

Abstract
Purpose
Statins are widely used for preventing cardiovascular disease, yet recent reports suggest an increased risk of acute kidney injury (AKI). We estimated the one-year risk of AKI associated with statin initiation and determined the comparative safety of individual statin formulations.
Methods
We performed a cohort study in insurance billing data from commercial and Medicare insurance plans in the United States for the years 2000—2010. We identified statin initiators and non-users with histories of medication use and healthcare utilization. AKI diagnosis codes were identified in the one year following the index date. We estimated hazard ratios (HR) and 95% confidence intervals (CI) with adjusted and propensity score (PS)-matched Cox-proportional hazards models. Models were run separately in insurance groups and adjusted for cardiovascular and renal risk factors, markers of healthcare utilization, and other medication use.
Results
We identified 3,905,155 statin initiators and 2,817,621 eligible non-users. The adjusted HR of AKI in statin initiators compared to non-users was: commercial, HR=1.04 (95% CI: 0.99, 1.09); Medicare, HR=0.72 (95% CI: 0.70, 0.75). PS-matching yielded: commercial, HR=0.82 (95% CI: 0.78, 0.87); Medicare HR=0.66 (95% CI: 0.63, 0.69). As individual formulations, higher-potency simvastatin was associated with an increased risk of AKI over lower-potency simvastatin in adjusted models: commercial, HR=1.42 (95% CI: 1.28, 1.58Medicare, HR=1.24 (95% CI: 1.15, 1.35).
Conclusions
As a class, statin initiation was not associated with an increase in AKI. However, higher-potency simvastatin did exhibit an increased AKI risk.
Keywords: comparative effectiveness, drug safety, acute kidney injury, propensity scores
Introduction
Statin use has become widespread in the United States (US) over the past decade.1 Statins are a mainstay of lipid management and an integral part of both primary and secondary cardiovascular disease (CVD) prevention.1–3 It has been suggested that statins have anti-inflammatory4 and other pleiotropic effects5–7 beyond their lipid-lowering function. Consequently, their use has been advocated in populations previously considered at low risk for CVD,8–10 raising new concerns about their renal safety profile. Previous data suggests that they are generally well-tolerated by the kidneys with two notable exceptions: myopathy-induced acute kidney injury (AKI) mediated by rhabdomyolysis;11,12 and proteinuria in rosuvastatin users.13 Expert panels have concluded that statins do not lead to AKI or tubular injury in the absence of myopathy, 14,15 however the primary data source for these recommendations were intervention studies designed to detect beneficial effects which may be too small to detect rare adverse events. In contrast, reports from the Food and Drug Administration reporting system16 suggest that statins may be associated with increased AKI risk, and, a study of over 2 million individuals from the United Kingdom demonstrated a nearly two-fold increased risk of AKI with statin use, with a dose response effect, but no apparent differences by potency.17 Other recent reports suggest increased AKI in higher- versus lower-potency statins.18,19 Non-randomized studies of statins are complicated by the lack of an exchangeable comparator drug or an easily identifiable comparable non-user group; treatment effect estimates can vary widely depending on the referent used. Clinical trials or well-designed observational studies would employ a comparison group of non-users or other medication users with a similar risk of the outcome. However, it is difficult to identify an exchangeable comparison group in non-randomized settings,20 particularly using administrative claims where difficult-to-measure behavioral and lifestyle factors, access to and utilization of healthcare, and non-billable clinical factors (obesity, smoking, family history, etc.) can all contribute to both the risk of AKI and statin initiation. Prior studies17 note large differences in patient health status between statin users and non-users, potentially introducing confounding by indication.
We conducted a study of the renal safety of statins in a large population-based cohort in the US. We examined the one-year risk of AKI among statin initiators versus non-users. Furthermore, we studied the comparative renal safety of individual statin formulations, and of higher-potency versus lower-potency statins.
Methods
Study population
We employed two large employer-based insurance claims databases: the Truven Health Analytics MarketScan® Commercial Claims and Encounters and Medicare Supplemental and Coordination of Benefits databases. These are compilations of insurance billing data from large, employer-based insurance plans from across the US. Adjudicated, paid inpatient, outpatient and pharmacy claims, and plan enrollment information are available in the databases for employees, dependents and retirees. All analyses were performed separately in the two databases: commercial, employer-based insurance (ages 40 – 64); and Medicare supplementary insurance (ages 65+).
This analysis using deidentified billing claims was ruled exempt from further review by the Institutional Review Board of the University of North Carolina at Chapel Hill (UNC).
Treatment ascertainment
We implemented a new user design21 where statin initiators were identified from pharmacy dispensing claims following 180 days without a statin prescription (see Figure 1). We required at least one, non-statin medication claim during the 180-day baseline period to ensure pharmacy benefit utilization. The formulation of the index statin prescription was labeled as either higher-potency or lower-potency based on formulation and dosage (see Table 1). Initiators of cerivastatin sodium were excluded due to its documented risk of myopathy and rhabdomyolysis and subsequent removal from the market.22,23
Figure 1.
