

Abstract
Background:
Family care burden among schizophrenia and depressive disorders has not been addressed in the research. Family burden was significantly high in patient with schizophrenia except the effect on physical health of other family member. Comparing burden in these two groups may help in the psychosocial management.
Aim:
The aim of the study was to examine family care burden in families of schizophrenia patient and compare them with patients having depressive disorders.
Materials and Methods:
One hundred family caregivers of patient with schizophrenia and 100 family caregivers of patient with depressive disorders were recruited for the study. It was cross sectional study. The patients were diagnosed as having schizophrenia (all types) and depressive disorders using International Classification of Disease-10, Classification of Mental and Behavioral Disorders, Diagnostic Criteria for Research ICD-10 DCR criteria. Pollack and Perlick scale was used to identify the key family caregivers. Patient with 2 or more than 2 years duration of illness were included in the study groups. Family burden was assessed in the both groups by using the Family Burden Interview Schedule (FBIS) of Pai and Kapur. Data was analyzed using the descriptive statistics, Chi-square test.
Results:
Caregivers of patients with schizophrenia in comparison to depressive disorder has significantly increased mean FBIS score (P<0.001). The family burden was significantly high in family caregivers of patients with the schizophrenia except the effect on physical health of other family members.
Conclusion:
To conclude caregivers of patient with schizophrenia experience high-level of burden than the caregivers of patients with the depressive disorders.
Keywords: Depressive disorders, family care burden, schizophrenia disorders
INTRODUCTION
Schizophrenia is a continuous, life time major psychiatric disorder that may affect children, adolescents and adults. Depression is episodic, recurrent in nature, characterized by low mood, decreased psychomotor activity and depressive cognitions. Caregivers play a significant role in caring people with chronic mental illness. Caring role is not an easy task and that may impact on their personal life. Individuals with schizophrenia are less likely to gain employment and to marry, which produces grater amount of burden on caregivers. As a consequence, the remaining family members need to undertake the care of the ill person. Family burden in caregiving of severe mental illness includes missed work, domestic routine disturbance, financial strain, effect on social and leisure activities, and decreased caring role to the other family member.[1,2]
Family burden care extensively studied in schizophrenia illness and reported significant burden on caregivers. This number account 90% of caregivers experiences moderate to severe burden.[3,4,5,6,7,8] Few studies reported that caregivers of depression patient experience a higher degree of burden.[9,10,11] There are no single published studies, which have compared the family burden among schizophrenia and depressive disorders. In view of lack of data, present study was undertaken with the aim of comparing burden among caregiving of schizophrenia and depressive disorder.
MATERIALS AND METHODS
The study sample included 100 patients with schizophrenia and 100 patients with depressive disorder. Purposive sampling method was used in this study. The samples were collected from the psychiatry out-patient and in-patient department. The patients fulfilling ICD-10 DCR criteria for schizophrenia and depression were included as cases. Patients within the age group of 18-45 years with 2 or more years duration of illness, who gave informed consent for the study were taken up for the study. Patients were excluded if they were found to have organic mental disorder or other co-morbid psychiatric disorder.
A semi-structured proforma was prepared for this study, which included registration number, diagnosis, age, sex, marital status, religion, educational status, occupation, duration of illness, family status, history of mental illness in the family, patient income, and domicile. Pollack and Perlick scale was used to identify key caregivers. Family Burden Interview Schedule (FBIS) includes 24 items classified into six categories viz., financial burden, and disruption of routine family activities, family leisure, family interactions, and effect on physical and mental health of others. Ratings are carried out on a three-point scale and schedule has a separate category to rate “subjective” burden. The validity and reliability of the scale was reported satisfactory. All the items were reliable, which was reported more than 0.78 by the authors of the schedule.
