

Abstract
Background:
Currently, in developing countries, there is a paradigm shift in the mortality patterns from communicable to non-communicable diseases.
Objective:
This study is aimed at providing a broad spectrum on the mortality patterns in elderly within a 5-year-period in a tertiary healthcare provider in Nigeria.
Materials and Methods:
This study is a retrospective review of mortality patterns of elderly patients from January 2007 to December 2011 occurring in Irrua specialist teaching hospital, (ISTH), Irrua and its environs. Information derived from the request cards include age, sex, clinical history, diagnosis, duration and cause of death.
Results:
During this period a total of 3,002 elderly (>65 years) admissions were seen. Of this, 561 patients were confirmed dead. Among this, 317 and 244 cases were elderly male and female patients, respectively. Hence the ratio of male to female was 1.3:1.0. The peak age group was 65-70 years accounting for 147 patients (26.2%). The age range of patients was 65-104 years while the modal and mean ages were 69 years and 74 years 4.2 standard deviation (SD), respectively. The most commonly encountered cause of mortality was cerebrovascular accident constituting 141 (25.1%) cases. The 2nd and 3rd majority of mortality cases were malignancies and diabetes mellitus (metabolic disorder) accounting for 85 (15.2%) and 45 (8%) cases, respectively. Others include congestive cardiac failure 35 (6.2%), Septicaemia 29 (5.2%), trauma 26 (4.6%) while chronic renal failure and chronic obstructive pulmonary disease consist of 22 cases (3.9%) each.
Conclusion:
Non-communicable diseases particularly cerebrovascular diseases and malignancies were the most commonly encountered cause of elderly mortality in our environment. Notwithstanding a large percentage of mortality patterns also results from communicable diseases with sepsis as the leading cause of mortality.
Keywords: Cerebrovascular accident, malignancy, mortality, sepsis
INTRODUCTION
Generally, there is scarcity of information in disease prevalence, mortality rates and patterns in developing countries including Nigeria and our geo-ethnical locality. This is contrary to what obtains in the developed countries where such data abounds. However, the few reports available are hospital-based and may not adequately form a comprehensive national data of disease patterns as recommended by the World Health Organization (W.H.O.), but definitely could serve in assessing the patterns of diseases, and its mortality and morbidity when monitored over a prolong period.1 The significance of this study is remarkable in the objectives of the W.H.O. in healthcare delivery and the achievement of the millennium development goals in Nigeria.2 Information derived from this surveillance patterns is significant to improvement of health services in Nigeria and hence reducing patterns of morbidity and mortality among patients in developing countries.
Studies have shown that in the past, communicable diseases constituted a huge source of mortality and morbidity in Africa as compared to western countries were non-communicable disease predominates.3 However currently there is a paradigm shift from communicable to non-communicable diseases in Africa.4 Reports have it that the disease patterns and mortality rates from cerebrovascular accidents, cardiovascular diseases, Diabetes and renal diseases is on the increase in Africa.5
The objective of this study is mainly to provide a broad report on the diseases prevalence patterns and disease mortality in elderly within a 5-year-period in a tertiary healthcare provider in Irrua, Nigeria. Again, this is to highlight the emerging non-communicable diseases in the elderly in our locality.
MATERIALS AND METHODS
Study setting and design
This study is a mortality review of 561 elderly patients (>65 years) as seen in the accident/emergency unit and medical/surgical wards of Irrua specialist teaching hospital, Irrua. This data was obtained from the medical records department and post mortem records of the pathology departments over a five years period from January 2007 to December 2011.
Demographic information derived from the request cards includes age, sex, clinical history, clinical diagnosis and duration and cause of death. The causes of death were broadly classified into non-communicable and communicable patterns. Again, non-communicable causes were further sub-classified into cardiovascular, malignancy, renal, burns, haematological, nutritional, and metabolic including diabetes mellitus and others (pyrexia of unknown origin, hypersensitivity reaction, snake bites, tetanus, ophthalmological disorders, psychiatric disorders and parasitic infections).
Data management
Data obtained were coded and analysed using the Statistical Packaging for Social Sciences (SPSS) version 17.
