

Abstract
Objectives:
To describe the epidemiology of head injuries sustained due to bicycle accidents in India.
Materials and Methods:
Data were retrospectively collected over a period of six months (15 May 2011 to 15 November 2011). Demography of patients, Glasgow coma scale (GCS), clinical and imaging findings, and mortality and outcome using Glasgow outcome scale (GOS), Rivermead post-concussion symptom questionnaire (RPCSQ) and Rivermead head injury follow-up questionnaire (RHFUQ), were analyzed. Outcome was assessed by telephonic interview.
Results:
There were 108 patients (100 males) with mean age of 27.7 years. Seventy-four (68.5%) were from rural areas. Accidents due to vehicular collision accounted for 60 (55.6%) cases. None wore a helmet. The admission GCS was 14-15 in 68.5% cases, 13-3 in 31.5%. The risk of moderate to severe injuries was increased among working laborers (OR = 5), and patients with loss of consciousness (OR = 4). Sixty-three (49%) patients had abnormal computed tomography (CT) findings; most common finding was skull fracture 25 (23.1%). Four patients needed surgery. The GOS assessment at three to six months revealed favorable outcome in 66 patients (61.1%) and death in 8 (7.4%). The common post-concussion symptoms were headache, fatigue, and poor concentration.
Conclusion:
The majority of hospitalized cyclists were from a rural background and of the lower income group. After three months the majority of patients had good recovery with few persistent concussion symptoms.
Keywords: Bicycle, glasgow outcome scale, head injury, outcome, rivermead post-concussion symptom questionnaire
Introduction
Traumatic brain injury (TBI) is a significant public health problem leading to mortality, morbidity, and socioeconomic losses in India. The majority (60%) of TBI cases are a result of road traffic accidents (RTA). Among RTA, pedestrian injuries are most common followed by two-wheelers and bicyclists.[1]
Most of the Indian population lives in rural areas and small cities. The roads of different types, widths, with varying topographic and climatic conditions, influence the travel pattern in rural and urban areas. Walking and cycling remain the dominant modes of transport in small cities and rural areas.[2,3] The pedal bicyclist constitutes a significant share of total traffic on Indian roads accounting for 15-35% of total trips.[3] The incidence of head injuries in cyclists ranges from 14-36% of the total injuries. Their demographic details, risk, cause, severity, helmet benefit, mortality rate and preventive measure studies have been well studied in developed countries.[4,5,6,7,8,9]
In our country, cycling forms a major mode of non-motorized transportation in villages and small cities, but literature on head injuries sustained in bicycle crashes is lacking. The present study aimed to explore the knowledge regarding the demographic, clinical and imaging findings, and outcome of bicycle-related injuries at our institute.
Materials and Methods
This study was done at a tertiary level referral centre for treatment of neurological, neurosurgical, and psychiatric patients. It has a separate facility for trauma cases that serves patients from neighboring districts. Patients with TBI, who have a different registration process, are evaluated by neurosurgery residents and data is entered in a structured “head injury proforma”, which consists of comprehensive demographic, clinical and computed tomography (CT) scan findings. These data are verified by a qualified neurosurgeon on duty. Data of all patients during a period from 15 May 2011 to 15 November 2011 were retrospectively reviewed. All these patients had undergone head CT scan. The CT scan findings were confirmed independently from images archived in picture archival communication system (PACS). From these records the data of all patients who sustained head injuries while riding a bicycle were identified. Their clinical records and CT images were reviewed.
The outcome assessment tools used were Glasgow outcome scale (GOS), Rivermead post-concussion symptom questionnaire (RPCSQ), and Rivermead head injury follow-up questionnaire (RHFUQ). The assessment was done at three months to six months after injury. To assess these scales we strictly followed the duration with minimum three months to maximally six months after injury because during the initial three months after head injury the majority of patients (70-80%) with mild to moderate severity manifests with concussion symptoms, but after three months these symptoms decrease to 15-20% and may be persistent for long time.[10,11] Outcome was assessed prospectively for 74 patients using telephonic interview. Thirty-four patients were not available for assessment. The exact reasons for non availability was possible change in phone numbers.
