

Abstract
Purpose
To detect major acute gastroenteritis virus (rotavirus, norovirus, astrovirus, and enteric adenovirus) and non-enteric type of adenovirus (AdV) in the stools of intussusception patients and to investigate the clinical role of detected viruses.
Methods
From March 2012 to February 2013, major acute gastroenteritis virus and non-enteric type of AdV were isolated from stool samples that collected from 44 patients treated for intussusception in Chungnam National University Hospital. Patients were divided according to age and isolated virus.
Results
Virus was detected in 28 (63%) stool specimens. The virus detection rate was significantly lower in patients aged under 12 months (p = 0.04). Twenty-two patients (78.6%) had non-enteric adenovirus, 4 (14.3%) had norovirus, 1 (3.6%) had sapovirus, and 1 (3.6%) had astrovirus. AdV subgroup C (AdV 1, 2, 5, and 6) comprised the majority with 20 cases (90.9%). A monthly increment-and-decrement pattern of intussusception was similar to that of viral detection in the stool samples. Enema reductions were successful in 39 patients and surgical manual reductions were performed in 5 patients. Virus was detected in 24 patients (61.5%) of enema reduction group and 4 patients (80.0%) of surgical manual reduction group. All of the detected viruses were non-enteric adenovirus subgroup C (AdV 1, 5, and 6) in surgical reduction patients.
Conclusions
The virus detection rate was high in the stools of intussusception patients. The pattern of seasonal intussusception occurrence rate was parallel with seasonal these viral detection rate in the stool samples. These findings suggest that viral infection plays an important role in the development of intussusception and further research is warranted.
Keywords: Intussusception, Non-enteric type of adenovirus, Norovirus
INTRODUCTION
Intussusception is the most common cause of intestinal obstruction in infants, with 80% of cases occurring before 2 years [1]. Although the pathogenic mechanism of intussusception without leading points has not yet been clarified, its major cause is suggested to be swelling and lymph node hyperplasia of Peyer's patch in the ileum secondary to infection [2].
Swelling of the lymphoid tissue and lymph node hyperplasia can occur from not only local reactions to infection but also reactions to food antigenic protein irritation, vaccination, systemic infection, etc. In 1998, infants who received the first rotavirus gastroenteritis vaccination, rhesus-human reassortant 4 vaccine (RRV-TV; Rotashield, Wyeth-Lederle Vaccines; Wteth Laboratories Inc., Marietta, PA, USA), developed intussusception within 2 weeks of vaccination with a 20-30-fold higher incidence, leading to the prohibition of such vaccination [3,4]. According to Bines et al. [5], the incidence of intussusception is higher in Vietnam and China than in Australia and the United States, and is related to adenovirus (Adv) infection. Recently, Okimoto et al. [6] reported that non-enteric adenovirus is a risk factor for the development of intussusception, and poliovirus, enterovirus, parechovirus, norovirus, and rotavirus are found in some stool specimens of affected patients. These results suggest that viral infection plays a vital role in the etiology of intussusception. We performed this study to detect major acute gastroenteritis virus and non-enteric type of AdV in the stool of intussusception patients and to evaluate the clinical role of detected viruses.
The aim of our study was to investigate the detection rate of major primary gastroenteritis viruses (rotavirus, norovirus, sapovirus, enteric adenovirus type 40 and 41, and astrovirus) and non-enteric adenoviruses and the clinical role and features associated with these viruses isolated from stool specimens of infants with intussusception.
MATERIALS AND METHODS
Patients
Forty four patients treated for intussusception at the Department of Pediatrics and Adolescent of Chungnam National University Hospital from March 2012 to February 2013 was enrolled. Diagnosis of intussusception was based on medical history, physical examination, and abdominal X-ray, ultrasonography, and enema reduction findings. Our study protocol was authorized by the institutional review board of Chungnam National University Hospital (2012-06-017-002), and the guardians provided informed consent for stool collection and identification of viruses in the stool specimens. Patients with mechanical causes were excluded from the study. According to the results of virus detection, patients were divided into the non-enteric adenovirus group and major acute gastroenteritis virus group, and the cases in which no viruses were detected were categorized as the no virus isolate group. The patient also divided into subgroup by the age. The clinical features and seasonal incidence were analyzed.