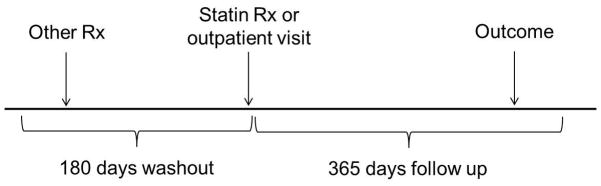
Table 1.
Statin potencies by formulation and dosage
| Formulation | Higher-potency dosages | Lower-potency dosages |
|---|---|---|
| Atorvastatin | > 10 mg | ≤ 10 mg |
| Fluvastatin | none | all |
| Lovastatin | > 40 mg | ≤ 40 mg |
| Pravastatin | none | all |
| Rosuvastatin | > 5mg | ≤ 5 mg |
| Simvastatin | > 40 mg | ≤ 40 mg |
A cohort of healthcare-seeking non-users was obtained by identifying individuals with an outpatient physician’s visit with a procedure code for an office visit or consultation (Current Procedural Terminology codes 99201–99205, 99211–99215, 99241–99245, 99271–99275) following 180 statin-free days. Similarly to the statin initiators, non-users were required to have at least one other medication dispensing during baseline. If a patient had eligible periods of non-use and initiation, only the first statin-initiation period was considered.
The date of the initial statin prescription (for initiators) or physician’s visit (for non-users) was considered the index date. The patient entered the cohort on the following day and was considered a statin initiator or non-user in a first exposure carried forward analysis to avoid potential bias by informative censoring due to discontinuation because of early muscle or renal symptoms.
Outcome Ascertainment
Inpatient and outpatient claims were searched for International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) diagnosis codes for acute renal failure (ARF) (ICD-9-CM 584.5 – 584.9) for up to one year following the index date or until censoring due to end of study or plan disenrollment. The validity of these codes has been investigated24,25; the positive predictive value varied widely across populations and reference standards (median, 67%; range. 15%–96%). The sensitivity has been shown to be quite low depending on the reference standard (26.2% – 47.6%), but the specificity is consistently very high (97.7% – 99.2%). Both statin initiators and non-users have histories of medication use and physician observation, so it seems unlikely that differential misclassification of AKI status would occur between treatment groups. Valid relative effect measures can still be estimated in situations with very high specificity under the assumption of nondifferential misclassification across treatment groups.26,27 We considered an expanded renal failure definition as a sensitivity analysis which included ARF, end-stage renal disease (ICD-9-CM 585.6), unspecified renal failure (ICD-9-CD 586), or a dialysis procedure code.
Covariate information
Inpatient and outpatient claims during the baseline period, including the index date, were investigated for diagnosis and procedure codes for cardiovascular and renal risk factors, recent acute events, healthcare utilization, and CVD management. For a complete list of considered covariates, see Table 2.
Table 2.
Distribution of patient characteristics by treatment group and data source
| –Commercial insurance | Medicare | |||
|---|---|---|---|---|
|
| ||||
| Statin Non-user (n=2,461,591) | Statin initiator (n=2,731,839) | Statin Non-user (n=356,030) | Statin initiator (n=1,173,316) | |
| Demographics | ||||
| Male, % | 37.1 | 48.56 | 38.33 | 43.87 |
| Mean age, standard deviation (SD) | 47.4 (7.5) | 53.9 (6.5) | 75.2 (8.0) | 74.1 (6.6) |
| CVD Management | ||||
| Angiography performed, % | 0.04 | 0.91 | 0.05 | 0.90 |
| Cardiac stress test performed, % | 1.06 | 8.95 | 1.67 | 11.06 |
| Echocardiograph, % | 1.69 | 9.85 | 4.76 | 17.40 |
| Mean number of lipid tests (SD) | 0.24 (0.55) | 1.02 (1.02) | 0.09 (0.36) | 0.33 (0.76) |
| Mean number of creatinine measurements (SD) | 0.00 (0.08) | 0.01 (0.17) | 0.00 (0.05) | 0.01 (0.12) |
| CVD & Comorbidities | ||||
| Diabetes, % | 3.76 | 23.10 | 6.81 | 22.65 |
| Chronic kidney disease, % | 0.21 | 1.12 | 0.79 | 2.93 |
| Other kidney disease, % | 0.06 | 0.25 | 0.08 | 0.28 |
| Proteinuria, % | 0.02 | 0.06 | 0.01 | 0.04 |
| Hypertension, % | 13.83 | 38.41 | 22.92 | 40.85 |
| Hyperlipidemia, % | 7.60 | 52.74 | 5.36 | 30.22 |
