

Linezolid, an oxazolidinone antibiotic approved for the treatment of respiratory tract and skin infection caused by Gram-positive bacteria, is known to have mitochondrial toxicity.1 Mitochondrial toxicity is explained by linezolid’s specific binding to mitochondrial ribosomes, leading to inhibition of mitochondrial protein synthesis.2
Ring sideroblasts (RS) are erythroid precursors with mitochondrial iron accumulation appearing as perinuclear granules on bone marrow (BM) smears after staining with Prussian blue. Ring sideroblasts are mainly observed in myelodysplastic syndromes (MDS) particularly refractory anemia with ring sideroblasts (RARS) and less often in several types of inherited sideroblastic anemia.3 RARS is defined by both the presence of dyserythropoiesis and 15% or more RS among the erythroid precursors.4 Molecular mechanisms leading to RS in RARS are not well understood.5 Recently, mutations of SF3B1, a gene implicated in the spliceosome machinery, were found in up to 60–75% of RARS.6 Altered function of SF3B1 protein seems responsible for the phenotype observed in RARS.7
Several drugs induce reversible sideroblastic anemia, including isoniazid and chloramphenicol. Linezolid is known to have hematologic toxicity, including anemia and thrombocytopenia. Pre-clinical studies with linezolid in dogs have shown the presence of ring sideroblasts on bone marrow (BM) smears.8 Clinical cases of linezolid-induced and reversible sideroblastic anemia have been reported.9–13
To establish the incidence of induced ring sideroblasts and sideroblastic anemia on linezolid therapy, we retrospectively analyzed BM smears of patients who were treated by linezolid in our center over a period of one year. Approval of this study was obtained from the Institutionnal Review Board of CHRU of Lille (N. CSTMT101).
All medical prescriptions of linezolid made in the University Hospital of Lille, France, in 2011 were reviewed. Overall, 921 patients received the drug for at least one day. Seventy-three patients had at least one BM smear in the three months following treatment, resulting in a total of 94 BM smears as some patients were treated several times). Most patients (55 of 73) had a history of hematologic malignancy; this fact could be explained by the large use of BM aspirates in the diagnostic procedure and follow up of these diseases.
After excluding 2 patients with no smear available for blue Prussian staining, 92 BM smears from 71 patients were stained. Counting of ring sideroblasts (RS) was performed by 2 separate morphologists. In case of discrepancy, a third count was made by another morphologist. BM smears with less than 5% erythroblasts were excluded (13 BM smears corresponding to 5 patients). Thus, 79 BM smears (66 patients) were finally analyzed.
Among the 66 patients, 48 had a history of hematologic malignancy (acute myeloid leukemia (AML) in 39 patients). No patient had a history of MDS. BM examination was realized systematically for underlying hematologic malignancies and for unexplained cytopenia(s). No patient was treated with drugs known to induce sideroblastic anemia (isoniazid, chloramphenicol).
Ten BM smears (10 of 66 patients, i.e. 15.1% of the final cohort) presented 15% or more RS of erythroid precursors (Table 1 and Figure 1). All patients were treated with linezolid 600 mg twice a day. Bone marrow was examined to explore cytopenia(s) in 8 patients with suspected linezolid toxicity. Median age was 63 years. Two patients (2 of 10) had a previous history of AML and one patient had history of post-transplant lymphoproliferative disease (1 of 10). No hematologic malignancy was known in the other patients. At the time of BM aspiration, 9 of 10 patients presented sideroblastic anemia (median hemoglobin 9.35 g/dL) with a median mean corpuscular volume (MCV) of 90.3 fL, 7 of 10 were thrombocytopenic (median platelet count 56 × 109/L) and none neutropenic (median neutrophil count 5.05 × 109/L). Dyserythropoiesis was observed in 6 of 10 patients and considered as “MDS-like” in 2 patients. Median percentage of RS was 52% (range 30–78.5%) of the number of erythroblasts. Median time of linezolid exposure was 13.5 days (range 8–31), median delay of BM aspiration after linezolid introduction was 13.5 days (range 8–29) and median delay between last intake and BM evaluation was one day (range 0–15).
Table 1.
Characteristics of patients with induced sideroblastosis on linezolid therapy.