Assessment of viral pathogens
1. Blood testing, stool specimen collection, and viral nucleic acid extraction
Complete blood cell count, serum electrolytes, blood sugar, liver function, and C-reactive protein levels were measured from blood samples. All blood samples were collected before enema reduction. Two stool specimens were collected during the hospitalization period from each patient: 1 was immediately analyzed for 4 primary gastroenteritis viruses and the other was kept at -60℃ for subsequent non-enteric adenovirus isolation. During the weekend or holidays, stool specimens were refrigerated at -4℃ as soon as stool collection. Viral nucleic acid extraction from the stool specimens was performed using the following protocol: fecal samples were suspended in phosphate-buffered saline (10% w/v) and centrifuged at 13,000 rpm for 20 minutes. Viral nucleic acids were isolated from the supernatant using commercially available viral deoxyribonucleic acid (DNA) and ribonucleic acid (RNA) extraction kits.
2. Detection of norovirus, astrovirus, sapovirus, enteric adenovirus, and rotavirus
Real-time reverse transcriptase polymerase chain reaction (RT-PCR) was performed for detection of rotavirus, astrovirus, sapovirus, and norovirus from the extracted RNA. RT-PCR reaction was run at 45℃ for 15 min, 95℃ for 10 min, and then followed by 45 cycles 95℃ for 30 sec and 55℃ for 30 sec. Adenovirus 40 and 41 were extracted using a real-time PCR kit.
3. Detection of non-enteric adenovirus
Partial hexon gene was amplified from the extracted DNA by PCR using primes Ad1: 5'-TTCCCCATGGCICAYAACAC-3', and Ad2: 5'-CCCTGGTAKCCRATRTTGTA-3', and then amplified DNA products were analyzed by gel electrophoresis to confirm positive specimens and the adenovirus subtypes were analyzed.
Statistical analysis
The IBM SPSS Statistics 20.0 (IBM Co., Armonk, NY, USA) was used for statistical analysis. Virus detection frequency according to age, clinical features by age and by group, time from the onset of symptoms to enema reduction, and the response to enema reduction treatment were tested using Fisher's exact test. Blood test results were analyzed using the Kruskal-Wallis test. Values of p<0.05 were considered statistically significant.
RESULTS
Clinical characteristics of the patients
The average patient age was 28±20 months (range, 4-82 months), with 12 (27.3%) aged under 12 months, 12 (27.3%) between 12 and 24 months, and 20 (45.4%) over 24 months. The male to female ratio was 2 : 1 (30 boys and 14 girls). The main symptoms were periodic abdominal pain or irritability (95.5%), vomiting (25.5%), bloody stools (25.0%). Nine patients (25.5%) had upper airway infection symptoms (Table 1). Vomiting and bloody stools were significantly higher in patients under 2 years of age (66.7% and 41.6%, respectively) than those aged over 2 years (p=0.002, 0.006, respectively) (Table 1). Eight patients (18.2%) had past intussusception history, and 3 patients (6.8%) developed reoccurrence within 24 hours of enema reduction. Of the 5 patients who underwent surgical manual reduction, enema reduction was performed on 3 patients within 24 hours, 1 patient within 48 hours, and 1 patient within 72 hours after initial onset of symptoms.
Table 1.
Clinical Manifestations of Patients with Intussusception by Age and Viral Isolates
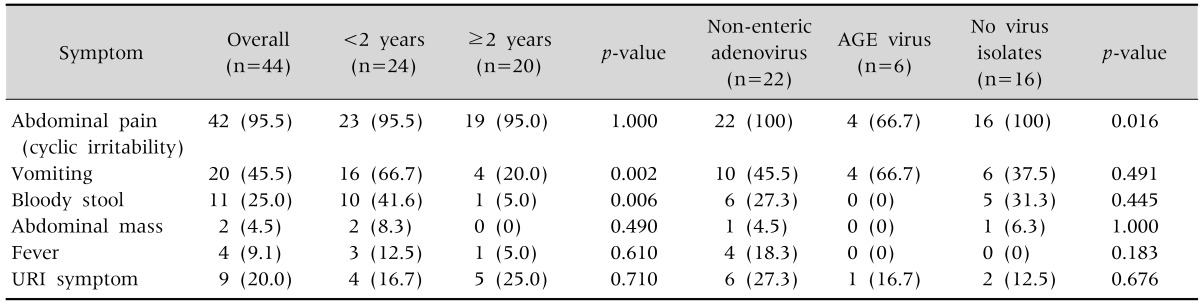
Values are presented as number (%). AGE virus: acute gastroenteritis virus including noro, spo, astro, enteric adeno, and rota virus, URI: upper respiratory infection.
