

Abstract
This study aimed to provide fundamental data to be utilized in preventing and treating musculoskeletal disorders and analyzing working postures commonly used during periodontal treatment. [Subjects] The subjects were three dental hygienists with work experience in dental clinics for more than 10 years. [Methods] For the analysis of working postures, we simulated the work posture of dental hygienists during the scaling procedures and oral radiographic imaging tasks. The subjects were recorded on video to precisely observe them while they were working. The captured working postures were assessed and analyzed using ergonomic assessment methods, the Rapid Entire Body Assessment, Rapid Upper Limb Assessment, and Strain index. [Results] No differences were exhibited in the intensities of manual scaling and ultrasonic scaling. Commonly, the shoulders and waist were found to be the most overburdened. According to the strain index, manual scaling and ultrasonic scaling working postures were identified to be most dangerous. [Conclusion] The work postures of dental hygienists during scaling are postures that are highly likely to generate work-related musculoskeletal disorders. Therefore, the development of therapeutic exercise programs easily performable in the workplace and daily life is thought to be crucial to prevent work-related musculoskeletal disorders.
Key words: Dental hygienist, Musculoskeletal disorder, Ergonomic risk factor
INTRODUCTION
When the aspects of diseases were examined by work characteristics of the Korean people, the percentage of population with musculoskeletal disorders accounted for 44.8% of all work-related diseases in 2004. Moreover, the percentage increased to 71.5% in 2009, increasing by 51.6% points during the past 6 years1). Musculoskeletal disorders surged by 193% in 2000 compared with 1999 and rapidly increased by 148% in 2003 compared with 2002, showing a drastically increasing trend. Direct compensation expense was KRW 5.9 billion for musculoskeletal disorders in 2000 including expenses for medical care and others. However, the expense has increased to KRW 155.6 billion, surging by about 25.4 times. The medical costs spent on musculoskeletal disorders are considerably large nationally and socially2). By taking direct and indirect costs into consideration, musculoskeletal disorders have drawn attention as one of the major industrial accidents. To resolve musculoskeletal disorders prevailing in workers, new legislation has been enacted since 2005, and Korea has initiated measured for the prevention and management of work-related musculoskeletal disorders3). Based on this legislation, physical therapists have worked in different industrial fields for work movement analysis and organized educational programs to prevent work-related musculoskeletal disorders. Thus, areas worked on by physical therapists have been expanded as well. In particular, hand and arm disorders, such as carpal tunnel syndrome and tendonitis, are the most common causes of disability retirement among dentists and dental hygienists4, 5). Dental hygienists may be at greater risk than dentists for developing upper extremity musculoskeletal disorders in the neck, shoulders, upper extremities, and lower back due to the long hours of periodontal work (dental scaling and root planning)6, 7). The tasks of dental hygienists consistently impose static force on the muscles for a long period of time due to periodontal work performed in a posture with the neck bent, waist twisted, and arms raised. This unique posture leads to continuous muscle tension due to the static force imposed on the muscles, which results in long-term generation of pain in the musculoskeletal system8). Furthermore, dental hygienists work in a chair-side sitting position, with variation as to the “clock positions” to get optimal visibility and accessibility to the different parts of the oral cavity during treatment of the patient9). According to domestic studies, 26.5% to 30.9% of dental hygienists have musculoskeletal disorder symptoms10), and according to the American Dental Association, more than 20% of dental hygienists have problems in the musculoskeletal system11). In addition, 6 to 8.5% of dental hygienists are known to suffer from carpal tunnel syndrome (CTS)12). Most previous studies were confined to analyzing the current status of musculoskeletal disorders. Detailed studies on physical factors such as dental instruments and work environment have been rarely performed on the musculoskeletal disorders of dental hygienists13). The main cause for the problems of the musculoskeletal system in dental hygienists is work environment such as unit chair and instruments14, 15). The work environment of dental hygienists, including such things as the unit chair and dental instruments has been point out as the main factor inducing the problems of the musculoskeletal system14). Other factors are instrument materials, hand force required depending on instrument surface texture and glove type, upper and lower limb postures of dental hygienists during scaling work, maintaining and operating devices with heavy force, and others15).
