

Abstract
In 1970, the first cephalosomatic linkage was achieved in the monkey. However, the technology did not exist for reconnecting the spinal cord, and this line of research was no longer pursued. In this paper, an outline for the first total cephalic exchange in man is provided and spinal reconnection is described. The use of fusogens, special membrane-fusion substances, is discussed in view of the first human cord linkage. Several human diseases without cure might benefit from the procedure.
Keywords: Fusogens, head transplantation, spinal cord reconstruction
“The impossible of today will become the possible of tomorrow”
Tsiolkovsky AT (1857-1935; Father of Astronautics)
In 1970, Robert White and his colleagues successfully transplanted the head of a rhesus monkey on the body of another one, whose head had simultaneously been removed. The monkey lived 8 days and was, by all measures, normal, having suffered no complications.[28] A few years later, he wrote: “…What has been accomplished in the animal model – prolonged hypothermic preservation and cephalic transplantation, is fully accomplishable in the human sphere. Whether such dramatic procedures will ever be justified in the human area must wait not only upon the continued advance of medical science but more appropriately the moral and social justification of such procedural undertakings.”[29] In 1999, he predicted that “…what has always been the stuff of science fiction - the Frankenstein legend, in which an entire human being is constructed by sewing various body parts together – will become a clinical reality early in the 21st century… brain transplantation, at least initially, will really be head transplantation – or body transplantation, depending on your perspective… with the significant improvements in surgical techniques and postoperative management since then, it is now possible to consider adapting the head-transplant technique to humans.”[30]
The greatest technical hurdle to such endeavor is of course the reconnection of the donor (D)'s and recipient (R)'s spinal cords. It is my contention that the technology only now exists for such linkage. This paper sketches out a possible human scenario and outlines the technology to reconnect the severed cord (project GEMINI). It is argued that several up to now hopeless medical conditions might benefit from such procedure.
HYPOTHERMIA PROTOCOL
The only way to perform a cephalic exchange in man is to cool the body-recipient (R)'s head to such a low temperature to allow the surgeons to disconnect and reconnect it to the donor (D)'s body, whose head has been removed in the same operating theater by a second surgical team. Once R's head has been detached, it must be joined to D's body, that is, it must be reconnected to the circulatory flow of D, within the hour.[29,30,31] Mammals can be sustained without blood flow for 1 hour at most when cooled to the accepted safe lower limit of 12-15°C: At a temperature of 15°C, the cerebral metabolic rate in man is 10% of normal. Recovery following circulatory arrest for as long as 1 hour has been reported at <20°C temperatures since the 1950s.[13,15] Profound hypothermia (PH) curtails the onset of global ischemia and give time to the surgeons to reconnect the bodies.
Clinical experience in cardiac surgery has demonstrated that total circulatory arrest under deep hypothermia (18°C) for 45 minutes produces virtually no discernible neurological damage, with a slight increase on approaching the hour.[16,34] Experience with surgical clipping of aneurysms shows the safety of the procedure.[22]
R's blood subjected to PH tends to become coagulopathic: Accordingly, R's head will be exsanguinated before linkage, and flushed with iced (4°C) Ringer's lactate.[2,13]
Hypothermia can be achieved in several ways,[2] but, in this particular endeavor, it will not involve total body extracorporeal circulation (TBEC), in order to avoid the attendant ill effects (brain damage and coagulopathy), and make the procedure as simple and as cheap as possible.
White developed a special form of PH, which he named autocerebral hypothermic perfusion (ACHP).[32] No pumps or oxygenators are called for [Figure 1]. The first patient submitted to this protocol was operated on in November 1968 for removal of a brain lesion. Here follows a short description.
Figure 1.