Virus detection rate and clinical features by age
Virus was detected in 28 stool specimens (63.6%), obtained from 4 patients (9.1%) aged under 12 months, 10 (22.7%) between 12 and 24 months, and 14 (31.8%) above 24 months (Fig. 1). The detection rate according to age group was 4/12 (33.3%) in patients aged under 12 months, 10/12 (83.3%) in patients between 12 and 24 months, and 14/20 (70.0%) in patients above 24 months. The virus detection rate was significantly lower in patients aged under 12 months (p=0.04, Fig. 1). Regarding the clinical features of each group based on the type of virus detected in the stool specimen, abdominal pain occurred in the non-enteric adenovirus group (22/22 patients, 100%), major acute gastroenteritis virus group (4/6 patients, 66.7%), and no virus isolate group (16/16 patients, 100%). Abdominal pain was significantly common in non-enteric adenovirus and no virus isolate groups (p=0.016, Table 1). However, there were not any significant intergroup differences in vomiting, bloody stools, abdominal mass, fever, upper respiratory system symptoms, and blood test results (Tables 1 and 2).
Fig. 1.

The number of patients with intussusception and viral isolates by age. The number of cases show non-enteric adenovirus isolates (n=22), AGE virus isolates (n=6), and no virus isolates (n=16). AGE virus: acute gastroenteritis virus including noro, spo, astro, enteric adeno, and rota virus. p=0.041.
Table 2.
Laboratory Findings according to the Isolation of Stool Viruses (n=44)

Values are presented as mean±standard deviation. AGE virus: acute gastroenteritis virus including noro, spo, astro, enteric adeno, and rotavirus, WBC: white blood cell, ALP: alkaline phosphatase, CRP: C-reactive protein.
Infectious pathogens
Of 44 total patients, non-enteric adenovirus was detected in 22 patients (50%) and primary gastroenteritis virus was detected in 6 patients (13.6%), including norovirus (n=4, 9.1%), co-infection of enteric adenovirus and sapovirus (n=1, 2.3%), and astrovirus (n=1, 2.3%). Overall, non-enteric adenovirus had the highest detection rate, norovirus was the next, and rotavirus was not detected (Fig. 2). For non-enteric adenovirus, subgroup C was detected in 20 of 22 patients (90.9%): 7 patients (31.8%) with adenovirus (AdV)-1 (C1), 3 patients (13.6%) with AdV-2 (C2), 8 patients (36.4%) with AdV-5 (C5), 1 patient (4.5%) with AdV-6 (C6), 1 patient (4.5%) with AdV-31 (A31), and 1 patient (4.5%) with AdV-3 (B3), with AdV-1 and 2 comprising the majority (Table 3). For the cases of gastroenteritis virus, all noroviruses were GII, and 3 of 4 patients (75%) were older than 2 years of age. One patient with enteric adenovirus and sapovirus co-infection and other one with astrovirus were younger than 2 years of age (Table 3). Non-enteric adenovirus was detected in all age groups, while gastroenteritis virus was not detected in patients aged under 12 months (Fig. 1 and 2).
Fig. 2.

Viruses detected from stool specimens of patients with intussusception.
Table 3.