| Ischemic heart disease*, % | 0.63 | 10.26 | 4.12 | 22.37 |
| Atrial fibrillation, % | 0.33 | 1.61 | 3.36 | 7.42 |
| Chronic liver disease or cirrhosis, % | 0.60 | 1.38 | 0.60 | 0.92 |
| Multiple myeloma, % | 0.01 | 0.05 | 0.09 | 0.13 |
| Systemic lupus erythematosus, % | 0.28 | 0.43 | 0.13 | 0.32 |
| Metabolic disorders, % | 0.37 | 0.82 | 0.50 | 0.87 |
| Acute Events | ||||
| Myocardial infarction (MI) in previous 2 weeks, % | 0.03 | 1.32 | 0.12 | 2.00 |
| MI, within previous 6 months, % | 0.05 | 1.63 | 0.30 | 2.77 |
| History of MI, % | 0.03 | 0.48 | 0.17 | 0.99 |
| Unstable angina in previous 2 weeks, % | 0.06 | 1.48 | 0.18 | 2.15 |
| Unstable angina in previous 6 months, % | 0.06 | 0.74 | 0.28 | 1.45 |
| Stroke, % | 0.48 | 3.38 | 3.80 | 10.92 |
| Coronary artery bypass graft, % | 0.01 | 0.68 | 0.06 | 1.32 |
| Insertion of a coronary stent, % | 0.03 | 2.12 | 0.09 | 3.04 |
| Angioplasty, % | 0.01 | 0.26 | 0.03 | 0.47 |
| Heart failure, % | 0.26 | 1.59 | 3.43 | 6.38 |
| Sepsis, % | 0.03 | 0.05 | 0.08 | 0.15 |
| Prevalent medication use | ||||
| Angiotensin converting enzyme (ACE) inhibitors, % | 8.99 | 24.84 | 22.52 | 31.91 |
| Angiotensin receptor blockers (ARBs), % | 4.61 | 13.23 | 9.79 | 17.22 |
| Beta blockers, % | 8.09 | 20.46 | 24.14 | 37.14 |
| Calcium channel blockers, % | 5.56 | 14.22 | 19.60 | 25.72 |
| Anti-platelet agents, % | 0.65 | 3.95 | 3.90 | 10.31 |
| Alpha blockers, % | 1.00 | 3.19 | 5.60 | 8.21 |
| Thiazides, % | 10.53 | 24.05 | 23.59 | 28.82 |
| Potassium-sparing diuretics, % | 2.81 | 5.33 | 8.10 | 8.53 |
| Loop diuretics, % | 1.10 | 4.14 | 9.78 | 12.98 |
| Niacin, % | 0.25 | 1.49 | 0.38 | 1.62 |
| Fibrates, % | 1.14 | 4.94 | 2.20 | 4.78 |
| Ezetimibe, % | 0.32 | 2.54 | 0.98 | 3.93 |
| Anti-coagulants, % | 0.73 | 2.30 | 5.24 | 8.43 |
| Non-steroidal anti-inflammatory agents (NSAIDS), % | 3.67 | 2.88 | 1.41 | 2.99 |
| Concurrent medication initiation | ||||
| ACE inhibitors, % | 1.80 | 9.94 | 0.62 | 10.99 |
| ARBs, % | 0.65 | 4.38 | 0.17 | 4.64 |
| Beta blockers, % | 1.32 | 7.7 | 0.50 | 12.18 |
| Calcium channel blockers, % | 0.98 | 5.18 | 0.37 | 7.44 |
| Anti-platelet agents, % | 0.10 | 3.15 | 0.11 | 5.73 |
| Alpha blockers, % | 0.15 | 1.28 | 0.14 | 2.60 |
| Thiazides, % | 1.98 | 7.04 | 0.79 | 7.11 |
| Potassium-sparing diuretics, % | 0.47 | 1.31 | 0.27 | 1.97 |
| Loop diuretics, % | 0.19 | 1.22 | 0.43 | 3.55 |
| Niacin, % | 0.04 | 1.67 | 0.02 | 1.10 |
| Fibrates, % | 0.15 | 1.49 | 0.04 | 0.95 |
| Ezetimibe, % | 0.03 | 7.30 | 0.02 | 6.06 |
| Anti-coagulants, % | 0.10 | 0.62 | 0.14 | 2.13 |
| NSAIDs, % | 3.67 | 2.88 | 1.41 | 2.99 |
Not counting myocardial infarction or unstable angina
Pharmacy dispensing claims during the baseline window were searched for prevalent use of additional medications. Medications that were not used during the baseline window but were newly-initiated within one day of the index date (day −1, 0, or 1)were considered as concurrently initiated medications and were included as separate variables in the analysis.
To restrict to those without a history of renal failure, we excluded individuals with baseline diagnoses of ARF, ESRD, unspecified renal failure, or a procedure code for dialysis.
Statistical analyses
We estimated adjusted hazard ratios (HR) and 95% confidence intervals (CI) with multivariable Cox proportional hazards models. Follow-up began the day after the index date and continued until censoring at the first occurrence of: the event of interest; plan disenrollment; one year after the index date; or end of the study period (December 31, 2010). We repeated the analyses stratified by sex, and within clinically-relevant subgroups at higher-risk for AKI—those with diabetes, hypertension or chronic kidney disease (CKD)—or those with acute coronary syndrome (ACS) occurring within the 20 days prior to the index date. We also estimated the comparative safety of higher-potency versus lower-potency statins and of individual statin formulations versus lower-potency simvastatin, as lower-potency simvastatin was the most broadly-used formulation in our sample.