The study authors thought that a systematic analysis of working postures inducing musculoskeletal disorders in dental hygienists is very crucial in organizing therapeutic exercises, educational programs, and physical therapy programs to prevent work-related musculoskeletal disorders. Therefore, this study aimed to contribute to the advancement of industrial physical therapy by providing fundamental data to be utilized in preventing and treating musculoskeletal disorders and analyzing working postures commonly used during periodontal treatment via an ergonomic approach.
SUBJECTS AND METHODS
This study examined three dental hygienists with work experience in dental clinics for more than 10 years and without orthopedic and neurological problems. Subjects were fully explained the goals, purposes, and procedures of the study based on the Declaration of Helsinki, and we included the subjects after obtaining voluntary informed consent. Subjects were right-handed and working in general practice dentistry with prophylactic and periodontal treatment. Their mean age was 42 (range 41–43) years, mean was height 163 cm (range 160–166), mean weight was 55 kg (range 53–57), and mean duration of employment was 12 years (range 10–13 years). The study was conducted in the practice room of the Department of Dental Hygiene at Kangwon National University in Korea. For the analysis of working postures, we simulated the work postures of dental hygienists during scaling procedures and oral radiographic imaging tasks. Before shooting video for the working posture analysis, subjects adjusted the unit chair and height of their chair so that they could work in their usual postures; a practice mannequin was used and the patient. To analyze the movement involved during scaling procedures, subjects were asked to take manual scaling and ultrasonic scaling working postures. Scaling was conducted with the generally used “clock position” on the mannequin head. The movement involved in scaling all then teeth was evaluated depending on the position of the operator based on the mannequin head by dividing the position into the near side and far side. Subsequently, the near side was set as the seven-o'clock direction, and the far side was set as the eleven-o'clock direction of the operator16). Oral radiographic imaging movement was simulated in the oral X-ray room of Kangwon National University for the analysis of postures taken during the radiography. Video was recorded from the right, left, and front sides to precisely observe the joint movements involved during radiography. Based on these data, we captured and repeatedly analyzed the working postures judged to be imposing the most burdens on the body three times. The captured working postures were assessed and analyzed using ergonomic assessment methods, the Rapid Entire Body Assessment (REBA) and Rapid Upper Limb Assessment (RULA). Three professors of industrial safety conducted the analysis to preserve the objectivity of the study. The professors assessed the scores through discussion and analyzed the different categorized working postures.
REBA was developed for the purpose of analyzing the degree of exposure of the body to physical burden and risk factors in the service industry including nursing, cleaning, and others with dynamic and unpredictable work postures. Different factors including repetition, static work, working postures, duration of working hours, and others were evaluated by groups, Group A (trunk, neck, leg) and Group B (humerus: shoulder, forearm, wrist), using recorded video and direct observation. It categorizes the dangerous levels into 5 stages using a grading system with a 15-point scale and suggests appropriate measures17). RULA enables convenient and swift assessment of workload imposed by working postures by focusing on upper limb analysis in assembling, servicing, meat processing, dental clinic work, and VDT tasks especially involving the shoulders, wrists, neck, and others. It divided the body parts into Group A (upper arm, lower arm, wrist) and Group B (neck, trunk, legs) and assessed them in terms of the number of movements, static muscle work, force, and working postures as workload parameters. It categorizes the dangerous levels into 4 stages using a grading system with a 7-point scale and suggests appropriate measures18).
The strain index (SI) is a method of evaluating jobs to determine if they expose workers to increased risk of developing musculoskeletal disorders of the distal upper extremity (DUE)19). The DUE is defined as the elbow, forearm, wrist, and hand. Musculoskeletal disorders of the DUE include specific diagnoses (e.g., epicondylitis, peritendinitis, tendon entrapment at the wrist or finger, and carpal tunnel syndrome) and less specific symptomatic conditions related to the muscle-tendon units of the DUE. The strain index uses six task variables to describe hand exertions: intensity of exertion, duration of exertion, exertions per minute, hand/wrist posture, speed of work (how fast), and duration per day. Among those factors, exertion is evaluated as the most serious risk factor. An SI higher than 5 indicates the occurrence of potential upper extremity disease. An SI below 3 indicates safe, while an SI above 7 is considered very dangerous.