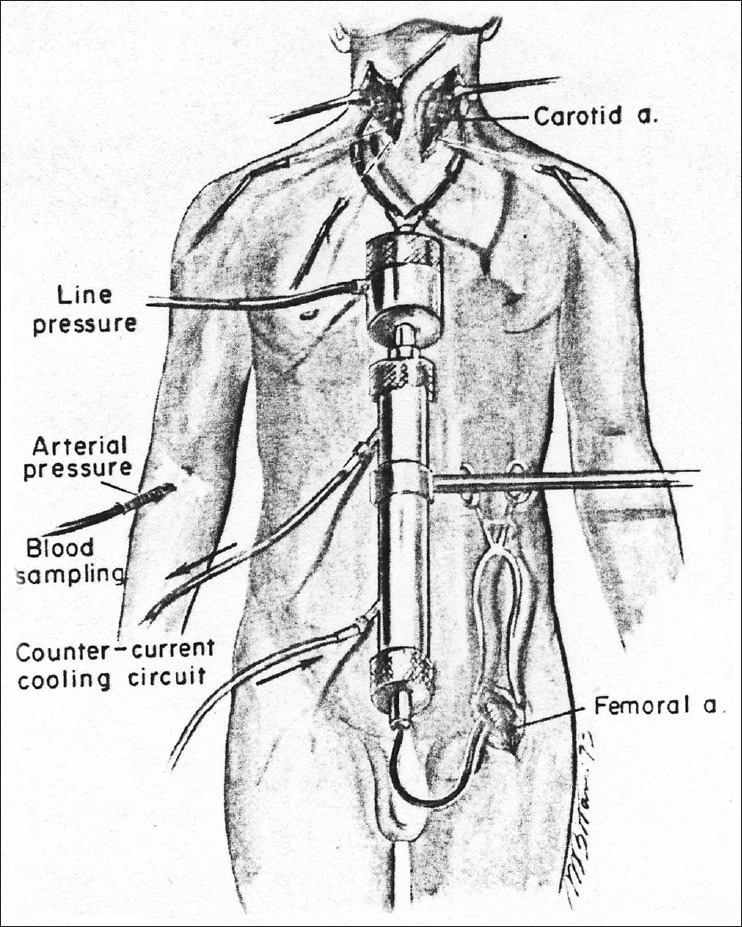
Drawing depicting White's autocerebral hypothermic perfusion in place (from White 1978)
After induction of anesthesia and intubation, and insertion of a cerebral 21G thermistor into the right parietal lobe and appropriate exposure, the common carotid arteries and their bifurcations were exposed. The two vertebral arteries were uncovered on each side of the neck as they coursed toward their body canals just caudal to the C6 body. Silk ligatures were passed around each individual artery and threaded through a short glass tube with a narrow opening and capped with a rubber tip for temporary nontraumatic occlusion. Following total body heparizination, the left femoral (F) artery and both common carotid (C) arteries were cannulated with small slightly curved metal cannulas (single carotid cannulation had been found to be unsafe in that it did not afford homogeneous bi-hemispheric cooling in monkeys). These were connected to each other via a pediatric Brown-Harrison high-efficiency heat-exchanger. Fluids of varying temperatures were circulated into the cylinder chamber around the tube containing the perfusing blood from a plastic reservoir using a sump pump. Under electroencephalography (EEG) control and with the F-C shunt open, each cervical artery was occluded beginning with the external carotids and ending with the closure of the vertebrals. With the demonstration that the shunt could maintain a normal EEG at normothermia, ACHP was instituted by altering the temperature of the fluid entering the heat-exchanger: After 48 minutes of perfusion, the intracerebral temperature had reached 11.4°C. Electrocortical activity invariably ceases with cortical temperatures below 20°C making the subject “brain dead”. Brain rewarming could be significantly retarded during the ischemic period by surrounding the head with ice. The patient made an uneventful recovery.
White[29,31] also experimented with biventricular cooling [Figure 2]. Here, two 18G ventricular cannulas are inserted in the anterior horn of each lateral ventricle through small burr holes in the skull and fixed with acrylic cement; a similar cannula is inserted percutaneously in the cisterna magna for egress of the perfusate. Sodium chloride (NaCl) solution (154 mmol/) at 2°C is perfused through both ventricular cannulas at a pressure of 80 cm/H2O and a flow of approximately 65 ml/min: <20°C can be achieved in about 30 minutes. This technique has been employed in man: It is rapid and easy and obviates vascular cannulation, extracorporeal routing of the circulation, and total body anticoagulation. No damage to the brain has been reported.
Figure 2.
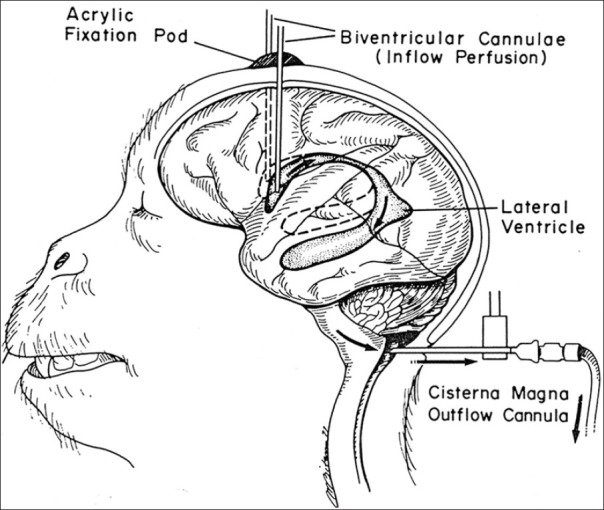
Drawing depicting biventricular cooling for deep brain hypothermia in a monkey (from White 1978)
Commercial cooling helmets are widely available[2] and similar contraptions helped White to lower and sustain brain temperature below 10°C consistently. With pressure maintained at >80 mmHg through catecholamines infusion, 15°C was achieved in <30’ in White's Rhesus experiments. No neurologic deficit was detected.
In HEAVEN, once D's circulation starts flowing into R's exsanguinated head, normal temperatures will be reached within minutes. A thermistor in the brain can be replaced by one placed in the temporalis muscle (TM), as this closely correlates with intraparenchymal brain temperature.[26] The anesthesiological management during hypothermia is outlined elsewhere.[34]
D's spinal cord will be selectively cooled, that is, no systemic PH will be necessary. With custom-built units,[1,24] the spinal subdural and epidural spaces can be perfused with cold solutions at 4-15°C, with rapid cooling and easily maintained at 10-15°C for several hours without neurologic sequelae [Figure 3]. Segmental hypothermia of the cervical cord produced no measurable temperature change of the brain.
Figure 3.
