be much more common in males. In this series we observe 8 women out of 26 cases. Although men have appendicitis more commonly than women (1.4:1)[12], the apparent predilection of postcolonoscopy appendicitis for men may also reflect increased rates of colonoscopy for men in certain populations such as United States Medicare beneficiaries[13]. The age of patients with this complication cluster from 50-70 in line with recommendations for screening colonoscopy, with notable younger exceptions among patients with gastrointestinal bleeding or ulcerative colitis[11,14]. It is possible that more than one mechanism can be implicated, especially when a patient may have an anatomical or immune predisposition to develop the inflammatory process, triggered by the preparation and or the procedure itself. Since our patient had no underlying disease and exhibited a typical presentation of appendicitis with symptoms beginning one day after colonoscopy, we believe that his appendicitis was most likely triggered by pneumatic pressure impacting the fecalith into the the appendiceal lumen, consistent with the demonstration of multiple appendicoliths on his preoperative imaging and confirmed on his pathology report. The pathophysiology of postcolonoscopy appendicitis may offer an interesting model to study appendicitis at large, as it provides a more precise onset for the time of intraluminal obstruction than the spontaneous inception of obstruction in typical appendicitis.
Table 1 summarizes demographic data, timing of presentation and treatment in previous reports of acute appendicitis following colonoscopy[9-31]. Appendectomy was the preferred treatment with few exceptions. Delay in diagnosis might preclude early appendectomy and can increase complications. Srivastava et al[9] report on a patient diagnosed with appendiceal abscess at 10 d following colonoscopy. A contrast study excluded leak at the polypectomy site on day 5 following colonoscopy in an afebrile patient with a normal white count. This delay in diagnosis and treatment ultimately resulted in multiorgan system failure and death. Although rare, it is likely that failure to consider appendicitis is the largest barrier to prompt diagnosis.
The majority of these cases were addressed by open appendectomy, which is an acceptable but notable alternative to the laparoscopic approach. It is possible that providers chose laparotomy due to concerns about colonoscopic bowel perforation. Recognizing appendicitis as a potential complication of colonoscopy might have permitted an initial laparoscopic approach.
Recent randomized trial evidence suggests that antibiotics alone can be used to treat uncomplicated appendicitis[15]. Uncomplicated diverticulitis should also be treated without surgery[16]. In addition, there is also the criteria for conservative management of selected colonoscopic perforations[1]. Taken together, these lines of evidence raise the question of whether there may be a role for conservative management of post-colonoscopy appendicitis in select patients in whom the bowel preparation was adequate and in whom there is no evidence of perforation, no history of immunocompromise, and adequate mental status for observation. Patients with peritonitis should be excluded from nonoperative therapy as the value of this conservative approach is tested in this population. A nonoperative approach would be especially attractive in managing a complication of a screening procedure.
With this case report, we intend to emphasize and create awareness that acute appendicitis is a rare but real complication of colonoscopy. We stress the importance of recognizing this condition promptly to provide early treatment and avoid further complications. These cases should continue to be documented especially to define the best overall approach in managing this complication.
Footnotes
P- Reviewers Brugge WR, Eslick GD, Radojcic BS S- Editor Zhai HH L- Editor A E- Editor Lu YJ
References
- 1.Kavic SM, Basson MD. Complications of endoscopy. Am J Surg. 2001;181:319–332. doi: 10.1016/s0002-9610(01)00589-x. [DOI] [PubMed] [Google Scholar]
- 2.Basson MD, Etter L, Panzini LA. Rates of colonoscopic perforation in current practice. Gastroenterology. 1998;114:1115. doi: 10.1016/s0016-5085(98)70348-8. [DOI] [PubMed] [Google Scholar]
- 3.Gatto NM, Frucht H, Sundararajan V, Jacobson JS, Grann VR, Neugut AI. Risk of perforation after colonoscopy and sigmoidoscopy: a population-based study. J Natl Cancer Inst. 2003;95:230–236. doi: 10.1093/jnci/95.3.230. [DOI] [PubMed] [Google Scholar]
- 4.Vender R, Larson J, Garcia J, Topazian M, Ephraim P. Appendicitis as a complication of colonoscopy. Gastrointest Endosc. 1995;41:514–516. doi: 10.1016/s0016-5107(05)80015-x. [DOI] [PubMed] [Google Scholar]
- 5.Doohen RR, Aanning HL. Appendiceal colic: A rare complication of colonoscopy. S D J Med. 2002;55:526–527. [PubMed] [Google Scholar]