RESULTS
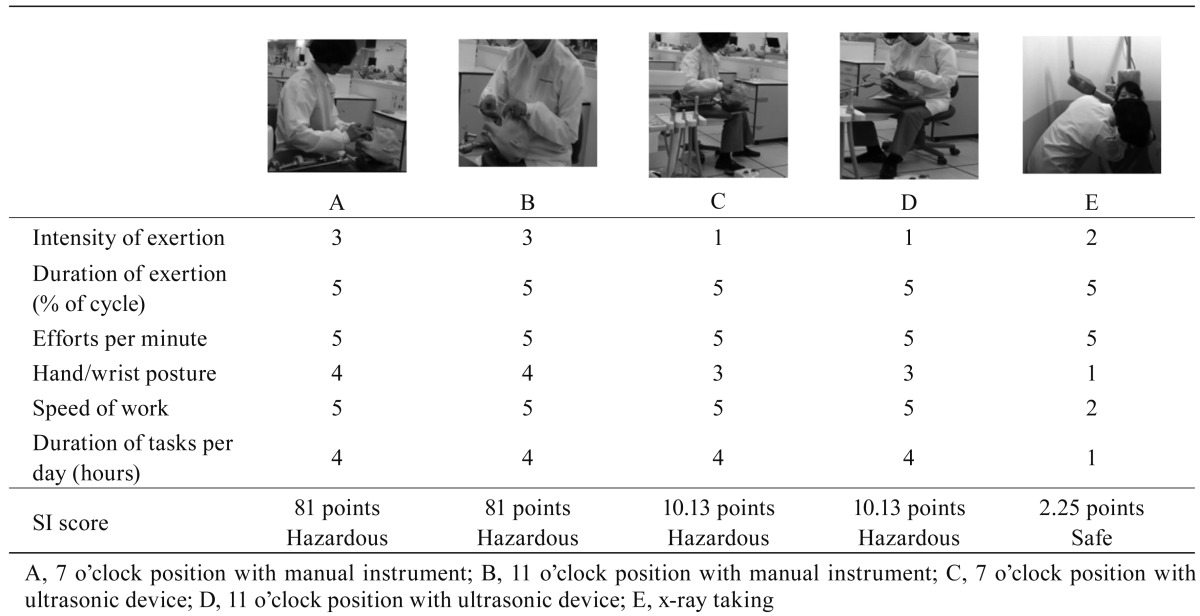
This study was performed to analyze the working postures of dental hygienists for the prevention and treatment of musculoskeletal disorders. We examined postures involved in scaling and radiography, and analyzed the evaluated scores of postures categorized by waist, neck, legs, shoulders, elbows, wrists, wrist twist, workload, grab, and activity. According to the results, “needs to be improved soon” was shown in the 7-o'clock direction analyzed with REBA in manual scaling and ultrasonic scaling working postures, and overload was detected in the work tasks of the shoulders, waist, and wrists. Moreover, “requires precise exam and immediate improvement” was found in RULA, and overload was detected in the waist, neck, shoulders, and wrists (Table 1). Among scaling working postures, the 11-o'clock direction analyzed with REBA was found to be “necessary,” and the shoulders were found to be the most overburdened. In addition, overload was detected in work tasks of the waist and wrists. “Requires precise exam and immediate improvement” was found in RULA, and the shouldres and wrists were found to be the most overburdened. Overload was detected in work tasks of the waist and neck (Table 1).
Table 1. Scaling position of the clinician.

Therefore, no differences were exhibited in the intensity of manual scaling and ultrasonic scaling performed from the 7-o'clock and 11-o'clock directions. Commonly, the shoulders and waist were found to be the most overburdened, and overload was frequently observed in the neck and wrists. “Needs to be immediately improved” was commonly detected in REBA and RULA with respect to working postures in oral radiography. Overburden was found in the order of the waist, shoulder, and wrist in REBA, while the waist followed by the neck and then the wrist were found to be the most overloaded in URLA (Table 2).
