

Abstract
The right lung has three lobes and two fissures while the left lung has two lobes and one fissure. During a routine dissection we observed a variant complete fissure and three incomplete fissures in the right lung while the left lung presented with a variant transverse fissure separating the superior lingual and anterior bronchopulmonary segments. In the right lung, the incomplete fissures lie between the apical and posterior bronchopulmonary segments; medial and lateral bronchopulmonary segments; apical and basal bronchopulmonary segments. The complete variant fissure separates the medial basal bronchopulmonary segment from the remaining basal segments. Such variant fissures and lobes are clinically important in cases of lobotomy.
Keywords: Bronchopulmonary segments, Lobotomies, Lung Fissure, Lung
Implications for Practice
Several reports have revealed that variations exist in the classical presentation of the fissures and lobes of the lungs.
This case report further reveals some of the unique variants that affect some of the bronchopulmonary segment.
These variants in fissures and lobulation can confuse a radiologist during routine X-ray or CT scans.
Background
The dissected lung surface is divided into lobules by dark lines. The lobule corresponds to the bronchopulmonary segment which is the functional unit of the lung. The right lung and left lung are separated into lobes by an oblique fissure present in both lungs and a transverse fissure which is present only in the right lung. The oblique fissures commence 6cm below the apex of each lung, 2cm from the medial plane and at the level of the third and fourth spine of the vertebra.1 The transverse fissure overlies the fourth rib to meet the oblique fissure at the level of the mid axillary line. The presence of the transverse fissure results in three lobes on the right lung while the left lung presents two lobes. The three lobes on the right lung are named: superior, middle and inferior lobe while in the left lung only the superior and inferior lobe are present.1 The awareness of anatomical variations of lobes of the lung is essential because radiologists may misinterpret them on an X-ray or a CT scan. Such variations when known can help in planning lobectomies involving individual segment. Hence this case study aims to present the unique variations in the morphology of lung fissures and lobes observed during a routine dissection. This might serve to generate some new data regarding lung lobes and fissures which can be made available to surgeons to help in the appropriate planning of surgery.
Case presentation
This case of variant fissures and lobes of the right and left lungs were incidentally noted in the Anatomy Department of Bayero University Kano State of Nigeria during dissection of the thoracic region of an adult male cadaver of about 40 to 45 years of age. The medical history of the individual was not known. The lung fissures and lobes were studied and the variant fissures and lobes were noted. The lungs specimens were photographed (Figures 1- 3).
Figure 1. Photograph of the anterior surface of the right lung showing: IVF: Incomplete variant fissure; OF: Oblique fissure; MBPS: Medial Bronchopulmonary Segment of the middle lobe; IVOF: Incomplete Variant Oblique fissure; LBPS: Lateral Bronchopulmonary Segment of the middle lobe; TF: Transverse fissure .
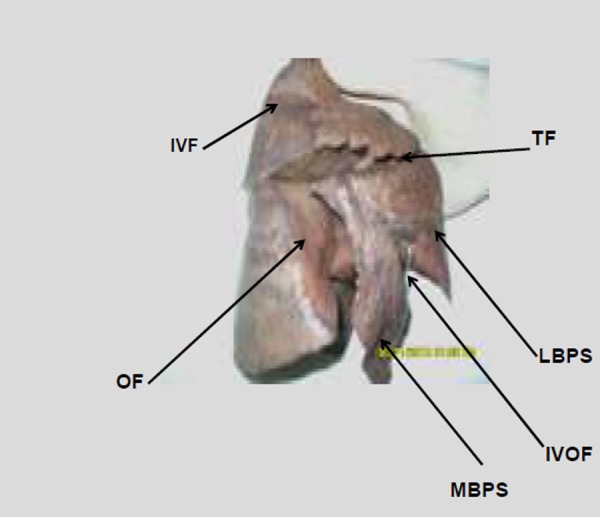
The right and left lungs displayed the classical oblique fissure (Figure 1a and Figure 4a), which normally commence from a distance of 7cm from the apex of the lung on the vertebral part of the medial surface to cross the inferior border at a distance of 2cm from the anterior border. The conventional transverse fissure (Figure 1b) was also noted in the right lung which during life normally passes transversely along the level of the fourth rib to meet with the oblique fissure at the mid axillary line. Three incomplete variant fissures were observed in the right lung as shown in Figures Figure 1, 2, and 3. The left lung presents one variant transverse fissure which is shown in Figure 4.