- 6.Bildzukewicz NA, Weinstein MS. Appendicitis following virtual colonoscopy: a case report. J Gastrointest Surg. 2012;16:2291–2293. doi: 10.1007/s11605-012-1994-3. [DOI] [PubMed] [Google Scholar]
- 7.Petro M, Minocha A. Asymptomatic early acute appendicitis initiated and diagnosed during colonoscopy: a case report. World J Gastroenterol. 2005;11:5398–5400. doi: 10.3748/wjg.v11.i34.5398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Benatta MA. Incidental diagnostic and treatment of a suppurative appendicitis at colonoscopy. Case Rep Med. 2012;2012:523708. doi: 10.1155/2012/523708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Srivastava V, Pink J, Swarnkar K, Feroz A, Stephenson BM. Colonoscopically induced appendicitis. Colorectal Dis. 2004;6:124–125. doi: 10.1111/j.1463-1318.2004.00579.x. [DOI] [PubMed] [Google Scholar]
- 10.Penkov P. Acute appendicitis following colonoscopy: causality or coincidence. ANZ J Surg. 2011;81:491–492. doi: 10.1111/j.1445-2197.2011.05767.x. [DOI] [PubMed] [Google Scholar]
- 11.Kothari T, Jormark S, Machnicki S, Robbins D. Acute purulent erosive appendicitis diagnosed during colonoscopy. Dig Endosc. 2012;24:292. doi: 10.1111/j.1443-1661.2011.01226.x. [DOI] [PubMed] [Google Scholar]
- 12.Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132:910–925. doi: 10.1093/oxfordjournals.aje.a115734. [DOI] [PubMed] [Google Scholar]
- 13.Gancayco J, Soulos PR, Khiani V, Cramer LD, Ross JS, Genao I, Tinetti M, Gross CP. Age-based and sex-based disparities in screening colonoscopy use among medicare beneficiaries. J Clin Gastroenterol. 2013;47:630–636. doi: 10.1097/MCG.0b013e31828345c8. [DOI] [PubMed] [Google Scholar]
- 14.Bachir NM, Feagins LA. Postcolonoscopy appendicitis in a patient with active ulcerative colitis. World J Gastrointest Endosc. 2010;2:232–234. doi: 10.4253/wjge.v2.i6.232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mason RJ, Moazzez A, Sohn H, Katkhouda N. Meta-analysis of randomized trials comparing antibiotic therapy with appendectomy for acute uncomplicated (no abscess or phlegmon) appendicitis. Surg Infect (Larchmt) 2012;13:74–84. doi: 10.1089/sur.2011.058. [DOI] [PubMed] [Google Scholar]
- 16.Shabanzadeh DM, Wille-Jørgensen P. Antibiotics for uncomplicated diverticulitis. Cochrane Database Syst Rev. 2012;11:CD009092. doi: 10.1002/14651858.CD009092.pub2. [DOI] [PubMed] [Google Scholar]
- 17.Pellish R, Ryder B, Habr F. An unusual complication: postcolonoscopy appendicitis. Endoscopy. 2007;39 Suppl 1:E138. doi: 10.1055/s-2007-966288. [DOI] [PubMed] [Google Scholar]
- 18.April MD, Simmons JR, Nielson AS. An unusual cause of postcolonoscopy abdominal pain. Am J Emerg Med. 2013;31:273. e1–273. e4. doi: 10.1016/j.ajem.2012.05.011. [DOI] [PubMed] [Google Scholar]
- 19.Moorman ML, Miller JP, Khanduja KS, Price PD. Postcolonoscopy appendicitis. Am Surg. 2010;76:892–895. [PubMed] [Google Scholar]
- 20.Johnston P, Maa J. Perforated appendicitis after colonoscopy. JSLS. 2008;12:335–337. [PMC free article] [PubMed] [Google Scholar]
- 21.Chae HS, Jeon SY, Nam WS, Kim HK, Kim JS, Kim JS, An CH. Acute appendicitis caused by colonoscopy. Korean J Intern Med. 2007;22:308–311. doi: 10.3904/kjim.2007.22.4.308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Izzedine H, Thauvin H, Maisel A, Bourry E, Deschamps A. Post-colonoscopy appendicitis: case report and review of the literature. Am J Gastroenterol. 2005;100:2815–2817. doi: 10.1111/j.1572-0241.2005.00309_5.x. [DOI] [PubMed] [Google Scholar]
- 23.Rosen MJ, Sands BE. Acute appendicitis following colonoscopy. J Clin Gastroenterol. 2005;39:78. [PubMed] [Google Scholar]
- 24.Takagi Y, Abe T. Appendicitis following endoscopic polypectomy. Endoscopy. 2000;32:S49. [PubMed] [Google Scholar]
- 25.Lipton S, Estrin J. Postcolonoscopy appendicitis: a case report. J Clin Gastroenterol. 1999;28:255–256. doi: 10.1097/00004836-199904000-00015. [DOI] [PubMed] [Google Scholar]
- 26.Hirata K, Noguchi J, Yoshikawa I, Tabaru A, Nagata N, Murata I, Itoh H. Acute appendicitis immediately after colonoscopy. Am J Gastroenterol. 1996;91:2239–2240. [PubMed] [Google Scholar]
- 27.Brandt E, Naess A. Acute appendicitis following endoscopic polypectomy. Endoscopy. 1989;21:44. doi: 10.1055/s-2007-1012894. [DOI] [PubMed] [Google Scholar]
- 28.Houghton A, Aston N. Appendicitis complicating colonoscopy. Gastrointest Endosc. 1988;34:489. doi: 10.1016/s0016-5107(88)71451-0. [DOI] [PubMed] [Google Scholar]
- 29.Musielak M, Patel H, Fegelman E. Postcolonoscopy appendicitis: laparoscopy a viable option. Am Surg. 2012;78:1300–1303. [PubMed] [Google Scholar]
- 30.Volchok J, Cohn M. Rare complications following colonoscopy: case reports of splenic rupture and appendicitis. JSLS. 2006;10:114–116. [PMC free article] [PubMed] [Google Scholar]
- 31.Horimatsu T, Fu KI, Sano Y, Yano T, Saito Y, Matsuda T, Fujimori T, Yoshida S. Acute appendicitis as a rare complication after endoscopic mucosal resection. Dig Dis Sci. 2007;52:1741–1744. doi: 10.1007/s10620-006-9467-8. [DOI] [PubMed] [Google Scholar]