RESULTS
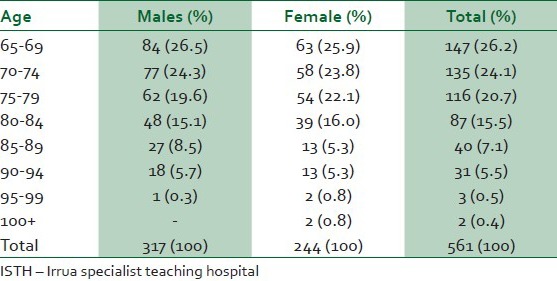
A total of 3,002 elderly (>65 years) patients were admitted in Irrua specialist teaching hospital during this 5-year-period. Of these, 561 patients were certified dead accounting for 18.7%. Out of these, 317 cases were elderly male patients and 244 were elderly female patients. Hence the ratio of male to female was 1.3:1.0. Among all, the disease mortality peak age group was 65-70 years accounting for 147 patients (26.2%). This is closely followed by 70-74 years constituting 135 (24.1%) cases. Only two cases constituting 0.4% occurred above 100 years and were seen in females. Other age of occurrence of disease mortality are shown in Table 1. The age range of patients was 65 to 104 years while the modal and mean ages were 69 years and 74 ± 4.2 years, respectively.
Table 1.
Age and sex distribution of mortality pattern in elderly patients of ISTH (2007-2011)
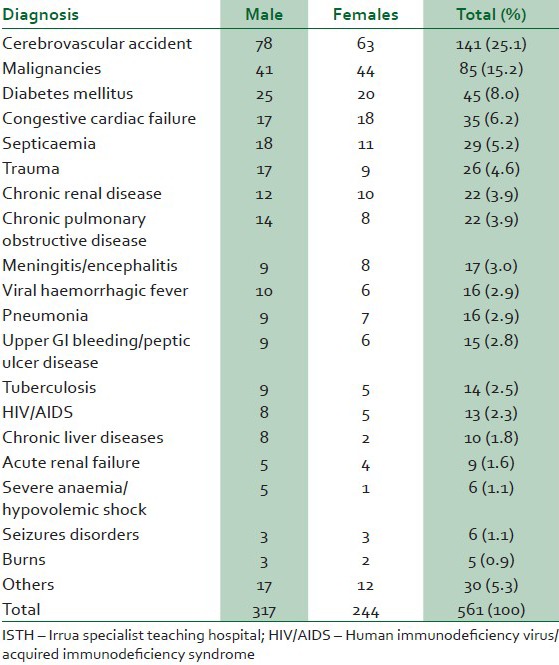
The pattern of diseases responsible for mortality in elderly age groups as seen in Table 2 is formatted in descending order of occurrence. Among these, the most commonly encountered includes cerebrovascular accident in both male and female elderly patients constituting a total of 141 (25.1%) cases. The second majority of mortality cases was malignancies occurring a distance second and accounting for 85 (15.2%) of all cases. The 3rd majority was diabetes mellitus (metabolic disorder) accounting for 45 (8%) cases. Others in that order includes congestive cardiac failure 35 (6.2%), Septicaemia 29 (5.2%), trauma 26 (4.6%), chronic renal failure and chronic obstructive pulmonary diseases constituted 22 (3.9%) each, meningitis/encephalitis 17 (3%), viral haemorrhagic fever and pneumonia accounted for 16 (2.9%) each, upper gastrointestinal bleeding/peptic ulcer diseases 15 (2.8%) while tuberculosis and human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) accounted for 14 (2.5%) and 13 (2.3%), respectively. Table 2 contains the rest of the list. All the cases classified as others were extremely rare these include tetanus, parasitic infections, psychiatric disorders, ophthalmological disorders and pyrexia of unknown origin.
Table 2.
Mortality patterns of diseases among elderly patients in ISTH (2007-2011)
DISCUSSION
Despite the fact that this study of mortality patterns of elderly patients is a hospital based study, its significance cannot be overemphasised as it show the patterns of death in our geographic and ethnic location served by this hospital. However, since there are no comprehensive national data on death patterns in this country, this may represent significantly part of the national health statistics if this is well extrapolated.