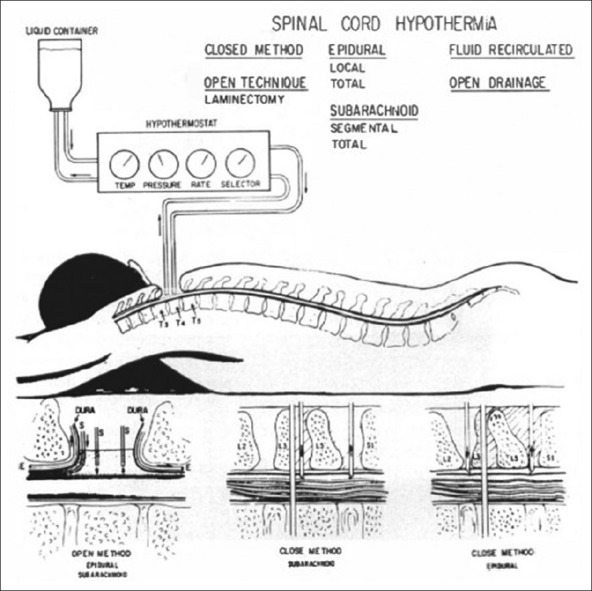
Depiction of various ways to locally cord the spinal cord (from Negrin 1973)
PROCEDURAL OUTLINE FOR CEPHALOSOMATIC SEPARATION IN RHESUS MONKEYS
In the seminal experiment,[28] a Rhesus monkey [Figure 4] was sedated, tracheotomized and mechanically respired, then transected at C4-C5 vertebral level. Surgical isolation was accomplished stepwise, under antibiotic coverage:
Figure 4.

Drawing depicting the first total cephalosomatic exchange in a monkey (from White et al. 1971)
Circumferential soft tissue and muscle were divided around the entire surface of the cervical vertebra with ligation and transection of the trachea and esophagus following appropriate intubation
Cervical laminectomy was performed at C4-C6 vertebral level with ligation and division of the spinal cord and its vasculature at C5-6. Following spinal cord division, an infusion of catecholamine was begun to counteract the hypotension of ensuing spinal shock with the maintenance of mean arterial pressure (MAP) 80-100 mmHg. Mechanical respiration was begun and continued throughout the experiment
The vertebral sinus was obliterated with judicious use of cautery and intravascular injection of fast-setting celloidin
Intraosseous destruction of the vertebral arteries was carried out
The vertebral body or interspace was transected. At this point, the head and body were completely separated save for the two neurovascular bundles
Each carotid artery and jugular vein in turn was divided and reconnected by means of a suitable sized tubing arranged in loops during constant EEG surveillance. Prior to cannulation, the preparation was heparinized and the vagi sectioned under ECG monitoring
For vascular transference of the cephalon to the new isolated body, the individual cannulas were occluded and withdrawn from the parent body carotid arteries and jugular veins (in sequence, allowing for continuous cerebral perfusion from one set of cannulas during the exchange) and replaced into the appropriate somatic vessel under EEG observation
Following successful cannula-vascular transfer, direct suture anastomosis of the carotid arteries and jugular veins was undertaken (silk 6-0 and 7-0, respectively) under the operating microscope. This permitted discontinuance of purposeful anticoagulation. Fresh monkey blood was available if significant losses were encountered under prolonged heparizination.
The monkey survived, neurologically intact, for 36 hours, having reacquired awareness within 3-4 hours.
With time, some blood loss was encountered from the muscles at the surfaces of surgical transection, due to chronic heparinization. The initial attempt to suture the vessels directly and thus eliminate the necessity of anticoagulation was only partially successful because of the constriction that developed in the jugular vein at the suture line, impeding venous return from the head.
No evidence of cellular changes compatible with a hyper-rejection reaction in cerebral tissue was seen on pathological examination up to 3 postoperative days.[29,31] The conclusion was that direct vascular suture will eliminate the long-term need for anticoagulation.
GEMINI: CORD ANASTOMOSIS
During the GEMINI procedure, the surgeons will cut the cooled spinal cords with an ultra-sharp blade: This is of course totally different from what happens in clinical spinal cord injury, where gross damage and scarring hinder regeneration. It is this “clean cut” the key to spinal cord fusion, in that it allows proximally severed axons to be “fused” with their distal counterparts. This fusion exploits so-called fusogens/sealants.
Several families of inorganic polymers (polyethylene glycol [PEG], nonionic detergents triblock copolymers, i.e., polymers of a PEG–propylene glycol–PEG structure: Poloxamers – e.g., poloxamer 188, 1107 – and poloxamines) are able to immediately reconstitute (fuse/repair) cell membranes damaged by mechanical injury, independently of any known endogenous sealing mechanism.[7] PEG (independent of molecular weight, 400-5000 being all equally effective) is both water-soluble and nontoxic in man; it can also seal the endothelium and wounds simply go dry during experimental laminectomy procedures.[20]
Originally, this “fusogenic” potential was exploited to induce the formation of hybridomas during the production of monoclonal antibodies as well as facilitating vesicular fusion in model membrane studies. Membrane fusion and attendant mixing of the cytoplasm of fused cells occurs when adjacent membranes touch in the presence of PEG or similar compound. Acute dehydration of the fusing plasmalemmas permits glycol/protein/lipid structures to resolve into each other at the outer membrane leaflet first and the inner membrane leaflet subsequently.[21] In other words, dehydration of the membrane facilitates the hydrophobic core of the lamellae to become continuous; rehydration after PEG exposure permits the polar forces associated with the water phase to help reorganize the structure of transmembrane elements. PEG is dislodged once the membrane is sealed. This reorganization of cellular water is believed to result from the strongly hydrophilic structure of PEG.