Table 2. Oral x-ray taking position.

According to the strain index, manual scaling and ultrasonic scaling working postures were identified to be the most dangerous. On the other hand, radiography postures were identified to be the most safe. Consequently, work postures during the scaling procedures are highly likely to generate various work-related musculoskeletal disorders in hygienists (Table 3).
Table 3. Strain inde.
This study was performed to analyze the working postures of dental hygienists for the prevention and treatment of musculoskeletal disorders. In manual scaling and ultrasonic scaling working postures, “needs to be improved soon” was found in REVA and “requires precise exam and immediate improvement” was found in RULA when analyzing the 7-o'clock working posture. Meanwhile, “requires improvement” was found in RULA and “requires precise exam and immediate improvement” was found in RULA when analyzing at the 11-o'clock working posture. Since manual scaling and ultrasonic scaling working postures were identified to be the most dangerous according to the strain index, the potential progress of musculoskeletal disorders was relatively higher in scaling procedures. According to an ergonomic analysis of Jung20), scaling tasks was verified to raise the risk of musculoskeletal disorders, aligning with the outcome of our study. No differences were observed in the potential risk of musculoskeletal disorders between manual scaling and ultrasonic scaling from the 7-o'clock and working postures. Commonly, the shoulders and waist were found to be the most overburdened, and overload was frequently observed in the neck and wrists.
Manual scaling and machinery (use of ultrasonic scaling and handpieces) showed higher loads on the trapezius muscles with regard to muscular rest, as well as the 10th and 50th percentiles were observed, than the other tasks, and for the forearm extensor muscles, an almost complete lack of muscular rest (0.1% time), and much higher loads regarding the 10th and 50th percentiles were observed9). However, the results of this study were slightly different from those of a study reporting that less stress was imposed on the muscles during ultrasonic scaling compared with manual scaling by reducing the workload in the right forearm extensors by approximately 50%. Inappropriate postures may induce various pains and body fatigue more quickly in static working postures because more than 50% of the muscles contract to resist gravity21).
Moreover, static works have a higher probability to generate disorders in the cervical spine compare with other works involving dynamic motions since most working postures in dental treatment impose static force on the muscles due to bending of the neck and raising of the arms8). Oral radiographic imaging postures were identified as “needs to be improved immediately” in REBA and RULA. In contrast, the same postures were found to the most safe in terms of the level of tension while working, exhibiting considerably contradictory results. Although oral radiography is performed in a short period of time, it requires excessive motions of upper extremities and the neck. For this reason, “needs to be improved immediately” seemed to be observed in the measures of REBA and RULA.
Fig. 2.
Place your hand with the palm facing the ceiling and the fingers downward as far as possible, not including the thumb.
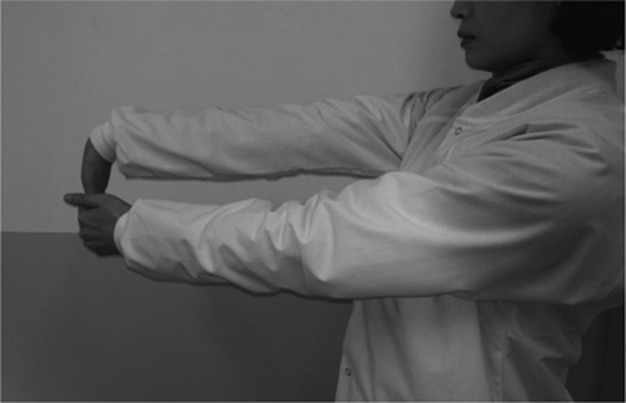
Fig. 3.

Stretch both arms outward from the body and perform repeatedly wrist flexion/extension.
Fig. 4.

Shoulder stretch: Clasp your hands behind your back and pull your arms up as high as you can.