Viral Isolates in Patients with Intussusception
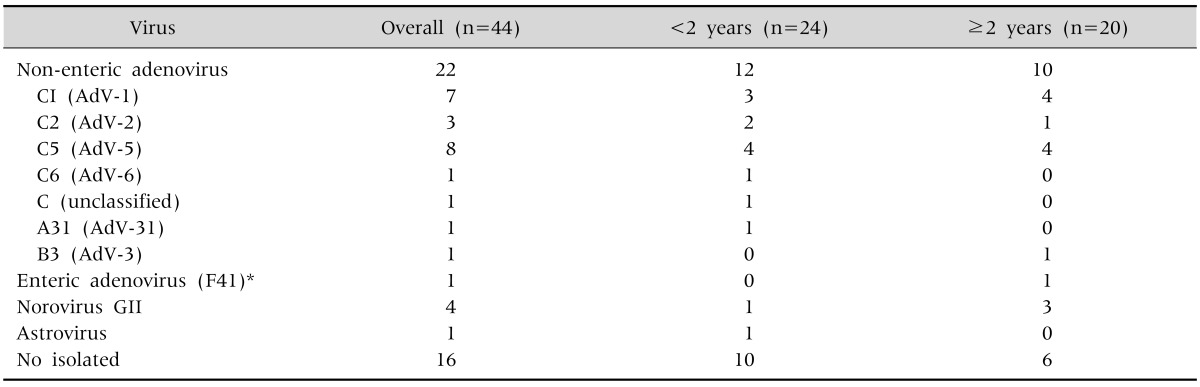
Values are presented as number (%).
*Two pathogens (adenovirus F41 and sapovirus) were isolated.
Monthly virus distribution
Intussusception cases occurred through winter to early summer, and there was almost no incidence during the fall. The patterns of monthly virus detection rate and intussusception occurrence rate were similar, i.e., the number of intussusception patients increased in proportion with the viral detection rates (Fig. 3). In addition, similar patterns were observed between monthly non-enteric adenovirus detection in stools and monthly adenovirus detection variation in local respiratory specimens [7].
Fig. 3.

Monthly distribution of viruses isolated and incidence of intussusception. AGE virus isolated included 1 astrovirus and 4 norovirus. Astrovirus was isolated in August. Calicivirus (norovirus, sapovirus) and enteric adenovirus were isolated from December to February. AGE virus: acute gastroenteritis virus including noro, spo, astro, enteric adeno, and rota virus.
Detected virus and reduction type
Enema reduction and surgical manual reduction were performed on 39 patients (88.6%) and 5 patients (11.4%), respectively. Viruses were detected in 24 patients (61.5%) who underwent enema reduction and 4 patients (80.0%) who underwent surgical closed reduction (Table 4). Of the patients treated with surgical manual reduction, non-enteric adenovirus group C was detected in 4 patients (2 patients with AdV-1, 1 patient with AdV-5, and 1 patient with AdV-6), and no virus was detected in 1 patient (Table 4). There were no significant intergroup differences in the frequency of enema reduction within 24 hours after onset of symptoms and the success rate of enema reduction (Table 4).
Table 4.
Comparison of Variables in the Patients with Intussusceptions by Viral Isolates (n=44)
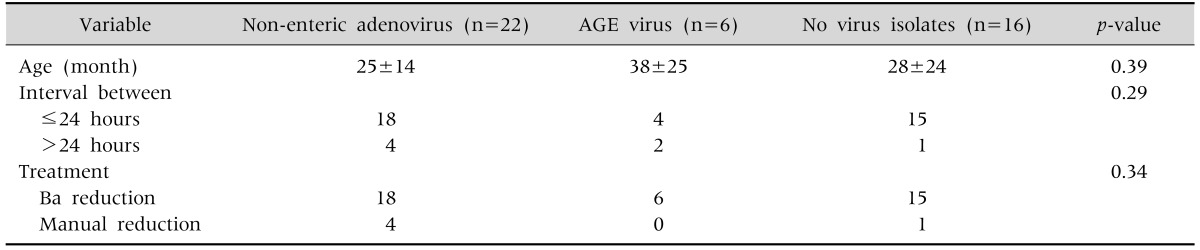
Values are presented as mean±standard deviation or number only. AGE virus: acute gastroenteritis virus including noro, spo, astro, enteric adeno, and rotavirus.