All analyses were performed using SAS 9.2 (SAS Institute, Inc., Cary, NC).
Propensity score methods
We estimated the predicted probability, or propensity score (PS) of statin initiation for each comparison using the measured covariates in logistic regression models. The distribution of the PS by treatment group was plotted to assess the extent to which the treatment groups appeared exchangeable with respect to the measured confounders. To assess treatment effect heterogeneity, we created 50 equal strata along the PS distribution and plotted the estimated the HRs within each strata.
We 1:1 matched non-users to initiators, matching to the fifth decimal place if possible using a greedy matching algorithm.28 Non-matching individuals were excluded from the analysis, and the HR was estimated within the matched cohort. This method estimates the effect of the treatment in those who received treatment and were successfully matched to non-users, rather than in the entire population29.
For the comparative formulation safety analysis, each formulation was weighted to the PS distribution of the low-potency simvastatin referent with a weight of: (1−PS)/PS. This created comparisons of each formulation with the same referent, creating directly comparable effect estimates.
Results
Statin initiators vs. non-users
The distribution of covariates between the treatment groups by insurance is shown in Table 2.
Ages 40 – 64: Commercial insurance
We identified 2,731,839 statin initiators and 2,461,591 eligible non-users. Statin initiators filled an average of 4.7 (SD 3.4) prescriptions during the year follow-up period for a mean of 207 (SD 106) days of prescription coverage. 31% of the initiators had continuous statin coverage throughout the entire year. Among the non-users, 0.5% initiated a statin during follow-up.
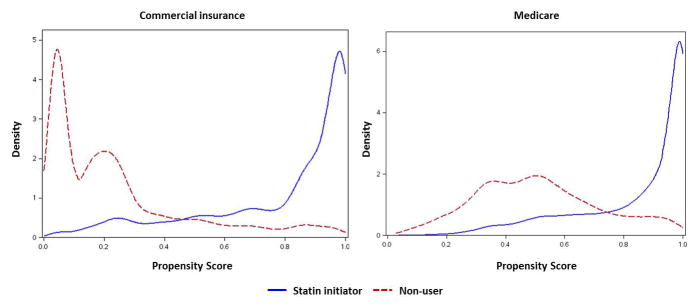
Statin initiators were older, had more CVD, more healthcare interactions, more comorbidity, and had more medication use than non-users. PS non-overlap between the treatment groups was pronounced (see Figure 2).
Figure 2.
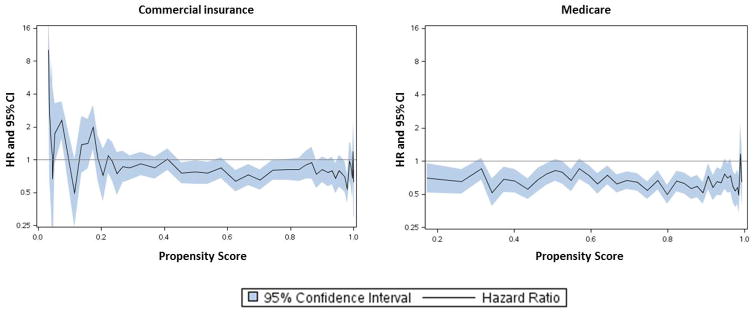
AKI was observed during one-year follow-up in 0.5% of the statin initiators and in 0.2% of the non-users. Crude Cox-proportional hazards models in the unmatched cohort revealed HR=2.81 (95% CI: 2.71, 2.91). The effect estimate was attenuated by multivariable adjustment to HR=1.04 (95% CI: 0.99, 1.09) (see Table 3). Upon propensity score matching of the statin initiators to non-users, 30.9% of the total sample successfully matched, resulting in HR=0.82 (95% CI: 0.78, 0.87). Treatment effect heterogeneity was observed along the distribution of the PS (see Figure 3), with substantially increased HRs in the lower extreme. The portions of the PS distribution with greatest overlap between treatment groups (approximately PS 0.3–0.7) which were retained in the PS-matched analysis (Figure 2) corresponded with the areas with lowest HR estimates (Figure 3).
Table 3.