In contrast, triblock copolymers, which are mainly composed of PEG side chains around a high molecular mass hydrophobic core, act differently, namely, the hydrophobic head group inserts itself into the membrane breach, seal-plugging it.
The diameter of injured axons does not affect their susceptibility to repair by PEG: Both myelinated and unmyelinated axons are equally susceptible, but also neurons.
PEG is easy to administer and has a strong safety record in man, often employed as vehicle to clinically injected therapeutic agents.[33] P188 has also been utilized clinically in man without ill effects. Yet, the lower the molecular weight of PEG, the more toxic might be the by-products of degradation in the body (the monomer is very toxic) and thus only a molecular weight >1000 is totally safe in man.
Bittner et al.[5] were the first to show axonal fusion after complete axonal transection and data accrued since 1999 strongly point to the actual possibility of functional reconnection of the severed spinal cord.[7,12] In these experiments, immediate (within 2 minutes and in no case more than 3 minutes of disconnection) topical application to isolated severed (transected and reattached) guinea pig spinal cord white matter in vitro and both immediate topical or intravenous (IV) application of PEG in vivo reversed physiological conduction block and dramatically increased the number of surviving axons (i.e., the overall amount of spared white matter) to a similar degree. This was associated with an extremely rapid electrophysiological (100%) and/or behavioral (93%) recovery in mammals: The first action potentials are evident within 5’-15’.[7,12] In neurologically complete spinal cord injuries (SCI) in dogs, there was a significant and rapid recovery of conduction, ambulation, and sensibility.[7,12] Recovery is stable for at least a month and actually improves with time. In both dogs and guinea pigs, IV PEG still had effects, respectively, 72 and 8 hours after SCI (instead, rats could be salvaged at 2 and 4 hours, but not 6 hours, after brain injury: There was actually a worsening), but it should be stressed how IV injection of 30% PEG only increased the locomotor rating score by 0.7 out of a 21-point-scale compared with the controls receiving saline, partly due to the difficulty in delivering sufficient amount of agents to the injured site via systemic circulation. This is a clear indication for the need to use a topical approach. In any case, PEG appears to be superior to poloxamer 188. A successful phase I human trial of PEG on human volunteers has been completed.[12]
To sum up, no more than 2 minutes of application of PEG can fuse previously severed myelinated axons in completely transected spinal cords, enough to permit the diffusion of intracellular markers throughout the reconnected segments and immediate recover of conduction of compound action potentials lost after injury. Injected PEG crosses the blood–brain barrier and spontaneously targets areas of neural injury, without accumulating or lingering in undamaged tissues. Similarly, PEG injected beneath the perineural sheath near the lesion in peripheral nerves is effective in functional repair.[7,12]
Certainly, PEG-mediated plasma membrane resealing is incomplete: Compound action potentials are only 20% strong, owing to either leakiness to K+ or inability of PEG to target paranodal regions of clustered K+ channels likely exposed to demyelination. However, this can be partially offset by the administration of a specific agent, 4-AminoPyridine, a drug in clinical use, with doubling of recovered strength (40%).[12]
Fortunately, better ways to deliver PEG have been developed.
One involves self-assembled monomethoxy poly(ethylene glycol)-poly(D, L-lactic acid) [mPEG (2000)-PDLLA] di-block copolymer micelles (60 nm diameter), in which a PEG shell surrounds a hydrophobic inner core. These polymeric micelles, sizing from 10 to 100 nm, possess unique properties such as biocompatibility and long blood residence time, and have been widely investigated as nano-carriers of water-insoluble drugs.[12] Injured spinal tissue incubated with micelles showed rapid restoration of compound action potential into axons. Much lower micelle concentration is required for treatment than pure PEG. Injected mPEG-PDLLA micelles are significantly more effective than high-concentration PEG in functional recovery of SCI, likely due to prolonged blood residence of mPEG-PDLLA micelles.
Another way exploits monodispersed, mesoporous spherical PEG-decorated silica nanoparticles: These are hydrophilic, biocompatible, nontoxic, and stable. This colloid-based PEG derivative may do an even better job compared with polymer solution by controlling the density of PEG molecules at cord level.[12] Recovery of SSEP conduction after 15’-20’ following injection was seen in guinea pigs with transected cords.[25]
An alternative, possible better way to fuse severed axons has been described.[6] Methylene Blue is applied in hypotonic Ca++free saline to open cut axonal ends and inhibit their plasmalemmal sealing. Then, a hypotonic solution of PEG (500 mM) is applied to open closely apposed axonal ends to induce their membranes to rapidly flow into each other (PEG-fusion). Finally, Ca++-containing isotonic saline is applied to remove PEG and to induce endogenous sealing of any remaining plasmalemmal holes by Ca++-induced accumulation and fusion of vesicles. This technique has been applied to experimentally cut sciatic nerves in rats with excellent results.