RESULTS
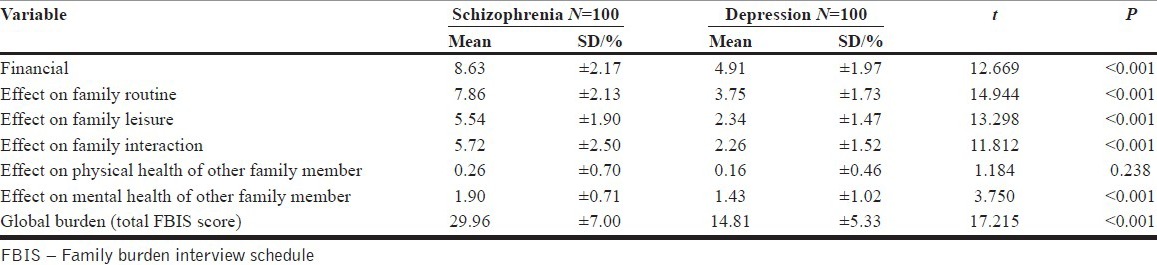
Objective burden was assessed in the both groups by using the FBIS [Table 1]. The mean score of the financial burden in patients with schizophrenia group was 8.63 and depression group had 4.91 with P<0.001. The mean scores of Effect on family routine in patients with schizophrenia group were 7.86 and depression group had 3.75 with P<0.001. The mean score of effect on family leisure in patients with schizophrenia group was 5.54 and depression group had 2.34 with P<0.001. The mean scores of effect on family interaction in patients with schizophrenia group were 5.72 and depression group had 2.26 with P<0.001. The mean score of effect on physical health of other family members in patients with schizophrenia group was 0.26 and depression group had 0.16 with P<0.238. The mean scores of effect on mental health of other family member in patients with schizophrenia group was 1.90 and depression group had 1.43 with P<0.001. The Global burden mean scores of FBIS were 29.96 and 14.81 for schizophrenia group and depression group respectively, this was also statistically significant (P<0.001) between two groups.
Table 1.
Comparison of objective burden in schizophrenia and depression
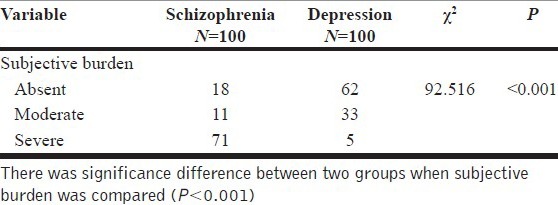
Subjective burden details among groups are described in Table 2. There was a significant difference between two groups with regard to subjective burden (P<0.001).
Table 2.
Comparison of subjective burden in schizophrenia and depression
DISCUSSION
Socio demographic details of the study group were published in the other article. The mean score of the financial burden was significantly high in patient in the schizophrenia group compared to depression. The possible differences in both groups could be the fact that schizophrenia is a continuous, chronic illness in which a patient is unable to achieve economic independence, whereas depression is an episodic illness where the amount of disability may be lesser. Schizophrenia required long-term treatment as compared to depression. Another possible reason for the difference in burden could be the fact that productivity is impaired in the schizophrenia group much more when compared to depression. It may be possible that the longer duration of illness of schizophrenia might have contributed to the increased financial burden of the key caregivers. In the present study, the majority of patients with schizophrenia were observed to be unemployed as compared to depression. Patients of schizophrenia have much more disruption in the work place due to the predominant negative, cognitive, and affective symptoms whereas patients of depression may not be having predominant negative symptoms, which may not disrupt their work. Hence, they could earn and bear treatment expenditure. Moreover, loss of employment in patients with schizophrenia still contributes to a greater financial burden on caregivers. The loss would be both direct and indirect costs that significantly contribute to the financial burden of family members. Many people with schizophrenia get into paid employment with great difficult, but they find difficult in holding jobs consequently caregivers may need to carry a large amount of the financial burden.
The mean of effect on family routine in schizophrenia disorder group was significantly high compared to the depressive group. An analysis of the difference in total mean score for effect on family leisure activities revealed that burden was significantly high among schizophrenia group compared to depressive group. The reason for differences may be schizophrenic behavior could deter family routine, and leisure activities. The nature and severity psychotic symptoms may cause social withdrawal like less interaction, lack of conversation, and few leisure interests in family members. Schene et al.[12] reported that caregivers avoid their social and leisure activities, to make reciprocity balance in role. Caregiver of schizophrenia group not only hesitant or restrict to social contact as a result of symptoms but also because of the guilt, stigma, and discrimination. Hence, it appears this population group requires more practical support from the social network whereas in case of depression the discrete nature of the episodes make patients return back to their premorbid level of functioning. It is worthwhile to note here that the caregivers of schizophrenia patient spent more time looking after their patients compared to depression. Genduso and Haley[13] asserted that schizophrenia is an early onset illness and the one who is affected may be from a younger age group and subsequently may not able to work for themselves. As an impact caregivers are forced to cut down their work hours to provide care for their patient. Another study carried out by Awad and Voruganti[14] reported that family members who leave their jobs to provide care for their ill relative with schizophrenia ranged from 1.2% for the first episode and 2.5% for long-term patients. The present study findings are consistent with these previous studies. The fear of leaving a schizophrenic patient alone makes the caregivers reside at home most of the time and consequently themselves isolate form the social contact or the outside world.