DISCUSSION
Our study is to investigate the detection rates of major acute gastroenteritis virus (norovirus, sapovirus, enteric adenovirus, astrovirus, and rotavirus) and non-enteric adenovirus and to determine whether differences exist in clinical features, blood test findings, and enema reduction results according to the type of virus detected in the stools of infants with idiopathic intussusception. The viral detection rate was 63.6%, with non-enteric adenovirus accounted for 50% and primary gastroenteritis virus comprising 13.6%, showing that the detection rate of non-enteric adenovirus was significantly higher. Norovirus comprised 2/3 of the primary gastroenteritis viruses detected. Among the three groups, in terms of clinical features, there were intergroup differences only in abdominal pain, with no differences revealed in other clinical features, blood test and enema reduction results.
The virus detection rate was 78.9% in the study of Okimoto et al. [6] which was higher than that in our study. This difference may be explained by the fact that this study limited detection target viruses to adenovirus and major primary gastroenteritis viruses, whereas Okimoto et al.'s study [6] recruited more types of viruses including adenovirus, enterovirus, calicivirus, and rotavirus. However, the detection rates of adenovirus and non-enteric adenovirus were 50.7% and 46.5%, respectively, similar to the detection rates in our study. Further, while the non-enteric adenovirus detection rate was high and the norovirus detection rate was low in patients aged over 2 years in Okimoto et al.'s study [6], the rate of non-enteric adenovirus detection did not differ and norovirus was detected more frequently in the same age group in our study. In Okimoto et al.'s study [6], AdV-1 (C1) and AdV-5 (C5) were dominant in the subgroup of non-enteric adenovirus in patients aged under 2 years, and AdV-3 (E3) and AdV-7 (E7) were dominant in patients aged above 2 years; however, this study revealed the dominance of AdV-1 (C1) and AdV-5 (C5) infection regardless of age, hence yielding different results. It is unclear from this study whether this discrepancy is the result of regional or seasonal differences due to different testing points.
The finding that viral pathogens were frequently detected in the stools of infants with intussusception implies that viruses play a vital role as an etiological factor in idiopathic intussusception, for which the cause remains unknown. Non-enteric adenovirus is most frequently related with idiopathic intussusception occurrence. Various other viruses have also been detected, including human herpes virus 6, cytomegalovirus, enterovirus, rhinovirus, norovirus, astrovirus, rotavirus, and others [5,6,8,9]. Rotavirus was detected in a few studies, but was not considered as the risk factor for intussusception [10,11]. Rotavirus was not detected in our study as well, which is consistent with the results of recent reports.
Regarding the pathophysiology of intussusception, an accepted hypothesis is that Peyer's patch swelling and lymph node hypertrophy caused by a viral pathogen in the ileum act as lead points [2,8]. The finding that concurrent adenovirus and human herpes virus 6 infection also increases the risk of intussusception indicates that viruses play a pivotal pathogenic role [8]. Another suggested hypothesis was that the reason for the increase of intussusception occurrence within 2 weeks of Rotashield vaccination of infants under the age of 1 year is reactive lymphoid hyperplasia of the ileum acting as the lead point due to vaccination [3]. However, Peyer's patch swelling did not appear to act as an anatomical lead point in a murine model [12]. Therefore, it is uncertain whether an enlarged Peyer's patch is the lead point or the result of intussusception. Kaemmerer et al. [13] suggested peristalsis disorders caused by inflammatory neuropathy triggered by adenovirus infection as an additional pathophysiological mechanism. Further research is necessary in this regard.
The cause of intussusception remains unclear, but the fact that it is subject to considerable seasonal variations, with an increased frequency in the winter with an increased risk of respiratory infections and in spring and summer with an increased risk of gastrointestinal viral infections, supports the assumption that infection could be an important causal factor in this disease [14,15]. However, seasonal variations may also be present depending on the research timeframe and region studied. During the timeframe that our study was conducted, from March 2012 to February 2013, most intussusception cases occurred from winter to early summer. This trend showed a pattern consistent with the frequency trend of virus detected in stools of intussusception patients. In particular, nearly all intussusception cases occurred during the highest occurrence periods of non-enteric adenovirus infection, March to July and December to February. These results could be evidence indirectly supporting the assumption that viral infection may be a crucial etiologic factor for intussusception development. Additionally, virus was not detected in 36.4% of intussusception patients in this study, this cannot be ruled out that the possibility of the involvement of other viruses that were not selected as detection targets. Interestingly, the seasonal adenovirus detection rate of the stool specimens of intussusception patients in this study showed a pattern similar to the monthly adenovirus detection rate in respiratory specimens in the same region, as revealed in the 2012-2013 respiratory virus occurrence report of the Korea Centers for Disease Control and Prevention [7].