Statistical analysis
The data was analyzed using SPSS 15.0 program (SPSS, Inc., Chicago, IL, USA; Network license, serial number 5047404). Data were expressed using descriptive statistics such as mean and standard deviation for continuous variables, and frequency and percentage for categorical variables. Logistic regression was used to compare moderate to severe injury with mild injury on crash characteristics. The independent variables considered were victim's occupation, Ear, Nose and Throat bleed (ENT bleed) (present or absent), loss of consciousness (present or absent), CT findings (normal or abnormal), skull fracture (present or absent).
The significance was calculated by Chi square for categorical groups and independent t test for continuous data.
Results
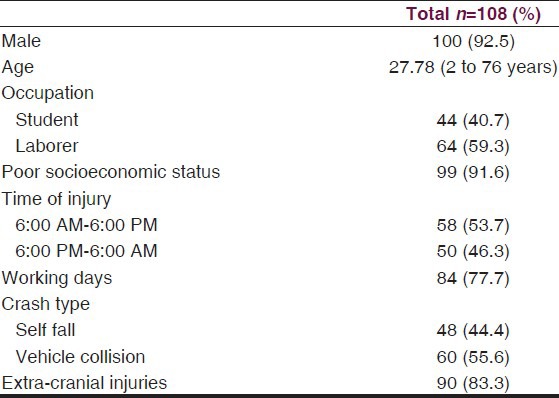
During the study period 6779 trauma patients were evaluated in emergency services. RTA accounted for 3388 (50%) cases. Among them, bicyclists accounted for 108/3388 (3.18%) cases. The demographic profile is depicted in Table 1. Most of these patients were young males, either student or laborers, from poor socioeconomic status, and sustained injuries during daytime due to collision with other vehicles. Single bicycle crash (fall) was more common among th epediatric age group. Most had extra-cranial injuries as well.
Table 1.
Demographic profile of patients
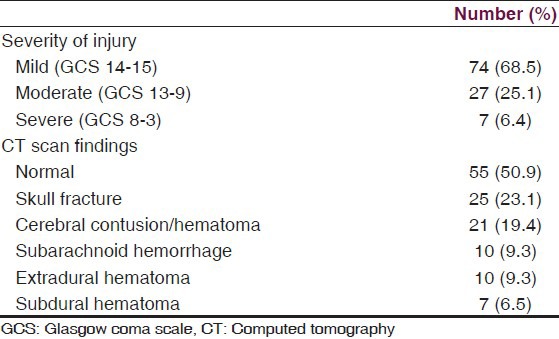
The clinical and imaging findings are given in Table 2. Most cases had mild TBI. The head CT scan was done for 98 (90.7%) cases, and was normal in nearly half. The commonest abnormality was skull fracture. Surgery was required for four (3.7%) cases.
Table 2.
Clinical and imaging findings of all 108 cases
Out of 108 patients, 74 were available for outcome assessment at mean 4.5 months after injury by telephonic interview. The outcome of these patients is given in Tables 3, 4a and 4b.
Table 3.
The follow-up details of functional outcome of 74 patients
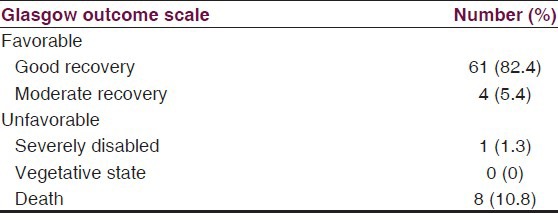
Table 4a.
Post-concussion symptoms’ follow-up details of 74 patients
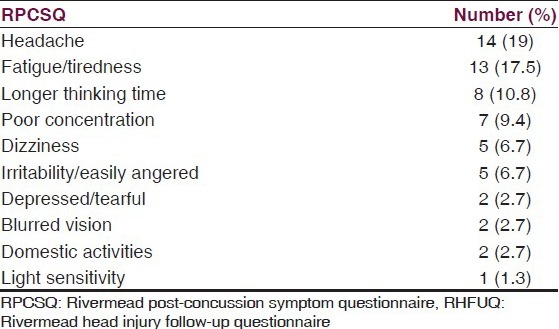
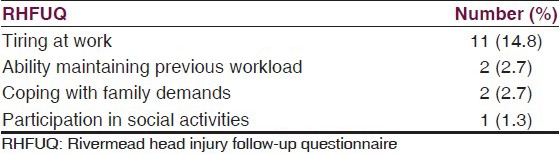
Table 4b.