The schizophrenia group had significantly high impairment in family interaction than depressive group. Disruption of family interaction was another significant variable of family burden. Due to symptoms of schizophrenia caregivers become tense and irritable as a consequence of which ambivalence may arise in the family system regarding caring of the ill person. Schizophrenia, which is a continuous relapsing disorder, family member requires somewhat different sort of adaptive skills. Relapsing disorder would need the role reallocation in the family system where as the episodic depressive disorder may be flexible and permit caregiving arrangements. For depressive illness, there are relatively lesser strains as the caregivers may divide the energy in caring for the ill. In a patient with schizophrenia, the amount of readjustment in the family system, roles, problem solving might be different and caregivers require more rapid mobilization of crisis, and treatment management. Nevertheless, the family interaction with the schizophrenia patient and the impact of the disorder on the family member remain substantial. The symptoms of schizophrenia may be unpredictable, even frightening at times which disrupt the family dynamics. In schizophrenia negative symptoms of apathy, amotivation, asociality often disrupt the family interaction. It is more when a patient falls prey to poor sanitation, excessive smoking, and reversal of sleep. Such a sleeping habit may affect the family members’ need for rest and family system. Due to the illness the family may feel rejected by the extended family members, and this is often mixed with a feeling of anger, guilt, and hopelessness. Our clinical observation states that most family members use denial defense mechanism about their ill relatives’ illness. This also tends to add on burden.
There was no significant difference of effect on physical health of other family members between two groups. Examination of differences on psychological health revealed that there was a significant difference among two groups with more psychological problem among caregivers of schizophrenia group. The reason for the greater psychological burden among caregivers of schizophrenia group could be the continuous, chronic nature of the illness, which could precipitate a feeling of isolation, anxiety, depression, and frustration in the caregiver in contrast to discrete episodic nature of depressive disorder. Moreover, chronic illness with the loss of insight would significantly enhance the extent of psychological burden of caregivers. With the paucity of residential care, the majority of schizophrenia patients live with their relatives and providing care for a lifetime which may later lead to psychological distress among caregivers. Boye et al.[15] reported that anxiety depressive behaviors are high in caregivers of chronic illness. The other reason could be relapsing chronic illness manifest more psychological discrepancy in caregivers. Thornicroft[16] has suggested that in the west people somewhat more flexible and open, expressing enduring greater tolerance toward mentally ill people, but negative attitudes were still predominately evident. Even more Reid et al.[17] found negative emotions regarding schizophrenia illness are markedly consistent over the course of illness and across different places. One possible reason for the difference could be the fact that coping strategies of caregivers in depressive disorder are found better possible reason could be the nature of illness.
Examination of differences on subjective burden revealed that there was a significant difference among two groups with more subjective burden in caregivers of schizophrenia group. Subjective burden delineates the personal distress or pain as a result of illness, which are psychological reactions, which caregivers undergo. These include grieving for the ill, feelings of loss, and loss of the person who might have been. The family members of schizophrenia group experience tremendous psychological stress with regard to caring of the ill person, which may precipitate subjective burden. These family members experiences considerable grief about not enough has been carried out for the ill and may feel that they are the cause or contributed for the patient illness.
The mean (FBIS) global burden score in relative of schizophrenia group was significantly higher compared to depression group. The study carried out by Nehra et al.[18] reported that both groups bipolar affective disorder and schizophrenia were similar in the areas of coping and care giving experiences.
Some interesting findings emerged out of this study. It was clearly seen that the extent and pattern of family care burden among families of schizophrenia patient is more than that among depressive disorder. The present study has implications for practice, administration, education, and research. The exploration of burden of family caregivers gives baseline data necessary for decisions taking, further research and generation of coping styles, and tools to promote rehabilitative caring. Psychosocial intervention program has to be planned on the bases of proper assessment by caregivers coping styles, communication skills and community resources of key caregivers.