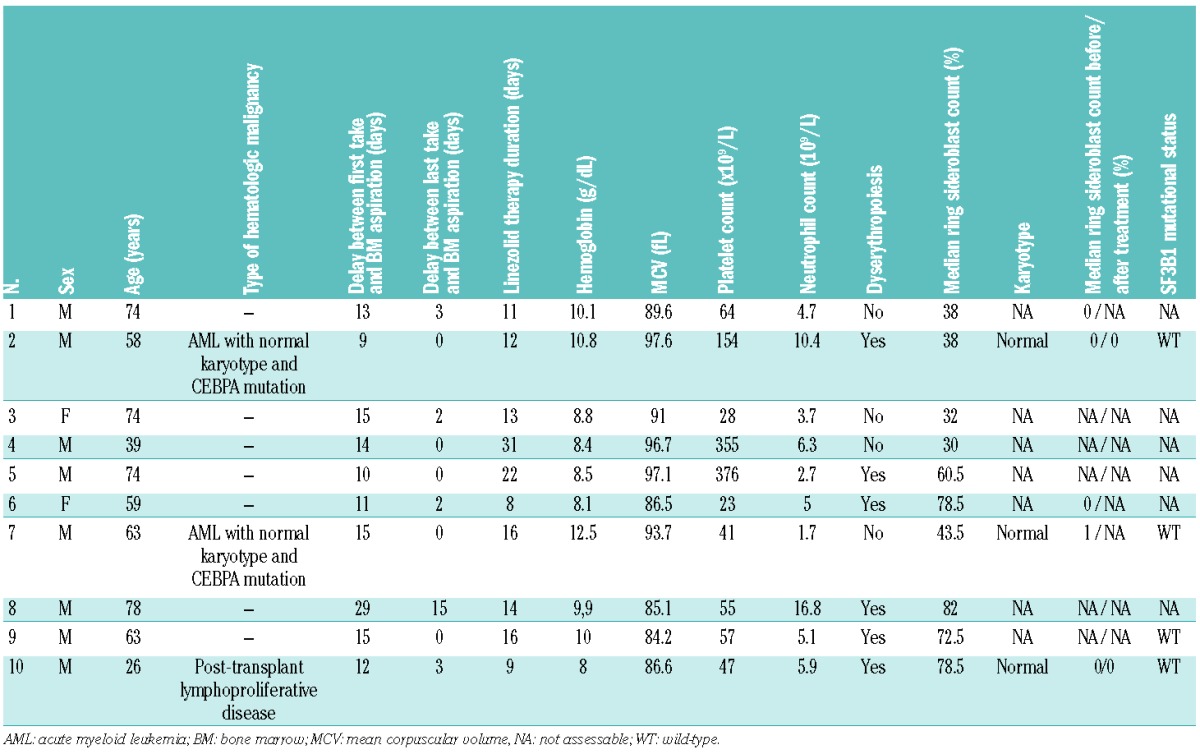
Figure 1.
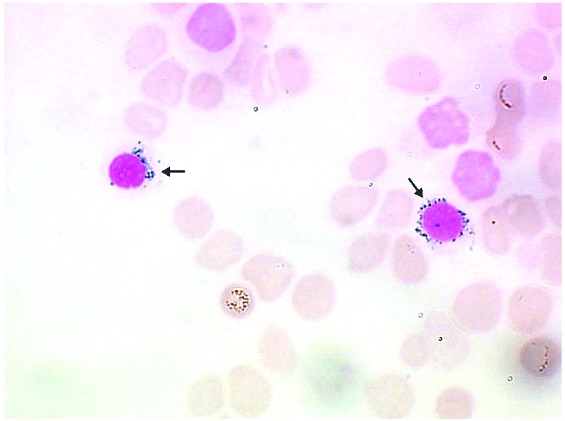
Ring sideroblasts observed on linezolid treatment (arrows); bone marrow aspirate. Prussian blue staining ×1000.
In patients with RS over 15% of erythroblasts, BM smears before and/or after therapy were analyzed to determine the reversibility of RS. BM smears were available for Prussian blue staining in 5 of 10 patients before therapy and in 2 of 10 after therapy. Morphological evaluation did not reveal any RS (including patients with previous history of AML). Blood count was available in 5 patients far from therapy (median time between bone marrow aspiration on linezolid therapy and best blood count evaluation 9.9 months). All but one had normalization of hemoglobin (median hemoglobin 12 g/dL) while platelet count was normal in all 5 patients (median platelet count 284×109/L). BM karyotype and screening of SF3B1 exons 13 to 16 mutations by PCR and Sanger sequencing were also performed to exclude MDS diagnosis. BM karyotype was normal when available (3 of 10). BM samples were available for molecular analysis in 4 patients and reveal no SF3B1 mutations.
Linezolid induces anemia and thrombocytopenia mainly after two weeks of exposure. To our knowledge, there are only a few cases reported of sideroblastic anemia induced by linezolid. Our retrospective study is the first to assess the incidence of RS on BM smears in a large cohort of patients treated with linezolid. RS 15% or over of erythroblasts was seen in approximately 15% of patients who required BM evaluation after a median exposure to treatment of 13.5 days. Nine patients presented sideroblastic anemia.