Head injury follow-up details of 74 patients
Most of the survivors had a good recovery. The post-concussion symptoms were more frequent among middle-aged patients presenting with moderate TBI. Eight (7.4%) succumbed to the injuries. Except for one elderly patient, all deaths occurred in young adults. Six patients died due to vehicle collision and two patients due to fall. In five cases the mortality was attributed to severe TBI, and in three cases to extra-cranial injuries. Only one fatal case was from an urban area, the rest were from rural areas.
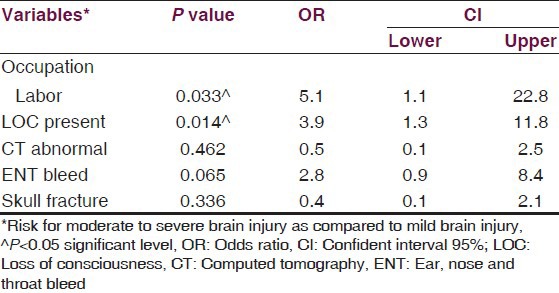
In the present study model the dependent variable, moderate and severe traumatic brain injury, was significantly affected by the occupation of the patient, and history of loss of consciousness (LOC). The analysis results showed that labor workers were more severely injured (P = 0.033) with five times more risk of sustaining moderate to severe injuries as compared to students. Patients presenting with loss of consciousness were more severely injured (P = 0.014) with four times more risk of sustaining moderate to severe injuries when compared to patients manifesting with no loss of consciousness [Table 5].
Table 5.
Logistic regression analysis for severity of injury
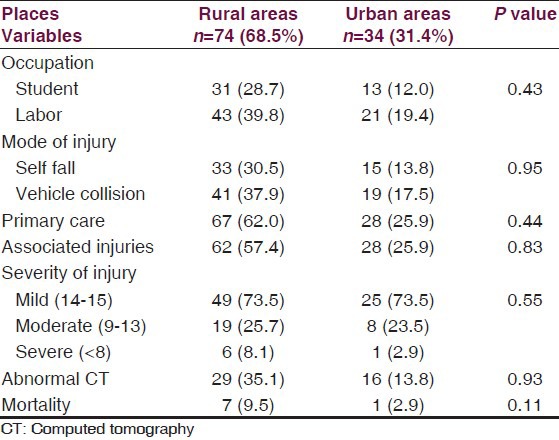
There was no significant difference between rural and urban cycle injuries as compared with patient's occupation, crash type, primary care, associated injuries, injury severity and CT findings [Table 6].
Table 6.
Comparison of characteristics of injuries in rural and urban areas
Discussion
Cycling is a healthy and economical mode of transportation. It is an easy way to get exercise that builds up muscle strength and tone, and keeps the heart healthy.[12] The expenses for using and maintaining it are minimal. It is the commonest mode of transportation among the rural population and low-income urban population in a developing country. Bicycles are commonly used by laborers and school students in India. The cyclists are vulnerable to injuries in rural areas due to bad, narrow roads, and sometimes domestic animals may either stand or sit on the roads, thereby obstructing the passage.[13] The roads in urban areas are congested and have vehicles of various speeds. There are no dedicated bicycle lanes.