While it is known that 80% of intussusception cases occur in infants under the age of 2 years, 45.5% occurred in children older than 24 months, yielding a different most frequently known affected age. This difference is assumed to be associated with the finding that the virus detection frequency was higher in patients aged above 24 months than that in patients aged below 24 months. In this study, the frequencies of vomiting and bloody stools in patients aged below 2 years were 45.5% and 25.0%, respectively. The high vomiting rate is consistent with the report of Park et al. [16], which showed that the vomiting frequency was higher and inversely correlated with age. However, the high occurrence rate of bloody stools differed from the results of other studies in which the rate decreased as the age decreased. This difference is due to the fact that glycerin enemas were performed uniformly on all suspected intussusception patients to collect the stool specimens in this study. In the study of Okimoto et al. [6], the abdominal pain frequency was high and the bloody stool frequency was low among patients in which adenovirus was detected. Abdominal pain was present in all adenovirus detection cases in this study, and the bloody stool frequency was lower than that of the no virus group, albeit statistically insignificant. In contrast, the frequency of abdominal pain in the primary gastroenteritis detection group was lower than that in the other 2 groups. While it is difficult to identify the reason for this difference, it is considered that the degree of intestinal obstruction caused by the overlapping intestines and mesenteric invagination may differ because of the different degree of Peyer's patch swelling in the ileum and surrounding mesentery as well as lymph node hypertrophy induced by viral infection.
The time from the onset of symptoms to the performance of enema reduction and its success rate were not correlated with the type of virus detected, but the non-enteric adenovirus subgroup C (AdV-1 in 2 patients, AdV-5 in 1 patient, and AdV-6 in 1 patient) was detected in the stools of 4 of 5 patients who underwent surgical reduction. This finding may be attributed to the higher detection rate in subgroup C, but it remains unclear whether the success rate of enema reduction in this subgroup was lower compared to that of other viruses. The limitations of our study are that it is a single center, uncontrolled trial with a small sample size and a short 1-year research period which may have affected the viral distribution in the stool samples depending on the trend of illness, and that the included viruses are limited to adenovirus and primary gastrointestinal virus. Therefore, a multicenter trial with a larger sample size and more target viruses is necessary.
In conclusion, the virus detection rate was high in Korean children with intussusception, with non-enteric adenovirus subgroup C comprising the majority of the cases investigated, followed by norovirus. Among the clinical features, the abdominal pain frequency differed depending on the virus detected, but no differences were observed in other symptoms and blood test results. Importantly, the seasonal trend in the detection rate of non-enteric adenovirus and norovirus coincided with the seasonal trend of intussusception occurrence, which suggests that viral infection plays a pivotal role as an etiological factor for intussusception development. Future research is warranted.
ACKNOWLEDGEMENTS
This study was supported by Chungnam National University Hospital Research Fund, 2011.