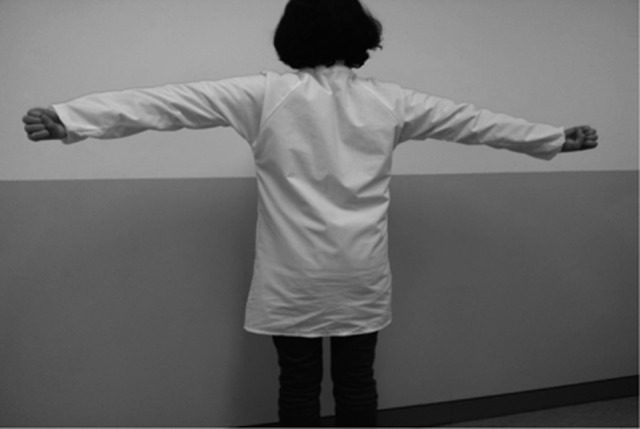
Fig. 5.

Draw your arms in as close as possible to the upper back and draw the scapulas in as much as you can.
Fig. 6.
Raise your arms at shoulder height and make a fist. Twist your fists backwards and forwards quickly.
Fig. 7.
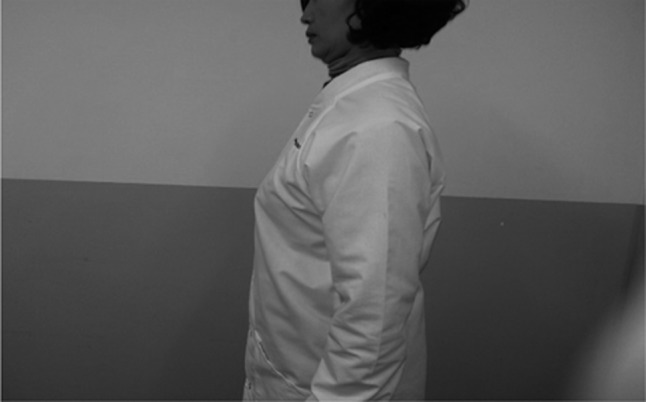
Draw your chin down and stretch your neck longer. Move your head backwards until your ears are behind the line extending upward from the shoulders.
Low scores were shown for work intensity, speed, and hours in the strain index. Since oral radiographic imaging postures require a wide range of motion in the waist and shoulders and do not necessitate for a long time, differences were attributable to the assessment methods.
This study performed an ergonomic analysis of the work postures of dental hygienists during scaling and radiography procedures and identified that the work postures are highly likely to generate work-related musculoskeletal disorders. However, radiographic imaging postures seemed to have a low possibility to generate chronic musculoskeletal disorders. Based on the ergonomic analysis, the development of therapeutic exercise programs easily performable in the workplace and daily life is thought to be crucial to prevent work-related musculoskeletal disorders. Darby and Walsh proposed strengthening and stretching exercises applicable to pelvis, knee, neck, wrist, finger, and others16). Therefore, exercise is anticipated to be essential to strengthening the forearms and providing the stability necessary for the mobility of the wrist and fingers, and to the ability of the low back and abdominal region to withstand gravity loads for a long period. In addition, stretching exercise is also crucial for the wrists and fingers when they need to perform and rapid movements. Quick stretching exercise seemed to be essential before performing oral radiography requiring a wide range of movement and complex working posture. Based on these results, composed some stretching and strengthening exercises were created22) (Figs 1–8).
Fig. 1.

Finger stretch and muscle strengthening: Bend and the IP joints of the four fingers, not including the thumb (10 times).
Fig. 8.

Stand against the wall like you are at the top position when performing push-ups.
REFERENCES
- 1.Kim KS, Park JK, Kim DS: Status and characteristics of occurrence of work-related musculoskeletal disorders. J Ergon Socie Kore, 2010, 29: 405–422 [Google Scholar]
- 2.Kim DS, Kim KS, Park JK: Evaluation of musculoskeletal disorder prevention management program operating. KIE Spring Conference Proceeding, 2010, 6: 1529–1535.