In this study, the mortality patterns of non communicable diseases in elderly were far more common than communicable diseases. This is similar to previous studies done by Ansa et al., where mortality from non-communicable diseases was far more common than communicable diseases pattern.5 Again, this study is in tandem with reports of other researchers.6,7,8 However, this is different from the report of Adeolu et al.,1 where communicable disease particularly infectious disease was the most common cause of death. The different in this variation may partly due to sample size and the age bracket of occurrence of infectious diseases occurring in younger age groups, particularly infants and childhood diseases. More so, significant number of young adult and middle age die from high prevalence of HIV/AIDS which are rarely seen in elderly patients. Our study confirms the emergence of non-communicable diseases in our locale, Nigeria in particular and developing countries in general. The reason being partly due to the fact that age is a major risk factor to most of the non-communicable diseases as this study was conducted in elderly patients. Again, lifestyle, western diet and obesity have contributed to the increase prevalence of non-communicable diseases, especially cardiovascular diseases. In this study, cerebrovascular accident was the most commonly encountered cause of death among admitted elderly patients. This is further supported by other researchers where it was adjudged as the most common cause of morbidity and mortality in medical admissions.5,6,7,8 Furthermore, other non-communicable diseases including diabetes mellitus, congestive cardiac failure with cardiovascular diseases and chronic renal failure accounted for majority of mortality cases among the elderly in our environment. This, once more is similar to previous global report where cardiovascular accidents accounted for most of the mortality patterns. Recent reports also corroborate this study revealing that it accounted for higher mortality rates in developing countries.8,9 This furthermore is supported by the statistics of the WHO suggesting that by the year 2020 eight out of every 10 cases of cardiovascular disease mortality would come from developing countries while there would be a decrease in the incidence of mortality rates in developed countries.10,11 This emerging trends of non-communicable diseases morbidity and mortality patterns in developing countries is worrisome because only very few well-equipped facilities to cater for such patients are available across the country with records of population explosion.
Again various malignancies constituted the second majority mortality pattern of diseases in elderly patients; however, there is a slight preponderance of mortality patterns in women. This once more is supported by the very high rates of breast cancer and cervical cancers mortality and morbidity pattern in developing countries.12 Meanwhile, in elderly males prostate cancer is among the most common cause of morbidity and mortality in Nigeria and worldwide.13 This very high prevalence of malignancies in our locality is not surprising as age is a major risk factor to the occurrence of malignancies worldwide as most of our patients were 65 years and above. Again, this centre is the only tertiary institution in this locality servicing several towns and villages in the two of the three senatorial districts (Edo central and north) and also part of neighbouring Kogi state. Therefore, it is serving as a referral centre to most oncology cases from all secondary and primary health institutions in this locality. However, this is at variance with studies done by Okunola et al.,9 where diabetes mellitus was the 2nd most frequent morbidity and mortality patterns. The reason for this variation may partly be attributed to pattern of study as their study span across all age groups while our study was restricted to elderly patients.
Notwithstanding, it is important to note that a large percentage of elderly mortality cases comes from communicable especially infectious diseases. This is similar to several reports by different researchers.14 The reasons for this similarity may partly be attributed to poverty, overpopulation with overcrowding, poor hygiene and socio-cultural believes. On our list sepsis/septiceamia was the most common cause of mortality among the communicable diseases in elderly although it ranked 5th in the series and accounted for 5.2% of all cause death in the elderly. Similarly viral haemorrhagic fever including Lassa fever is also a very common cause of mortality in this environment. The reason for this observation is based on the fact that this locality falls within the Lassa fever belt of Nigeria. More so, it is the only referral centre tertiary institution in Edo state and neighbouring states that is fully equipped to investigate and manage Lassa fever cases.