Better agents than PEG have been identified and are available. Chitosan (poly-β-(1 → 4)-D-glucosamine) is a positively charged natural polymer that can be prepared by de-N-acetylation of chitin, a widely found natural biopolymer (crustaceans, fungi). It is biocompatible, biodegradable, and nontoxic. It is normally used as clinical hemostatic and wound healing agent in both gauze and granules. Chitosan appears superior to PEG: Chitosan in sterile saline (or otherwise nanoengineered nano/micro particles) can act as a potent membrane sealer and neuroprotector, being endowed with significant targeting ability.[12] Chitosan is capable of forming large phospholipid aggregates by inducing the fusion of small dipalmitoyl phosphatidylcholine (DPPC) bilayers, a major component of the plasma membrane.
Combining the actions of both chitosan and PEG leads to a newly developed hydrogel based on photo-cross-linkable chitosan (Az-C), prepared by partial conjugation of 4-azidobenzoic acid (ABA) to chitosan.[3] Chitosan hydrogel is attractive for use in GEMINI, due to its simplicity of application, tissue adhesiveness, safety, and biocompatibility. The Az-C network is reinforced by adding PEG (Az-C/PEG gel). Low-molecular-weight PEG with a nonreactive terminal group would be best. This gel can be applied as a viscous liquid that flows around the damaged cord temporarily held together. The gel precursor solution can be quickly cross-linked in situ by short-term UV illumination, covering the tubular part of the nerves and providing a reliable linkage during the healing process. The composite gels of PEG and Az-C have higher storage moduli and shorter gelation times than an Az-C gel or fibrin glue, and nerves anastomosed with an Az-C/PEG gel tolerate a higher force than those with fibrin glue prior to failure. These effects are likely due to the formation of a semi-IPN network, where PEG interpenetrates the covalent Az-C network and physically reinforces the network. Az-C/PEG gels are compatible with nerve tissues and cells. PEG is slowly released over a prolonged period, providing additional fusogenic potential.
A possible objection to GEMINI involves the supposed need for proper mechanical alignment (abutment) of the severed axons. The behavioral results of the PEG experiments, however, make a strong point that, while the number of axons reconnected to be expected is unknown, the results are nonetheless clinically meaningful, as highlighted by Bittner et al.[6] It is relevant to note how as little as 10% of descending spinal tracts are sufficient for some voluntary control of locomotion in man.[4] It is equally important to remark how the gray matter in this paradigm remains basically unscathed and functional. Here, interneuronal chains can function as a relay between the supraspinal input and the lower motor circuitry, given proper active training and provision of sensory cues in order to promote plasticity. Interneurons may act as central pattern generator for movement in man, and treatment strategies that promote their sprouting and reconnection of interneurons have great potential in promoting functional recovery.[17] One way to achieve this is by electrical stimulation: Electrical stimulation is known to promote plasticity and regeneration in patients (e.g., 20 Hz continuous stimulation.[8,14] In GEMINI, this would be achieved by installing an epidural spinal cord stimulating (SCS) apparatus, a commonly employed, safe way to treat neurological conditions. Parenthetically, these interneuronal chains can be set into operation by nonpatterned stimulation delivered via intact segmental input pathways: SCS has proved effective in this regard too in humans.[23] Another attractive way to supply electrical stimulation is by oscillating field stimulation.[27] Interestingly, electricity can be exploited to achieve axonal fusion (electrofusion): This method is at the moment not a suitable alternative for GEMINI, but it should be explored in this context.[11]
POSSIBLE PROCEDURAL SCENARIO OF HEAVEN SURGERY
What follows is a possible scenario in order to give the reader a feel for the whole endeavor.
Donor is a brain dead patient, matched for height and build, immunotype and screened for absence of active systemic and brain disorders. If timing allows, an autotransfusion protocol with D's blood can be enacted for reinfusion after anastomosis.
The procedure is conducted in a specially designed operating suite that would be large enough to accommodate equipment for two surgeries conducted simultaneously by two separate surgical teams.
The anesthesiological management and preparation is outlined elsewhere.[34] Both R and D are intubated and ventilated through a tracheotomy. Heads are locked in rigid pin fixation. Leads for electrocardiography (ECG), EEG (e.g., Neurotrac), transcranial measurement of oxygen saturation and external defibrillation pads are placed. Temperature probes are positioned in tympanum, nasopharynx, bladder, and rectum. A radial artery cannula is inserted for hemodynamic monitoring. R's head, neck, and one groin are prepped and draped if ACHP is elected. A 25G temperature probe may be positioned into R's brain (deep in the white matter), but, as highlighted, a TM thermistor should do.
Antibiotic coverage is provided throughout the procedure and thereafter as needed.
Before PH, barbiturate or propofol loading is carried out in R to obtain burst suppression pattern. Once cooling begins, the infusion is kept constant. On arrest, the infusion is discontinued in R, and started in D. An infusion of lidocaine is also started, given the neuroprotective potential.[9] Organ explantation in R is possible by a third surgical team.