CONCLUSION
The present study has shown that family members of patients with schizophrenia experienced considerable high degree of family burden compared to depressive disorder group. This has an important implication for management of patient with the schizophrenia.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Kreisman DE, Joy VD. Family response to the mental illness of a relative: A review of the literature. Schizophr Bull. 1974;1:34–57. doi: 10.1093/schbul/1.10.34. [DOI] [PubMed] [Google Scholar]
- 2.Hatfield AB. Coping and adaptation: A conceptual framework for understanding families. In: Hatfield AB, Lefely HP, editors. Families of the Mentally Ill. New York: Guilford; 1997. pp. 60–84. [Google Scholar]
- 3.Magliano L, Fiorillo A, De Rosa C, Malangone C, Maj M National mental health project working group. Family burden in long-term diseases: A comparative study in schizophrenia vs. physical disorders. Soc Sci Med. 2005;61:313–22. doi: 10.1016/j.socscimed.2004.11.064. [DOI] [PubMed] [Google Scholar]
- 4.Provencher HL. Objective burden among primary caregivers of persons with chronic schizophrenia. J Psychiatr Ment Health Nurs. 1996;3:181–7. doi: 10.1111/j.1365-2850.1996.tb00085.x. [DOI] [PubMed] [Google Scholar]
- 5.Gautam S, Nijhawan M. Burden on families of schizophernic and chronic lung disease patients. Indian J Psychiatry. 1984;26:156–9. [PMC free article] [PubMed] [Google Scholar]
- 6.Bury L, Zaborowski B, Konieczyńska Z, Jarema M, Cikowska G, Kunicka A, et al. Family burden of schizophrenic patients with various forms of psychiatric care. Psychiatr Pol. 1998;32:275–85. [PubMed] [Google Scholar]
- 7.Jenkins JH, Schumacher JG. Family burden of schizophrenia and depressive illness. Specifying the effects of ethnicity, gender and social ecology. Br J Psychiatry. 1999;174:31–8. doi: 10.1192/bjp.174.1.31. [DOI] [PubMed] [Google Scholar]
- 8.Mors O, Sørensen LV, Therkildsen ML. Distress in the relatives of psychiatric patients admitted for the first time. Acta Psychiatr Scand. 1992;85:337–44. doi: 10.1111/j.1600-0447.1992.tb10315.x. [DOI] [PubMed] [Google Scholar]
- 9.Perlick DA, Rosenheck RA, Miklowitz DJ, Chessick C, Wolff N, Kaczynski R, et al. Prevalence and correlates of burden among caregivers of patients with bipolar disorder enrolled in the systematic treatment enhancement program for bipolar disorder. Bipolar Disord. 2007;9:262–73. doi: 10.1111/j.1399-5618.2007.00365.x. [DOI] [PubMed] [Google Scholar]
- 10.Carpentier N. Comparison of the extent and pattern of family burden in depressive disorders. Indian J Psychiatry. 2005;37:105–12. [PMC free article] [PubMed] [Google Scholar]
- 11.Jacob M, Frank E, Kupfer DJ, Carpenter LL. Recurrent depression: An assessment of family burden and family attitudes. J Clin Psychiatry. 1987;48:395–400. [PubMed] [Google Scholar]
- 12.Schene AH, van Wijngaarden B, Koeter MW. Family caregiving in schizophrenia: Domains and distress. Schizophr Bull. 1998;24:609–18. doi: 10.1093/oxfordjournals.schbul.a033352. [DOI] [PubMed] [Google Scholar]
- 13.Genduso LA, Haley JC. Cost of illness studies for schizophrenia: Components, benefits, results, and implications. Am J Manag Care. 1997;3:873–7. [PubMed] [Google Scholar]
- 14.Awad AG, Voruganti LN. The burden of schizophrenia on caregivers: A review. Pharmacoeconomics. 2008;26:149–62. doi: 10.2165/00019053-200826020-00005. [DOI] [PubMed] [Google Scholar]
- 15.Boye B, Bentsen H, Ulstein I, Notland TH, Lersbryggen A, Lingjaerde O, et al. Relatives’ distress and patients’ symptoms and behaviours: A prospective study of patients with schizophrenia and their relatives. Acta Psychiatr Scand. 2001;104:42–50. doi: 10.1034/j.1600-0447.2001.00190.x. [DOI] [PubMed] [Google Scholar]
- 16.Thornicroft G. From stigma to ignorance prejudice and discrimination. In: Thornicroft G, editor. Shunned: Discrimination against People with Mental Illness. New York: Oxford University press; 2006. pp. 170–203. [Google Scholar]
- 17.Reid J, Lloyd C, De Groot L. The psychoeducation needs of parents who have an adult son or daughter with a mental illness. [Accessed 12th November 2012];Aust E J Adv Ment Health. 2005 4:1–13. Available from: http://www.auseinet.com/journal/vol4iss2/reid.pdf . [Google Scholar]
- 18.Nehra R, Chakrabarti S, Kulhara P, Sharma R. Caregiver-coping in bipolar disorder and schizophrenia: A re-examination. Soc Psychiatry Psychiatr Epidemiol. 2005;40:329–36. doi: 10.1007/s00127-005-0884-3. [DOI] [PubMed] [Google Scholar]