Effect measure estimates of statin initiation versus non-use and higher-potency versus lower-potency statin use on acute kidney injury
| Crude | Adjusted* | Propensity Score* Matched | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
| Insurance group | Treatment | N | Events (%) | HR | 95% CI | HR | 95% CI | N | Events (%) | HR | 95% CI |
| Commercial insurance | Non-users | 2,461,591 | 4,241 (0.2) | -- | -- | -- | -- | 802,561 | 2,569 (0.3) | -- | -- |
| Statininitiators | 2,731,839 | 13,661 (0.5) | 2.81 | 2.71, 2.91 | 1.04 | 0.99, 1.09 | 802,561 | 2,237 (0.3) | 0.82 | 0.78, 0.87 | |
| Medicare | Non-users | 356,030 | 5,420 (1.5) | -- | -- | -- | -- | 272,695 | 4,295 (1.6) | -- | -- |
| Statininitiators | 1,173,316 | 23,122 (2.0) | 1.32 | 1.28, 1.35 | 0.72 | 0.70, 0.75 | 272,695 | 2,948 (1.1) | 0.66 | 0.63, 0.69 | |
| Commercial insurance | Lower-potency | 1,991,792 | 9,140 (0.5) | -- | -- | -- | -- | 734,904 | 5,873 (0.8) | -- | -- |
| Higher-potency | 736,212 | 4,490 (0.6) | 1.32 | 1.27, 1.37 | 1.12 | 1.08, 1.16 | 734,904 | 6,290 (0.9) | 1.09 | 1.05, 1.14 | |
| Medicare | Lower-potency | 885,259 | 16,708 (1.9) | -- | -- | -- | -- | 285,856 | 6,139 (2.2) | -- | -- |
| Higher-potency | 285,897 | 6,365 (2.2) | 1.18 | 1.14, 1.21 | 1.06 | 1.03, 1.09 | 285,856 | 6,363 (2.2) | 1.03 | 1.00, 1.07 | |
HR, Hazard ratio; CI, Confidence interval; ref, referent
Adjustment and propensity score model covariates include: sex; age; calendar year; presence of angiography, cardiac stress test stent, angioplasty, echocardiograph, coronary artery bypass grafting, myocardial infarction, unstable angina, other ischemic heart disease, stroke, diabetes, chronic kidney disease, proteinuria, hypertension, hyperlipidemia, atrial fibrillation, heart failure, chronic liver disease or cirrhosis, multiple myeloma, systemic lupus erythematosus, sepsis, metabolic disorders; number of creatinine measurements, lipid measurements; use or initiation of ACE inhibiors, ARBs, beta blockers, calcium channel blockers, anti-platelet agents, alpha blockers, thiazide diuretics, loop diuretics, firbates, ezetimibe, anti-coagulants, non-steroidal anti-inflammatory agents.
Figure 3.
Ages 65+: Medicare
Statin use was much more common among the Medicare population; we identified 1,173,316 eligible statin initiators and 356,030 eligible non-users. Statin initiators filled a mean of 4.6 (SD 3.2) prescriptions during the follow-up year for a mean of 217 (SD 98) days covered. 22.5% of the initiators maintained active statin prescriptions for the full year. Of the non-users, 0.8% initiated a statin during follow-up
The treatment groups were comparable in age, yet the statin initiators had more CVD, comorbidities, acute events, healthcare interactions, and medication use and co-initiation than non-users. PS overlap was greater in the Medicare group than the commercially insured, but there were still areas of considerable non-exchangeability, particularly above PS 0.8 (see Figure 2).
AKI was observed in 2.0% of the initiators and 1.5% of the non-users during follow-up. The crude HR was 1.32 (95% CI: 1.28, 1.35), and after adjustment, it changed to HR=0.72 (95% CI: 0.70, 0.75). Upon propensity score matching, 35.7% of the total sample successfully matched, resulting in HR= 0.66 (95% CI: 0.63, 0.69). When stratified by the PS distribution, the HR estimates were much more homogeneous (see Figure 3).
Sensitivity Analysis
In both age groups, when the expanded kidney failure outcome definition was considered, the effect measure estimates remained almost identical.
Subgroup Analyses
The rates of AKI were highest in those with CKD in both age groups. AKI occurrence was higher in all subgroups among the older Medicare groups than in the younger commercially insured. However, the effect of statin initiation appeared relatively constant over all subgroups within each estimation technique, with effect measure estimates tending to be lower among the Medicare group (see Table 4). Statin use was not associated with an increased risk of AKI in any subgroup.
Table 4.