Figure 2. Photograph of the inferior surface of the right lung showing the complete variant fissure (CVF) separating the medial basal bronchopulmonary segment (MBBPS) from the remaining basal segments.
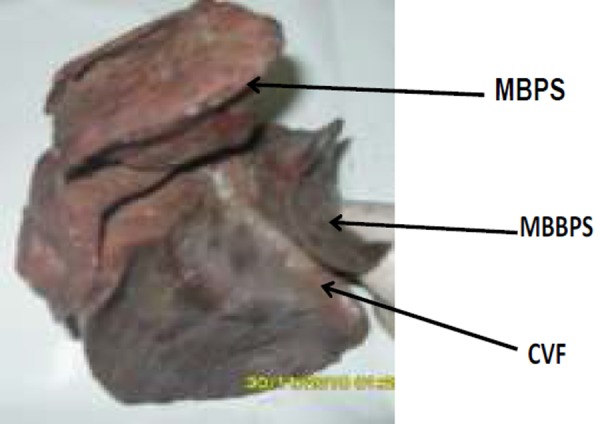
Figure 3. Photograph of the anterior surface of the inferior lobe of the right lung showing the Incomplete Variant Fissure (IVF) apparently showing the demarcating line between the apical and the basal segments of the inferior lobe.

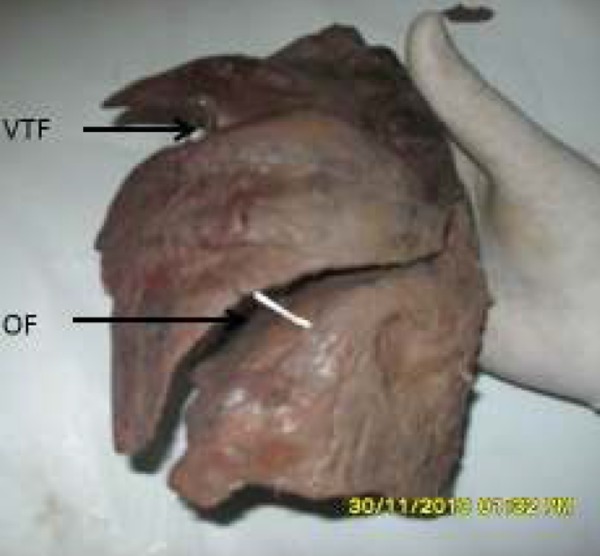
Figure 4. Photograph of anterior surface of the left lung showing: OF: oblique fissure; VTF: Variant transverse fissure.
In the superior lobe of the right lung the incomplete variant fissure present is believed to show where the apical bronchopulmonary segment separates from the anterior bronchopulmonary segment.
In the middle lobe the presence of the incomplete variant fissure was also noted and it is believed to denote the boundary of the medial and lateral bronchopulmonary segments of the middle lobe. This variant fissure extends inferiorly into the diaphragmatic and mediastinal surface of the right lung
In the inferior lobe, a variant fissure was also observed separating the medial basal bronchopulmonary segment from the remaining basal segments. The variant fissure extends forward to meet with the oblique fissure (Figure 2). Figure 3 presents another fissure in the inferior lobe which is an incomplete fissure that seems to denote the demarcating boundary between the apical bronchopulmonary segment and the basal bronchopulmonary segments of the inferior lobe. The left lung had a variant fissure at the superior lobe which demarcates the anterior bronchopulmonary segment from the superior lingular bronchopulmonary segment.