References
- 1.Fischer TK, Bihrmann K, Perch M, Koch A, Wohlfahrt J, Kåre M, et al. Intussusception in early childhood: a cohort study of 1.7 million children. Pediatrics. 2004;114:782–785. doi: 10.1542/peds.2004-0390. [DOI] [PubMed] [Google Scholar]
- 2.Kombo LA, Gerber MA, Pickering LK, Atreya CD, Breiman RF. Intussusception, infection, and immunization: summary of a workshop on rotavirus. Pediatrics. 2001;108:E37. doi: 10.1542/peds.108.2.e37. [DOI] [PubMed] [Google Scholar]
- 3.Murphy TV, Gargiullo PM, Massoudi MS, Nelson DB, Jumaan AO, Okoro CA, et al. Intussusception among infants given an oral rotavirus vaccine. N Engl J Med. 2001;344:564–572. doi: 10.1056/NEJM200102223440804. [DOI] [PubMed] [Google Scholar]
- 4.Zanardi LR, Haber P, Mootrey GT, Niu MT, Wharton M. Intussusception among recipients of rotavirus vaccine: reports to the vaccine adverse event reporting system. Pediatrics. 2001;107:E97. doi: 10.1542/peds.107.6.e97. [DOI] [PubMed] [Google Scholar]
- 5.Bines JE, Liem NT, Justice FA, Son TN, Kirkwood CD, De CM, et al. Risk factors for intussusception in infants in Vietnam and Australia: adenovirus implicated, but not rotavirus. J Pediatr. 2006;149:452–460. doi: 10.1016/j.jpeds.2006.04.010. [DOI] [PubMed] [Google Scholar]
- 6.Okimoto S, Hyodo S, Yamamoto M, Nakamura K, Kobayashi M. Association of viral isolates from stool samples with intussusception in children. Int J Infect Dis. 2011;15:e641–e645. doi: 10.1016/j.ijid.2011.05.008. [DOI] [PubMed] [Google Scholar]
- 7.Korea Centers for Disease Control & Prevention. Influenza and respiratory virus report No. 195-247 [Internet] Osong: Korea Centers for Disease Control & Prevention; 2012~2013. [cited 2013 Sep 1]. Available from: http://www.cdc.go.kr/CDC/info/CdcKrInfo0502.jsp?menuIds=HOME001-MNU0003-MNU0048-MNU0050. [Google Scholar]
- 8.Lappalainen S, Ylitalo S, Arola A, Halkosalo A, Räsänen S, Vesikari T. Simultaneous presence of human herpesvirus 6 and adenovirus infections in intestinal intussusception of young children. Acta Paediatr. 2012;101:663–670. doi: 10.1111/j.1651-2227.2012.02616.x. [DOI] [PubMed] [Google Scholar]
- 9.Jakab F, Péterfai J, Verebély T, Meleg E, Bányai K, Mitchell DK, et al. Human astrovirus infection associated with childhood intussusception. Pediatr Int. 2007;49:103–105. doi: 10.1111/j.1442-200X.2007.02293.x. [DOI] [PubMed] [Google Scholar]
- 10.Velázquez FR, Luna G, Cedillo R, Torres J, Muñoz O. Natural rotavirus infection is not associated to intussusception in Mexican children. Pediatr Infect Dis J. 2004;23(10 Suppl):S173–S178. doi: 10.1097/01.inf.0000142467.50724.de. [DOI] [PubMed] [Google Scholar]
- 11.El-hodhod MA, Nassar MF, Ezz ES, Ahmed EF. Rotavirus fecal antigen retrieval in infantile intussusception. Eur J Clin Microbiol Infect Dis. 2008;27:879–881. doi: 10.1007/s10096-008-0506-6. [DOI] [PubMed] [Google Scholar]
- 12.Peter G, Myers MG National Vaccine Advisory Committee; National Vaccine Program Office. Intussusception, rotavirus, and oral vaccines: summary of a workshop. Pediatrics. 2002;110:e67. doi: 10.1542/peds.110.6.e67. [DOI] [PubMed] [Google Scholar]
- 13.Kaemmerer E, Tischendorf JJ, Steinau G, Wagner N, Gassler N. Ileocecal intussusception with histomorphological features of inflammatory neuropathy in adenovirus infection. Gastroenterol Res Pract. 2009;2009:579501. doi: 10.1155/2009/579501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hsu HY, Kao CL, Huang LM, Ni YH, Lai HS, Lin FY, et al. Viral etiology of intussusception in Taiwanese childhood. Pediatr Infect Dis J. 1998;17:893–898. doi: 10.1097/00006454-199810000-00009. [DOI] [PubMed] [Google Scholar]
- 15.Selvaraj G, Kirkwood C, Bines J, Buttery J. Molecular epidemiology of adenovirus isolates from patients diagnosed with intussusception in Melbourne, Australia. J Clin Microbiol. 2006;44:3371–3373. doi: 10.1128/JCM.01289-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Park BC, Kim SY, Jung SJ. A comparative analysis of clinical features and treatment outcomes of intussusception according to age distribution. Korean J Pediatr Gastroenterol Nutr. 2005;8:150–156. [Google Scholar]