In India various age groups use bicycles as a common mode of travel. The present study showed that 50% of injuries occurred in the middle age group. In the middle-aged group most were males of the labor class who sustained injuries during daytime while going to work. Studies from developed countries have described the injury patterns and possible preventive measures among preschool and school children cyclists.[8,14,15,16,17] A prospective study by Davidson et al., showed that the majority of injured cyclists were men on roads without separate lanes during daylight hours.[7] Our data also showed that bicycle collision with moving vehicles, especially motorcycles, auto-rickshaws, and cars was the commonest crash type in all age groups. Single bicycle crash (fall) was more common among the pediatric age group. The studies by Eid et al., and Hefny et al., have shown that the common cause of injury was fall from moving bicycle followed by collision with other moving vehicle.[9,18]
On logistic regression our results showed that the menial workers and patients manifesting with LOC after injury are at risk of developing moderate to severe injury. It could be that this group of workers has to use busy arterial roads where they are exposed to high-speed vehicular traffic. A study by Rivera et al., reported that the risk of serious injuries among cyclists was increased by vehicle collision, self-reported speed >15 mph, and age over 39 years.[4]
The present study data showed that eight patients (7.4%) died, all were males. Most of them died due to TBI. Six patients (5.5%) died due to vehicle collision and two patients (1.8%) due to fall. Majority of deaths 7 (6.4%) were in rural areas. Probably, village roads have unpaved paths or improper surfaces with partial concrete and craters which explains the increased accidents in rural areas as observed from our study. Also, a fall on these roads could result in head injury and/or polytrauma which could be more severe. In the literature the mortality rate among pedal cyclist ranges from 0.18-1.5%, and TBI is the leading cause of death.[6,9] More deaths are due to collision with other vehicles.[6]
Studies have reported advantages and disadvantages for using a helmet while riding a bicycle.[19] None of the patients in our study used a helmet while cycling due to lack of information and laws to enforce the rules.
Outcomes were measured after head injury that accessed improvement in functioning and quality of life, measures of activity and participation, measure of psychological and psychosocial adjustment.[20] These areas of outcome are covered in GOS, RPCSQ, and RHFUQ. The outcome was favorable in most of the patients but a significant number of cases had post-concussion symptoms like headache, giddiness, tiredness, and fatigue and decreased interactions with others, which were more frequent among middle-aged patients presenting with moderate TBI.
Limitations of the study
The duration for outcome assessment was three to six months. We could not explain the exact details of one-third of the patients who did not respond to telephonic interview for outcome assessment. We could not collect the data on modality of transport use after a TBI.
Recommendations
The study gives information about bicycle accident related head injury. The results showed that the accidents occurred on bad roads without lane road discipline. Hence the following recommendations are made.
Pre-event phase—separation of cyclists from motor vehicles by dedicated bicycle tracks.[21] Pre-event and event phase—separate signals and low speeds at intersection.[22] Event and post-event phase—wear proper bicycle helmets.[4,5,7,9] Post-event medical management and rehabilitation for persistent concussion symptoms.
Conclusion
Bicycle injuries are common among middle-aged males from a rural background due to vehicular collision. The majority had associated injuries with abnormal head CT findings. The laborers and patients presenting with loss of consciousness were at high risk of developing moderate to severe injuries. Post-traumatic concussion symptoms were more among moderately injured middle-aged patients.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Gururaj G. An epidemiological approach to prevention: Prehospital Care and rehabilitation in neurotrauma. Neurology India. 1995;43:95–105. [Google Scholar]
- 2.Gururaj G. Bangalore: Aditi Enterprises; 2011. Road safety in India: A frame work for action copyright: NIMHANS. [Google Scholar]
- 3.Mohan D. Delhi: Indian institute of technology; 2004. The Road ahead traffic injuries and fatalities in India. [Google Scholar]
- 4.Rivera FP, Thompson DC, Thompson RS. Epidemiology of bicycle injuries and risk factors for serious injury. Inj Prev. 1997;3:110–4. doi: 10.1136/ip.3.2.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Frank E, Frankel P, Mullins RJ, Taylor N. Injuries resulting from bicycle collisions. Acad Emerg Med. 1995;2:200–3. doi: 10.1111/j.1553-2712.1995.tb03198.x. [DOI] [PubMed] [Google Scholar]
- 6.Sikic M, Mikocka-Walus AA, Gabbe BJ, McDermott FT, Cameron PA. Bicycling injuries and mortality in Victoria, 2001–2006. Med J Aust. 2009;190:353–6. doi: 10.5694/j.1326-5377.2009.tb02446.x. [DOI] [PubMed] [Google Scholar]
- 7.Davidson JA. Epidemiology and outcome of bicycle injuries presenting to an emergency department in the United Kingdom. Eur J Emerg Med. 2005;12:24–9. doi: 10.1097/00063110-200502000-00007. [DOI] [PubMed] [Google Scholar]
- 8.Karkhaneh M, Naghavi M, Rowe BH, Hagel BE, Jafari N, Saunders LD. Epidemiology of bicycle injuries in 13 health divisions, Islamic Republic of Iran 2003. Accid Anal Prev. 2008;40:192–9. doi: 10.1016/j.aap.2007.05.006. [DOI] [PubMed] [Google Scholar]
- 9.Eid HO, Bashir MM, Muhammed OQ, Abu-Zidan FM. Bicycle-related injuries: A prospective study of 200 patients. Singapore Med J. 2007;48:884. [PubMed] [Google Scholar]
- 10.Podell K, Gifford K, Bougakov D, Goldberg E. Neuropsychological assessment in traumatic brain injury. Psychiatr Clin North Am. 2010;33:855–76. doi: 10.1016/j.psc.2010.08.003. [DOI] [PubMed] [Google Scholar]
- 11.Crippen DW. Head Trauma Treatment and Management. [Last accessed on 2012 Jul 3]. Available from: http://emedicine.medscape.com/article/433855-treatment .