The acquired and reversible features of induced RS on linezolid therapy were suggested by evaluation of sequential BM smears, normalization of blood count far from therapy, karyotypes and absence of SF3B1 mutations. Unfortunately, those data were not always available. No specific feature was associated with induced RS in the 10 patients except a very high percentage of RS (median percentage 52%).
Some drugs, such as isoniazid, penicillamine, chloramphenicol and busulfan, are known to induce reversible sideroblastic anemia by different mechanisms.14,15 Linezolid’s toxicity seems similar to that of chloramphenicol (inhibition of mitochondrial translation, induction of reversible sideroblastic anemia after a median exposure of 2 weeks).
Considering these results and the large use of linezolid, hematologists should avoid overdiagnosing MDS as RARS in case of recent or concomitant linezolid treatment.
Acknowledgments
We thank the staff of the hematology laboratory of the University Hospital of Lille for their participation in this work. We thank Eileen Boyle for her help in revising the English translation.
Footnotes
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Soriano A, Miró O, Mensa J. Mitochondrial toxicity associated with linezolid. N Engl J Med. 2005;353(21):2305–6 [DOI] [PubMed] [Google Scholar]
- 2.Leach KL, Swaney SM, Colca JR, McDonald WG, Blinn JR, Thomasco LM, et al. The site of action of oxazolidinone antibiotics in living bacteria and in human mitochondria. Mol Cell. 2007;26(3):393–402 [DOI] [PubMed] [Google Scholar]
- 3.Cazzola M, Invernizzi R. Ring sideroblasts and sideroblastic anemias. Haematologica. 2011;96(6):789–92 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mufti GJ, Bennett JM, Goasguen J, Bain BJ, Baumann I, Brunning R, et al. Diagnosis and classification of myelodysplastic syndrome: international working group on morphology of myelodysplastic syndrome (iwgm-mds) consensus proposals for the definition and enumeration of myeloblasts and ring sideroblasts. Haematologica. 2008;93(11):1712–7 [DOI] [PubMed] [Google Scholar]
- 5.Cuijpers MLH, Raymakers RAP, Mackenzie MA, de Witte TJM, Swinkels DW. Recent advances in the understanding of iron overload in sideroblastic myelodysplastic syndrome. Br J Haematol. 2010;149(3):322–33 [DOI] [PubMed] [Google Scholar]
- 6.Papaemmanuil E, Cazzola M, Boultwood J, Malcovati L, Vyas P, Bowen D, et al. Somatic sf3b1 mutation in myelodysplasia with ring sideroblasts. N Engl J Med. 2011;365(15):1384–95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Visconte V, Rogers HJ, Singh J, Barnard J, Bupathi M, Traina F, et al. Sf3b1 haploinsufficiency leads to formation of ring sideroblasts in myelodysplastic syndromes. Blood. 2012;120(16):3173–86 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lund JE, Brown PK. Hypersegmented megakaryocytes and megakaryocytes with multiple separate nuclei in dogs treated with pnu-100592, an oxazolidinone antibiotic. Toxicol Pathol. 1997;25(4):339–43 [DOI] [PubMed] [Google Scholar]
- 9.Montpetit MC, Shammo JL, Loew J, Dunlap S, Pamboukian SV, Heroux A. Sideroblastic anemia due to linezolid in a patient with a left ventricular assist device. J Heart Lung Transplant. 2004;23 (9):1119–22 [DOI] [PubMed] [Google Scholar]
- 10.Kakimoto T, Nakazato T, Miura R, Kurai H, Yamashita D, Sagara Y, et al. [Sideroblastic anemia after prolonged linezolid therapy]. Rinsho Ketsueki. 2008;49(11):1566–8 [PubMed] [Google Scholar]
- 11.Dawson MA, Davis A, Elliott P, Cole-Sinclair M. Linezolid-induced dyserythropoiesis: chloramphenicol toxicity revisited. Intern Med J. 2005;35(10):626–8 [DOI] [PubMed] [Google Scholar]
- 12.Abena PA, Mathieux VG, Scheiff JM, Michaux LM, Vandercam BC. Linezolid and reversible myelosuppression. JAMA. 2001;286(16): 1973; author reply 1974. [PubMed] [Google Scholar]
- 13.Saini N, Jacobson JO, Jha S, Saini V, Weinger R. The perils of not digging deep enough--uncovering a rare cause of acquired anemia. Am J Hematol. 2012;87(4):413–6 [DOI] [PubMed] [Google Scholar]
- 14.Ammus S, Yunis AA. Drug-induced red cell dyscrasias. Blood Rev. 1989;3(2):71–82 [DOI] [PubMed] [Google Scholar]
- 15.Fernandez LA, Zayed E. Busulfan-induced sideroblastic anemia. Am J Hematol. 1988;28(3):199–200 [DOI] [PubMed] [Google Scholar]