Effect measure estimates of statin initiation versus non-use in relevant subgroups
| Crude | Adjusted* | Matched* | ||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Subgroup | N | Events % | HR | 95%CI | HR | 95%CI | HR | 95%CI |
| Commercial insurance | ||||||||
| Males | 2,239,132 | 10,363 (0.5) | 2.08 | 1.99, 2.17 | 0.90 | 0.85, 0.95 | 0.75 | 0.70, 0.80 |
| Females | 2,954,298 | 7,539 (0.3) | 3.57 | 3.38, 3.76 | 1.24 | 1.16, 1.33 | 0.91 | 0.83, 0.99 |
| CKD | 35,887 | 2,457 (6.9) | 1.21 | 1.07, 1.36 | 0.85 | 0.74, 0.98 | 0.84 | 0.70, 1.01 |
| Diabetes | 723,461 | 7,403 (1.0) | 1.26 | 1.17, 1.36 | 0.79 | 0.73, 0.86 | 0.74 | 0.66, 0.83 |
| Hypertension | 1,389,701 | 8,590 (0.6) | 1.83 | 1.73, 1.95 | 1.04 | 0.97, 1.12 | 0.94 | 0.86, 1.03 |
| Hyperlipidemia | 1,627,836 | 5,998 (0.4) | 2.06 | 1.84, 2.30 | 1.08 | 0.96, 1.21 | 0.93 | 0.78, 1.08 |
| Recent ACS | 93,274 | 1,147 (1.2) | 0.92 | 0.69, 1.22 | 0.77 | 0.58, 1.05 | 0.72 | 0.47, 1.11 |
| Medicare | ||||||||
| Males | 651,155 | 15,037 (2.3) | 1.20 | 1.15, 1.25 | 0.68 | 0.65, 0.72 | 0.59 | 0.55, 0.63 |
| Females | 878,191 | 13,505 (1.5) | 1.38 | 1.32, 1.44 | 0.77 | 0.73, 0.81 | 0.70 | 0.66, 0.75 |
| CKD | 37,143 | 3,994 (10.8) | 0.90 | 0.81, 1.01 | 0.64 | 0.57, 0.73 | 0.55 | 0.45, 0.66 |
| Diabetes | 723,461 | 7,403 (1.0) | 1.26 | 1.17, 1.36 | 0.62 | 0.58, 0.67 | 0.56 | 0.51, 0.63 |
| Hypertension | 560,951 | 12,966 (2.3) | 1.33 | 1.26, 1.40 | 0.76 | 0.72, 0.81 | 0.70 | 0.64, 0.76 |
| Hyperlipidemia | 373,695 | 6,023 (1.6) | 1.47 | 1.28, 1.69 | 0.77 | 0.70, 0.89 | 0.67 | 0.54, 0.82 |
| Recent ACS | 63,386 | 2,443 (3.7) | 0.78 | 0.65, 0.94 | 0.71 | 0.58, 0.86 | 0.73 | 0.56, 0.97 |
HR: Hazard ratio; CI: Confidence interval; CKD: Chronic kidney disease; ACS: Acute coronary syndrome
Adjustment and propensity score model covariates include: sex; age; calendar year; presence of angiography, cardiac stress test stent, angioplasty, echocardiograph, coronary artery bypass grafting, myocardial infarction, unstable angina, other ischemic heart disease, stroke, diabetes, chronic kidney disease, proteinuria, hypertension, hyperlipidemia, atrial fibrillation, heart failure, chronic liver disease or cirrhosis, multiple myeloma, systemic lupus erythematosus, sepsis, metabolic disorders; number of creatinine measurements, lipid measurements; use or initiation of ACE inhibiors, ARBs, beta blockers, calcium channel blockers, anti-platelet agents, alpha blockers, thiazide diuretics, loop diuretics, firbates, ezetimibe, anti-coagulants, non-steroidal anti-inflammatory agents
Higher-potency vs. lower-potency initiators
In the commercially insured statin initiators, 27.0% initiated a higher-potency statin. Among the Medicare initiators, 24.4% first used a higher-potency statin. In both groups, all effect measure estimation techniques yielded similar, minimally elevated risk estimated of higher-potency statin initiation versus lower-potency statins on AKI (see Table 3). PS distribution overlap was very good in these comparisons (see Web Appendix 1).
Comparative safety of statin formulations
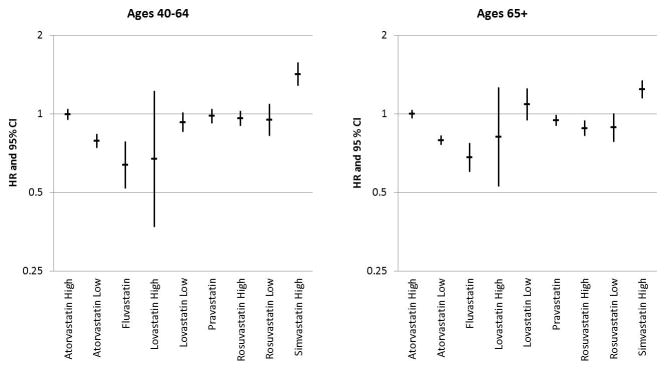
The risk of AKI in individual statin formulations was compared to lower-potency simvastatin within insurance groups. See Web Appendix 2 for PS distribution plots, which demonstrate very good overlap for each comparison. Lower-potency simvastatin-standardized models revealed generally similar hazards of AKI among the various formulations. Most formulations showed a comparable risk to that in lower-potency simvastatin (see Figure 4). In both age groups, adjusted models for higher-potency simvastatin demonstrated an increased one-year AKI risk: commercial, HR = 1.42 (95% CI: 1.28, 1.58); Medicare, HR = 1.24 (95% CI: 1.15, 1.35). Additionally, lower-potency atorvastatin and fluvastatin tended to carry the least AKI risk.
Figure 4.
Discussion
In this relatively low-risk cohort of over 6.5 million individuals, we found that the cumulative risk for AKI in statin initiators was about 0.5% in commercially-insured users and 2.0% in Medicare initiators. As a class, statin initiation was not associated with AKI after adjustment for known confounding variables; these findings remained constant with PS matching. However, we did find that higher-potency simvastatin was associated with an increased risk of AKI compared to lower-potency simvastatin among both commercially and Medicare insured adults. The increased risk of AKI associated with higher-potency simvastatin adds another potential safety concern to the documented risk of mylagias30 that has already prompted a safety warning from the Food and Drug Administration31. The greatly increased crude hazard ratios (commercially insured: HR=2.93, 95% CI: 2.61, 3.28; Medicare: HR=1.52, 95%CI: 1.41, 1.65) suggest that higher-potency simvastatin is used in higher risk patient populations than other statins, and the potential for residual confounding remains.