- 3.Park KH, Jung BY: Characteristics and causes of musculoskeletal disorders for employees aged 50 years or older. J Ergon Socie Kore, 2009, 28: 139–145 [Google Scholar]
- 4.Anton D, Rosecrance J, Merlino L., et al. : Prevalence of musculoskeletal symptoms and carpal tunnel syndrome among dental hygienists. Am J Ind Med, 2002, 42: 248–257 [DOI] [PubMed] [Google Scholar]
- 5.Gilles MA, Wing AM: Age-related changes in grip force and dynamics of hand movement. J Mot Behav, 2003, 35: 79–85 [DOI] [PubMed] [Google Scholar]
- 6.Hui D, Peter L, Alfredo V, et al. : Pinch forces and instrument tip forces during periodontal scaling. J Periodontol, 2007, 38: 525–531 [DOI] [PubMed] [Google Scholar]
- 7.Rice VJ, Nindl B, Pentikis JS: Dental workers, musculoskeletal cumulative trauma, and carpal tunnel syndrome, who is at risk? Int J Occup Saf Ergon, 1996, 2: 218–233 [DOI] [PubMed] [Google Scholar]
- 8.Kilbom A, Persson J: Work technique and its consequences for musculoskeletal disorders. Ergonomics, 1987, 30: 273–279 [DOI] [PubMed] [Google Scholar]
- 9.Åkesson I, Balogh I, Hansson GÅ: Physical workload in neck, shoulders and wrists/hands in dental hygienists during a work-day. Appl Ergon, 2012, 43: 803–811 [DOI] [PubMed] [Google Scholar]
- 10.Jung SH: Study on subjective symptoms and diagnosis of work-related musculoskeletal disorders experienced by dental hygienists. Korea University master's thesis, 2004
- 11.Werner RA, Franzblau A, Gell N, et al. : Prevalence of upper extremity symptoms and disorders among dental and dental hygiene students. J Calif Dent Assoc, 2005, 33: 123–131 [PubMed] [Google Scholar]
- 12.Dong H, Barr A, Loomer P, et al. : The effects of periodontal instrument handle design on hand muscle load and pinch force. J Am Dent Assoc, 2006, 137: 1123–1130 [DOI] [PubMed] [Google Scholar]
- 13.Yoo JH, Ro HL, Lee MY: The musculoskeletal pain and inconvenient feeling during hand instruments with mannequin and intra-oral cavity in dental hygiene students. J Kore Soci Physi Med, 13: 247–254. [Google Scholar]
- 14.Crawford, L, Gutierrez G, Harber P: Work environment and occupational health of dental hygienists: a qualitative assessment. J Occup Enviro Med. 2005, 47: 623–632. [DOI] [PubMed] [Google Scholar]
- 15.Laroche C, Barr A.Dong H: Effect of dental tool surface texture and material on static friction with a wet gloved finger tip. J Biomech, 2007, 40: 697–701 [DOI] [PubMed] [Google Scholar]
- 16.Michele LD, Margaret W: Dental hygine theory and practice ED 2. Elsevier Science, USA, 2003, pp. 101–132. [Google Scholar]
- 17.Hignett S, McAtamney L: Rapid Entire Body Assessment (REBA). Appl Ergon, 2000, 31: 201–205 [DOI] [PubMed] [Google Scholar]
- 18.McAtamney L, Corlett E: RULA: a survey method for the investigation of work-related upper limb disorders. Appl Ergon, 1993, 24: 91–99 [DOI] [PubMed] [Google Scholar]
- 19.Moore JS, Garg A: The strain index: a proposed method to analyze jobs for risk of distal upper extremity disorders. Am Ind Hyg Assoc J, 1995, 56: 443–458 [DOI] [PubMed] [Google Scholar]
- 20.Jung YS: The ergonomic analysis on dental hygienists scaling treatment posture based on video pictures. Catholic University doctoral thesis, 2008
- 21.Jo YS: Review of the Occupational Hazards to Dental Personnel. J Kore Ind Heal Assoc, 1997, 16: 66–77 [Google Scholar]
- 22.Brill PW, Suffes S: Instant relief. Bantam books, USA, 2003, pp 76–94. [Google Scholar]