R's head is subjected to PH (ca 10°C), while D's body will only receive spinal hypothermia; this does not alter body temperature. This also avoids any ischemic damage to D's major organs. R lies supine during induction of PH, then is placed in the standard neurosurgical sitting position, whereas D is kept upright throughout. The sitting position facilitates the surgical maneuvers of the two surgical teams. In particular, a custom-made turning stand acting as a crane is used for shifting R's head onto D's neck. R's head, previously fixed in a Mayfield three-pin fixation ring, will literally hang from the stand during transference, joined by long Velcro straps. The suspending apparatus will allow surgeons to reconnect the head in comfort.
The two teams, working in concert, would make deep incisions around each patient's neck, carefully separating all the anatomical structures (at C5/6 level forward below the cricoid) to expose the carotid and vertebral arteries, jugular veins and spine. All muscles in both R and D would be color-coded with markers to facilitate later linkage. Besides the axial incisions, three other cuts are envisioned, both for later spinal stabilization and access to the carotids, trachea and esophagus (R's thyroid gland is left in situ): Two along the anterior margin of the sternocleidomastoids plus one standard midline cervical incision.
Under the operating microscope, the cords in both subjects are clean-cut simultaneously as the last step before separation. Some slack must be allowed for, thus allowing further severance in order to fashion a strain-free fusion and side-step the natural retraction of the two segments away from the transection plane. White matter is particularly resistant to many of the factors associated with secondary injury processes in the central nervous system (CNS) such as oxygen and glucose deprivation and this is a safeguard to local manipulation.
Once R's head is separated, it is transferred onto D's body to the tubes that would connect it to D's circulation, whose head had been removed. The two cord stumps are accosted, length-adjusted and fused within 1-2 minutes: The proximal and distal cord segments must not be accosted too tightly to avoid further damage and not too loose to stop fusion. A chitosan-PEG glue, as described, will effect the fusion. Simultaneously, PEG or a derivative is infused into D's blood-stream over 15’-30’. A few loose sutures are applied around the joined cord, threading the arachnoid, in order to reinforce the link. A second IV injection of PEG or derivative may be administered within 4-6 hours of the initial injection.
The bony separation can be achieved transsomatically (i.e., C5 or C6 bodies are cut in two) or through the intervertebral spaces. In both R and D, after appropriate laminectomies, a durotomy, both on the axial and posterior sagittal planes, would follow, exposing the cords. In D, the cord only has been previously cooled. If need be, pressure in D is maintained with volume expansion and appropriate drugs.
The vascular anastomosis for the cephalosomatic preparation is easily accomplished by employing bicarotid-carotid and bijugular-jugular silastic loop cannulae. Subsequently, the vessel tubes would be removed one by one, and the surgeons would sew the arteries and veins of the transplanted head together with those of the new body. Importantly, during head transference, the main vessels are tip-clamped to avoid air embolism and a later no-reflow phenomenon in small vessels. Upon linkage, D's flow will immediately start to rewarm R's head. The previously exposed vertebral arteries will also be reconstructed.
The dura is sewn in a watertight fashion. Stabilization would follow the principles employed for teardrop fractures, anterior followed by posterior stabilization with a mix of wires/cables, lateral mass screws and rods, clamps and so forth, depending on cadaveric rehearsals.
Trachea, esophagus, the vagi, and the phrenic nerves are reconnected, these latter with a similar approach to the cord. All muscles are joined appropriately using the markers. The skin is sewn by plastic surgeons for maximal cosmetic results.
R is then brought to the intensive care unit (ICU) where he/she will be kept sedated for 3 days, with a cervical collar in place. Appropriate physiotherapy will be instituted during follow-up until maximal recovery is achieved.
COROLLARY CONSIDERATIONS
A possibility that must be considered is the onset of cord Central Pain (CP)), following transection of the spinothalamic tract (STT). While fusion of the STT tract is also expected, a suboptimal fusion might trigger the pain in susceptible individuals. The genesis of CP has been elucidated and a cure is available.[10]
After transplant, body image and identity issues will need to be addressed, as the patient gets used to seeing and using the new body. The patient's perception of the allotransplant should continuously be readdressed by the psychiatrists to ensure that positive, but realistic expectations are maintained. The key indicators for success are the patient's ability to form alliances with his or her health care team, intellectual and emotional development, and body image, and whether he or she has untreated or ongoing posttraumatic stress disorder. Further psychiatric assessment and treatment may be needed based on individual results to prevent an adverse postoperative emotional reaction and to ensure that the stress or anxiety related to the procedure, recovery, and new body is addressed and kept to a minimum.[18,19]
Immunosuppression is induced by a specific medication regimen and is monitored by the transplant physician and transplant coordinator. Posttransplant blood samples need to be drawn at regular intervals to screen for the development of antidonor antibodies. Ideally, serum is drawn concurrent with obtaining tissue biopsies to facilitate correlation of histology with systemic markers of immunologic activation. Biopsies should be performed regularly for suspected rejection or infection.
CONDITIONS QUALIFYING FOR HEAVEN
Several conditions would qualify for HEAVEN surgery. White[29] pointed to tetraplegics, who show a tendency to multi-organ failure. In truth, the impeller of White's study was a possible cure for intractable cancer without brain metastases. I believe that the first patient should be someone, probably young, suffering from a condition leaving the brain and mind intact while devastating the body, for instance, but by no means exclusively, progressive muscular dystrophies or even several genetic and metabolic disorders of youth. These are a source of huge suffering, with no cure at hand.