Consistent with some prior studies23,32, we did not observe a class effect of statins on renal safety. This analysis, with a sample size of over 6 million individuals, is arguably better powered to detect potential harms than previous analyses.
However, the findings of the study contrast markedly with results from a population-based investigation from the United Kingdom17 which demonstrated an increased risk of AKI associated with statin use (54% increase for women and 67% men) compared to non-use, and a greater risk of AKI with increasing dose of agent. A potential explanation for the difference is the composition of the non-user comparison group. The choice of comparison groups for studies of drug effects can have substantial influence on effect estimates20. Using a general sample of non-users may introduce younger, healthier individuals without the indication for treatment resulting in residual confounding by indication, as statin users are more likely to have high cholesterol levels, be treated for CVD, have acute CVD events, and have more comorbidities than younger, healthier controls who are not being treated or evaluated by physicians. To avoid this bias, we restricted our non-user group to individuals with a history of medication use and outpatient physician visits, creating a comparison group with similar healthcare utilization. Additionally, we performed comparisons between different statin-initiating groups (higher- versus lower-potency statins, individual formulations).
When compared with non-users, statin initiators tended to be have more risk factors, more healthcare utilization, and use more medications than non-users. However, PS methods allowed us to describe the exchangeability of treatment groups relative to measured confounders, identify areas of equipoise even in the presence of substantial non-overlap, and describe treatment effect heterogeneity over the propensity score distribution. This was evident particularly in the younger, commercially-insured population: at the lower propensity scores (less than 0.2), there were marked increased HR in the statin users at low PS. Both the initiators and non-users in this PS appear to have very few indications for statin treatment and few renal risk factors, yet the statin users experience more much more AKI. This could largely be attributed to confounding by unmeasured factors, including rare genetic disorders, extreme family histories, etc. which would lead to AKI and statin treatment in those without coded traditional risk factors. Characteristics were much better balanced within potency and formulation treatment groups.
Surprisingly, the results of the PS analyses suggest a modest protective effect of statin use against one-year risk of AKI. While these findings were robust across renal failure definitions, they should be interpreted conservatively. The a priori intent of the analysis was to examine potential renal injury associated with statin initiation, rather than benefit. Furthermore, given the low occurrence of AKI in this relatively low-risk population, the estimated absolute reduction of AKI in statin initiators may not be clinically meaningful. A large proportion of the sample failed to match, reducing the generalizability of the PS-matched estimates. However, the non-matching were those without equipoise between statin treatment and non-treatment—either highly likely or very unlikely to have received statin treatment. Therefore, the resulting matched population represents those patients of greatest interest in this study of a potentially rare adverse event: those who have a realistic option whether or not to initiate a statin. However, these results are not reflective of the entire statin-initiating population do not justify widespread use of statins as a preventive therapy for AKI.
These results must be interpreted in light of several important limitations. As with all administrative claims-based studies, information on kidney function, cardiovascular risk, and other covariates and outcomes is derived from coded reimbursement claims rather than biomarkers and diagnostic test results. Consequently, key risk factors for AKI and CVD such as glomerular filtration rate, blood lipids, obesity, smoking, and family history of CVD or renal disease are either unavailable or only indirectly available through ICD-9 codes. When present, diagnostic codes or proxies for health status (e.g. healthcare utilization, screening, etc.) were used as potential covariates.
In particular, baseline kidney function—a strong predictor of AKI—could only be ascertained from billing codes for CKD which are known to have low sensitivity but high specificity.25 While we adjusted for the presence of non-ESRD CKD diagnosis codes, they occurred infrequently (see Table 2). Yet, it is unlikely that the reliance on the codes for CKD would have meaningfully biased the results; only information available to the prescriber at the time of medication prescription can confound the drug-outcome relationship. While baseline renal function is an important AKI risk factor, such information is likely unknown at the time of prescribing in these low-risk patients.33–35 Furthermore, it is unlikely that statin use or agent was preferentially affected by renal status given that most statins do not require dose modifications according to renal function.
Another limitation of the study is the low sensitivity of AKI using billing codes,36 which may underestimate AKI incidence. Yet, previous studies of community-acquired AKI have demonstrated a comparable, low frequency of AKI despite the use of serum creatinine measures.37–40 Furthermore, given the high specificity of billing codes for AKI,36 measures of relative effect, such as the reported HRs, may still be unbiased.26,27
This study contains several notable strengths. First, our analysis is based on a very large cohort from throughout the US with carefully selected comparison groups. Secondly, we employed propensity score methods to select cohorts with similar characteristics, control for confounding, and describe heterogeneity in a way which standard analyses would have been unable to do. We considered several measures of CVD severity, healthcare utilization, concurrent medication initiation, and other relevant clinical factors as adjustment factors. Lastly, our findings were robust over sensitivity analyses, including an expanded renal failure definition and multiple estimation techniques.