- 12.Oja P, Titze S, Bauman A, de Geus B, Krenn P, Reger-Nash B, et al. Health benefits of cycling: A systematic review. Scand J Med Sci Sports. 2011;21:496–509. doi: 10.1111/j.1600-0838.2011.01299.x. [DOI] [PubMed] [Google Scholar]
- 13.Munivenkatappa A, Shukla DP, Devi BI, Kumarsamy AD, Bhat DI, Somanna S. Domestic animal-related neuro-trauma: An account, from a tertiary institute. J Neurosci Rural Pract. 2013;14:19–23. doi: 10.4103/0976-3147.105604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Selbst SM, Alexander D, Ruddy R. Bicycle-related injuries. Am J Dis Child. 1987;141:140–4. doi: 10.1001/archpedi.1987.04460020030021. [DOI] [PubMed] [Google Scholar]
- 15.Powell EC, Tanz RR. Cycling injuries treated in emergency departments need for bicycle helmets among preschoolers. Arch Pediatr Adolesc Med. 2000;154:1096–100. doi: 10.1001/archpedi.154.11.1096. [DOI] [PubMed] [Google Scholar]
- 16.Kiss K, Pótó Z, Pintér A, Sárközy S. Bicycle injuries in children: An analysis based on demographic density. Accid Anal Prev. 2010;42:1566–9. doi: 10.1016/j.aap.2010.03.014. [DOI] [PubMed] [Google Scholar]
- 17.Klin B, Rosenfeld-Yehoshua N, Abu-Kishk I, Efrati Y, Kozer E, Jeroukhimov I, et al. Bicycle-related injuries in children: Disturbing profile of a growing problem. Injury. 2009;40:1011–3. doi: 10.1016/j.injury.2009.01.135. [DOI] [PubMed] [Google Scholar]
- 18.Hefny AF, Eid HO, Grivna M, Abu-Zidan FM. Bicycle-related injuries requiring hospitalization in the United Arab Emirates. J Injury. 2012;43:1547–50. doi: 10.1016/j.injury.2011.05.016. [DOI] [PubMed] [Google Scholar]
- 19.Uibel S, Müller D, Klingelhoefer D, Groneberg DA. Bicycle helmet use and non-use-recently published research. J Occup Med Toxicol. 2012;7:9. doi: 10.1186/1745-6673-7-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Shukla D, Devi BI, Agrawal A. Outcome measures for traumatic brain injury. Clin Neurol Neurosurg. 2011;113:435–41. doi: 10.1016/j.clineuro.2011.02.013. [DOI] [PubMed] [Google Scholar]
- 21.Schepers JP, Kroeze PA, Sweers W, Wust JC. Road factors and Bicycle-Motor vehicle crashes at unsignalized priority intersections. Accid Anal Prev. 2011;43:853–61. doi: 10.1016/j.aap.2010.11.005. [DOI] [PubMed] [Google Scholar]
- 22.Reynolds CC, Harris MA, Teschke K, Cripton PA, Winters M. The impact of transportation infrastructure on bicycling injuries and crashes: A review of the literature. Environ Health. 2009;8:47. doi: 10.1186/1476-069X-8-47. [DOI] [PMC free article] [PubMed] [Google Scholar]