Discussion
All the variations noted in lobulation and fissures in both lungs might be as a result of altered pulmonary development.2 Meenakshi et al. in their study also revealed that the presence of a variant fissure could be due to the failure of obliteration of these fissures either completely or partially.3 The fissures and lobes of the lungs separate the main lobes of the lungs. These lobes develop during intra-uterine life by means of lung bud which divides into a right and left bronchi bud which later forms the corresponding right and left main bronchus. The right main bronchus will give rise to three secondary bronchi for the developing three lobes of the right lung while the left main bronchus will give rise to two secondary bronchi for the two developing lobes. The secondary bronchi of both lungs divide to form the tertiary bronchi which are the primordial structures of the bronchopulmonary segments. During intra-uterine life the individual segments are initially separated by fissures that fuse as the lungs develop, except along two planes that are represented as the oblique and horizontal fissures, as seen in the right lung and along one plane represented as the oblique fissure in the left lung.3,4 These fissures in the lung enable even expansion of the lung during respiration and are usually used as landmarks in specifying lesions.5 When a variant fissure is present as seen in the reported cases (Figures 1, 2, and 3) there is a potential for confusion when interpreting X-ray films. On occasions, such variant fissures may even be mistaken as a pleural effusion.3
The variant fissure which demarcates the medial basal segment and the superior incomplete fissure which demarcates the superior segment as observed in Figure 2 and Figure 3, respectively, have been reported to be the most common variant fissures that are detected on CT scans.6 The variant fissure separating the superior segment of the inferior lobe from the basal segment as shown in Figure 3 was described previously as the superior accessory fissure by Godwin and Tarver 1984.6 In the present reported case a variant fissure that was noted on the right lung can also be termed as a superior variant fissure. This type of fissure is reported to be more common in the right lung.6 A variant fissure such as the one noted in Figure 1 and Figure 2 which separated the medial and lateral bronchopulmonary segments of the middle lobe and the medial basal segment from each basal segment respectively, may be of advantage because it might help to limit the spread of infection.3
The knowledge of variant fissures is very important especially in the pre-operative planning of lobectomy. Once the presence of a variant fissure is noted the procedure for a segmental resection may also have to change to avoid the post-operative complication of air leakage.7 In X-rays of the lungs, variant fissures always give the semblance of pleural effusion whereas in CT scans they might not even be detected. 8
This present case of variations in the fissures of lungs might help to explain certain unusual X-ray presentation of the lung. Similarly, it might help to understand certain radiographic findings such as extension of fluid into a variant fissure and the spread of diseases through different pathways in the lungs.9
ACKNOWLEDGEMENTS
We are grateful to all the technologists of the Department of Anatomy, Faculty of Medicine, Bayero University Kano-Nigeria
Footnotes
PEER REVIEW
Not commissioned. Externally peer reviewed.
CONFLICTS OF INTEREST
The authors declare that they have no competing interests.
ETHICS COMMITTEE APPROVAL
Cadavers used in Nigerian Universities are composed of unclaimed unidentified bodies. The Nigerian police within the jurisdiction where the body was found gives approval for the release of the body for dissection purposes.
Please cite this paper as: Esomonu UG, Taura MG, Modibbo MH, Egwu AO. Variation in the lobar pattern of the right and lungs: A case report. AMJ 2013, 6, 10, 511- 514. http//dx.doi.org/10.4066/AMJ.2013.1856
References
- 1.Shah P, Johnson D, Standring S. In: Gray’s Anatomy. 39th ed. Edinburgh:Churchill Livingstone: 2005. Thorax; pp. 1068–1069. [Google Scholar]
- 2.Modgil V, Das S, Suri R. Anomalous lobar pattern of right lung: A case report. Int. J. Morphol. 2006;24:5–6. [Google Scholar]
- 3.Meenakshi S, Manjunath KY, Balasubramanyam V. Morphological variations of the lung fissures and lobes. Indian J Chest Dis Allied Sci. 2004 Jul-Sep;46(3):179–82. [PubMed] [Google Scholar]
- 4.Larsen WJ. Churchill Livingstone, New York: 1993. Human Embryology; pp. 111–30. [Google Scholar]
- 5.Yamashita H. Tokyo lgaku Shoin: 1978. Roentgenologic Anatomy of Lung; pp. 49–53. [Google Scholar]
- 6.Godwin JD, Tarver RD. Accessory Fissures of the Lung. AJR Am J Roentgenol. 1984;144:39–47. doi: 10.2214/ajr.144.1.39. [DOI] [PubMed] [Google Scholar]
- 7.Walker WS, Craig SR. A proposed anatomical classification of the pulmonary fissures. J R Coll Surg Edinb. 1997 1997 Aug;42(4):233–4. [PubMed] [Google Scholar]
- 8.Ariyurek OM, Gulsun M, Demirkazik FB. Accessory fissures of the lung: evaluation by highresolution computed tomography. Eur J Radiol. 2001 2001 Jan;37(1):54–9. doi: 10.1007/s003300100852. [DOI] [PubMed] [Google Scholar]
- 9.Dandy WE. Incomplete pulmonary interlobar fissure sign. Radiology. 1978;128:21–5. doi: 10.1148/128.1.21. [DOI] [PubMed] [Google Scholar]