In our study, a handful of death resulting from trauma was encountered in elderly. This supports the increase global trend in mortality patterns from cases of gunshot injuries and road traffic accidents.14,15 Studies have shown that about 1.2 million deaths resulting from auto-crash yearly were reported globally.15 Furthermore, it is estimated globally by the year 2020 that auto-crash trauma would be the 3rd leading cause of morbidity and mortality worldwide.15,16
CONCLUSION
Non-communicable diseases particularly cerebrovascular diseases and malignancies are the leading causes of elderly mortality in our environment. Diabetes mellitus and trauma were also commonly encountered causes of death in the elderly. However, a large percentage of mortality patterns also results from communicable diseases with sepsis as the leading cause while meningitis and viral haemorrhagic fever were frequently common. Hence, there is the need to advocate a holistic care for the elderly to reduce the scourge of both non-communicable and communicable disease mortality in elderly.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Adeolu AA, Arowolo OA, Alatise IO, Osasan SA, Bisiriyu LA, Omoniyi EO, et al. Pattern of death in a Nigeria Teaching Hospital; A 3-Decade analysis. Afr Health Sci. 2010;10:266–72. [PMC free article] [PubMed] [Google Scholar]
- 2.Murray CJL, Lopez AD. Progress and directions in refining the Global Burden of Disease Approach. World Health Organization discussion document. [Last accessed on 2001 Jan 10]. Available from: http://www.who.int/whosis/guides/guidemebod.htm . [DOI] [PubMed]
- 3.Ebrahim S, Smith GD. Exporting failure? Coronary heart disease and stroke in developing countries. Int J Epidemiol. 2001;30:201–5. doi: 10.1093/ije/30.2.201. [DOI] [PubMed] [Google Scholar]
- 4.Reducing risks promoting healthy life. Geneva: WHO; 2002. World Health Organization. The World Report 2002. [Google Scholar]
- 5.Ansa VO, Ekott JU, Bassey EO. Profile and outcome of cerebrovascular admission at the University of Uyo Teaching Hospital, Uyo: A five year review. Niger J Clin Pract. 2008;11:22–4. [PubMed] [Google Scholar]
- 6.Ogun SA, Adelowo OO, Familoni OB, Jaiyesimi AE, Fakoya EA. Pattern and outcome of medical admission at the Ogun State University Teaching Hospital, Sagamu: A three year review. West Afr J Med. 2000;19:304–8. [PubMed] [Google Scholar]
- 7.Odenigbo CU, Ogujiofor OC. Pattern of medical admission at the Federal Medical Centre, Asaba: A two year review. Nig J Clin Pract. 2009;12:395–7. [PubMed] [Google Scholar]
- 8.Reddy KS, Yusuf S. Emerging Epidemic of cerebro-vascular diseases in Developing Countries. Circulation. 1998;97:597–601. doi: 10.1161/01.cir.97.6.596. [DOI] [PubMed] [Google Scholar]
- 9.Okonola OO, Akintude AA, Akinwusi PO. Some emerging issues in medical admission pattern in the tropics. J Dent Med Med Sci. 2011;1:5–8. doi: 10.4103/1119-3077.94098. [DOI] [PubMed] [Google Scholar]
- 10.Onwuchekwu AC, Asekomeh EG. Geriatric admission in developing country: Experience from a tertiary centrein Nigeria. Ethn Dis. 2009;19:359–62. [PubMed] [Google Scholar]
- 11.Akinwusi PO, Okunola OO, Opadijo OG. Hypertensive herth failure in Osogbo, south western Nigeria: Clinical presentation and outcome. Nig Med Pract. 2009;56:53–6. [Google Scholar]
- 12.Bray F, Ren JS, Masuyer E, Ferlay J. Estimates of global cancer prevalence for 27 sites in adult population in 2008. Int J Cancer. 2013;132:1133–45. doi: 10.1002/ijc.27711. [DOI] [PubMed] [Google Scholar]
- 13.Forae GD, Obaseki DE, Aligbe JU, Ekanem VJ. Morphological patterns of prostatic lesions in Benin-City: A twenty year retrospective study. Ann Trop Pathol. 2011;2:23–8. [Google Scholar]
- 14.From the centre for disease control and prevention. Death resulting from firearms- and motor-vehicle-related injuries--United States, 1968-1991. JAMA. 1994;271:495–6. [PubMed] [Google Scholar]
- 15.Krug EG, Sharma GK, Lozano R. The global burden of injuries. Am J Public Health. 2000;90:523–6. doi: 10.2105/ajph.90.4.523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020.Global Burden of Disease Study. Lancet. 1997;349:1498–504. doi: 10.1016/S0140-6736(96)07492-2. [DOI] [PubMed] [Google Scholar]