CONCLUSION
HEAVEN appears to have grown into a feasible enterprise early in the 21st century, as anticipated by White.
Extensive preparation for the surgery will be necessary. The teams will have to refine the approach details on cadaveric specimens and the surgery will have to be reenacted several times in order to coordinate the surgical and anesthesiological teams. GEMINI will also need to be confirmed with preliminary primate experimentation, or, ideally in brain dead patients before organ explantation.
On the whole, in the face of clear commitment, HEAVEN could bear fruit within a couple of years.
I have not addressed the ethical aspects of HEAVEN. In Thomas Mann's “The Transposed Heads,” two friends, the intellectual Shridaman and the earthy Nanda, behead themselves. Magically, their severed heads are restored – but to the wrong body, and Shridaman's wife, Sita, is unable to decide which combination represents her real husband. The story is further complicated by the fact that Sita happens to be in love with both men. This short story highlights the ethical dilemma that must be faced: The HEAVEN created “chimera” would carry the mind of the recipient but, should he or she reproduce, the offspring would carry the genetic inheritance of the donor.
However, it is equally clear that horrible conditions without a hint of hope of improvement cannot be relegated to the dark corner of medicine. This paper lays out the groundwork for the first successful human head transplant.
ACKNOWLEDGMENTS
The author wish to express his gratitude to the two unknown referees for their warm support and suggestions.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2013/4/2/335/113444
Disclaimer: The authors of this article have no conflicts of interest to disclose, and have adhered to SNI's policies regarding human/animal rights, and informed consent. Advertisers in SNI did not ask for, nor did they receive access to this article prior to publication
REFERENCES
- 1.Albin MS, White RJ, Locke GE, Kretchmer HE. Spinal cord hypothermia by localized perfusion cooling. Nature. 1966;210:1059–60. doi: 10.1038/2101059a0. [DOI] [PubMed] [Google Scholar]
- 2.Alzaga AG, Cerdan M, Varon J. Therapeutic hypothermia. Resuscitation. 2006;70:369–80. doi: 10.1016/j.resuscitation.2006.01.017. [DOI] [PubMed] [Google Scholar]
- 3.Amoozgar Z, Rickett T, Park J, Tuchek C, Shi R, Yeo Y. Semi-interpenetrating network of polyethylene glycol and photocrosslinkable chitosan as an in-situ-forming nerve adhesive. Acta Biomaterialia. 2012;8:1849–58. doi: 10.1016/j.actbio.2012.01.022. [DOI] [PubMed] [Google Scholar]
- 4.Basso DM. Neuroanatomical substrates of functional recovery after experimental spinal cord injury: Implications of basic science research for human spinal cord injury. Phys Ther. 2000;80:808–17. [PubMed] [Google Scholar]
- 5.Bittner GD, Ballinger ML, Raymond MA. Reconnection of severed nerve axons with polyethylene glycol. Brain Res. 1986;367:351–5. doi: 10.1016/0006-8993(86)91617-3. [DOI] [PubMed] [Google Scholar]
- 6.Bittner GD, Keating CP, Kane JR, Britt JM, Spaeth CS, Fan JD, et al. Rapid, effective, and long-lasting behavioral recovery produced by microsutures, methylene blue, and polyethylene glycol after completely cutting rat sciatic nerves. J Neurosci Res. 2012;90:967–80. doi: 10.1002/jnr.23023. [DOI] [PubMed] [Google Scholar]
- 7.Borgens RB. Cellular engineering: Molecular repair of membranes to rescue cells of the damaged nervous system. Neurosurgery. 2001;49:370–8. doi: 10.1097/00006123-200108000-00021. [DOI] [PubMed] [Google Scholar]
- 8.Canavero S. Total eye transplantation for the blind: A challenge for the future. Med Hypotheses. 1992;39:201–11. doi: 10.1016/0306-9877(92)90111-o. [DOI] [PubMed] [Google Scholar]
- 9.Canavero S, Bonicalzi V, Narcisi P. Safety of magnesium-lidocaine combination for severe head injury: The Turin LidoMag pilot study. Surg Neurol. 2003;60:165–9. doi: 10.1016/s0090-3019(03)00159-9. [DOI] [PubMed] [Google Scholar]
- 10.Canavero S, Bonicalzi V. 2nd ed. Cambridge: Cambridge University Press; 2011. Central Pain Syndrome. [Google Scholar]
- 11.Chang WC, Hawkes E, Keller CG, Sretavan DW. Axon repair: Surgical application at a subcellular scale. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2010;2:151–61. doi: 10.1002/wnan.76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cho Y, Borgens RB. Polymer and nano-technology applications for repair and reconstruction of the central nervous system. Exp Neurol. 2012;233:126–44. doi: 10.1016/j.expneurol.2011.09.028. [DOI] [PubMed] [Google Scholar]
- 13.De Georgia M, Deogaonkar A, Merrill TL. Methods to induce hypothermia. In: Mayer SA, Sessler DI, editors. Therapeutic hypothermia. New York: Marcel Dekker; 2005. pp. 293–322. [Google Scholar]
- 14.Gordon T, Sulaiman OA, Ladak A. Electrical stimulation for improving nerve regeneration: Where do we stand? Int Rev Neurobiol. 2009;87:433–44. doi: 10.1016/S0074-7742(09)87024-4. [DOI] [PubMed] [Google Scholar]
- 15.Harris BA, Andrews PJ. Direct brain cooling. In: Mayer SA, Sessler DI, editors. Therapeutic hypothermia. New York: Marcel Dekker; 2005. pp. 323–86. [Google Scholar]
- 16.Hindman BJ. Hypothermia in neurological and cardiac anethesia. In: Mayer SA, Sessler DI, editors. Therapeutic hypothermia. New York: Marcel Dekker; 2005. pp. 525–606. [Google Scholar]
- 17.Illis LS. Central nervous system regeneration does not occur. Spinal Cord. 2012;50:259–63. doi: 10.1038/sc.2011.132. [DOI] [PubMed] [Google Scholar]
- 18.Klapheke M. The role of the psychiatrist in organ transplantation. Bull Menninger Clin. 1999;63:13–39. [PubMed] [Google Scholar]
- 19.Klapheke M. Transplantation of the human hand: Psychiatric considerations. Bull Menninger Clin. 1999;63:159–73. [Google Scholar]
- 20.Koob AO, Duerstock BS, Babbs CF, Sun Y, Borgens RB. Intravenous polyethylene glycol inhibits the loss of cerebral cells after brain injury. J Neurotrauma. 2005;22:1092–111. doi: 10.1089/neu.2005.22.1092. [DOI] [PubMed] [Google Scholar]
- 21.Lee J, Lentz BR. Outer leaflet-packing defects promote poly(ethylene glycol)-mediated fusion of large unilamellar vesicles. Biochemistry. 1997;36:421–31. doi: 10.1021/bi9622332. [DOI] [PubMed] [Google Scholar]
- 22.Mack WJ, Ducruet AF, Angevine PD, Komotar RJ, Shrebnick DB, Edwards NM, et al. Deep hypothermic circulatory arrest for complex cerebral aneurysms: Lessons learned. Neurosurgery. 2007;60:815–27. doi: 10.1227/01.NEU.0000255452.20602.C9. [DOI] [PubMed] [Google Scholar]
- 23.Minassian K, Hofstoetter U, Tansey K, Mayr W. Neuromodulation of lower limb motor control in restorative neurology. Clin Neurol Neurosurg. 2012;114:489–97. doi: 10.1016/j.clineuro.2012.03.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Negrin J Jr. Spinal cord hypothermia in the neurosurgical management of the acute and chronic post-traumatic paraplegic patient. Paraplegia. 1973;10:336–43. doi: 10.1038/sc.1973.58. [DOI] [PubMed] [Google Scholar]
- 25.Shi Y, Kim S, Huff TB, Borgens RB, Park K, Shi R, et al. Effective repair of traumatically injured spinal cord by nanoscale block copolymer micelles. Nat Nanotechnol. 2010;5:80–7. doi: 10.1038/nnano.2009.303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Shimizu H, Chang LH, Litt L, Zarow G, Weinstein PR. Effect of brain, body, and magnet bore temperatures on energy metabolism during global cerebral ischemia and reperfusion monitored by magnetic resonance spectroscopy in rats. Magn Reson Med. 1997;37:833–9. doi: 10.1002/mrm.1910370606. [DOI] [PubMed] [Google Scholar]
- 27.Walters BC. Oscillating field stimulation in the treatment of spinal cord injury. PM R. 2010;2(12 Suppl 2):S286–91. doi: 10.1016/j.pmrj.2010.10.014. [DOI] [PubMed] [Google Scholar]
- 28.White RJ, Wolin LR, Massopust LC, Jr, Taslitz N, Verdura J. Primate cephalic transplantation: Neurogenic separation, vascular association. Transplant Proc. 1971;3:602–4. [PubMed] [Google Scholar]
- 29.White RJ. Hypothermia preservation and transplantation of brain. Resuscitation. 1975;4:197–210. [Google Scholar]
- 30.White RJ. Head transplants. Sci Am. 1999:24–6. [Google Scholar]
- 31.White RJ. Cerebral hypothermia and circulatory arrest. Review and commentary. Mayo Clin Proc. 1978;53:450–8. [PubMed] [Google Scholar]
- 32.White RJ, Massopust LA, Jr, Wolin LR, Taslitz N, Yashon D. Profound selective cooling and ischaemia of primate brain without pump or oxygenator. Br J Surg. 1969;56:630–1. [PubMed] [Google Scholar]
- 33.Working P, Newman M, Johnson J, Cornacoff J. Safety of PEG and PEG derivatives. In: Harris JM, Zalipsky S, editors. PEG chemistry and biological applications. Washington DC: American Chemical Society; 1997. pp. 45–57. [Google Scholar]
- 34.Young WL, Lawton MT, Gupta DK, Hashimoto T. Anesthetic management of deep hypothermic circulatory arrest for cerebral aneurysm clipping. Anesthesiology. 2002;96:497–503. doi: 10.1097/00000542-200202000-00038. [DOI] [PubMed] [Google Scholar]