In conclusion, statin initiation was not associated with an increased risk of AKI among most individuals. However, there was an increased risk of AKI associated with higher-potency simvastatin. These finding provide new information to help weigh the risks and benefits of statins agents as the debate about their expanded use continues.
Key points.
Statins as a class are not associated with increased AKI
Higher-potency simvastatin carried an increased risk of AKI
Treatment effect heterogeneity across the propensity score distribution can explain differences in effect estimates from different propensity score-based methods.
Acknowledgments
Sponsors: This research was supported by an NIH NIDDK training grant from in renal epidemiology to Dr. Layton administered by the UNC Kidney Center (5 T32 DK007750-13, PI: RJ Falk)
Footnotes
Presentations: Portions of this work have been presented at the 2012 American Society of Nephrology Kidney Week in San Diego, CA, and other portions have been accepted for publication at the 2013 International Convention on Pharmacoepidemiology and Therapeutic Risk Management in Montreal, Canada.
Conflicts: Dr. Layton, Ms. Pate, Dr. Kshirsagar have no conflicts to declare.
Dr. Brookhart has served on scientific advisory boards for Pfizer, with honoraria either donated to charity or received by UNC.
Dr. Simpson has received research support from Merck, and honoraria for lectures from Merck and Pfizer.
Dr. Jonsson Funk: GlaxoSmithKline (GSK) has a collaborative agreement with the Center for Pharmacoepidemiology, Department of Epidemiology, UNC Chapel Hill. GSK does not review any research nor provide any input into the analysis of the drug classes being studied.
Dr. Stürmer receives investigator-initiated research funding and support as Principal Investigator (RO1 AG023178) and Co-Investigator (RO1 AG018833) from the National Institute on Aging at the National Institutes of Health. He also receives research funding as Principal Investigator of the UNC-DEcIDE center from the Agency for Healthcare Research and Quality. Dr. Stürmer does not accept personal compensation of any kind from any pharmaceutical company, though he receives salary support from the Center for Pharmacoepidemiology in the Department of Epidemiology at UNC and from unrestricted research grants from pharmaceutical companies to UNC.
References
- 1.Spatz ES, Canavan ME, Desai MM. From here to JUPITER: identifying new patients for statin therapy using data from the 1999–2004 National Health and Nutrition Examination Survey. Circulation Cardiovascular quality and outcomes. 2009;2:41–8. doi: 10.1161/CIRCOUTCOMES.108.832592. [DOI] [PubMed] [Google Scholar]
- 2.Lin V, Holman JR. Which drugs should post-MI patients routinely receive? The Journal of Family Practice. 2010;59:527–9. [PubMed] [Google Scholar]
- 3.Mills EJ, Wu P, Chong G, et al. Efficacy and safety of statin treatment for cardiovascular disease: a network meta-analysis of 170,255 patients from 76 randomized trials. QJM: monthly journal of the Association of Physicians. 2011;104:109–24. doi: 10.1093/qjmed/hcq165. [DOI] [PubMed] [Google Scholar]
- 4.Albert MA, Danielson E, Rifai N, Ridker PM. Effect of statin therapy on C-reactive protein levels: the pravastatin inflammation/CRP evaluation (PRINCE): a randomized trial and cohort study. JAMA: the journal of the American Medical Association. 2001;286:64–70. doi: 10.1001/jama.286.1.64. [DOI] [PubMed] [Google Scholar]
- 5.Giusti-Paiva A, Martinez MR, Felix JV, et al. Simvastatin decreases nitric oxide overproduction and reverts the impaired vascular responsiveness induced by endotoxic shock in rats. Shock. 2004;21:271–5. doi: 10.1097/10.shk.0000115756.74059.ce. [DOI] [PubMed] [Google Scholar]
- 6.Haslinger-Loffler B. Multiple effects of HMG-CoA reductase inhibitors (statins) besides their lipid-lowering function. Kidney Int. 2008;74:553–5. doi: 10.1038/ki.2008.323. [DOI] [PubMed] [Google Scholar]
- 7.McFarlane SI, Muniyappa R, Francisco R, Sowers JR. Clinical review 145: Pleiotropic effects of statins: lipid reduction and beyond. The Journal of clinical endocrinology and metabolism. 2002;87:1451–8. doi: 10.1210/jcem.87.4.8412. [DOI] [PubMed] [Google Scholar]
- 8.Tonelli M, Lloyd A, Clement F, et al. Efficacy of statins for primary prevention in people at low cardiovascular risk: a meta-analysis. CMAJ: Canadian Medical Association journal = journal de l’Association medicale canadienne. 2011;183:E1189–202. doi: 10.1503/cmaj.101280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brugts JJ, Yetgin T, Hoeks SE, et al. The benefits of statins in people without established cardiovascular disease but with cardiovascular risk factors: meta-analysis of randomised controlled trials. Bmj. 2009;338:b2376. doi: 10.1136/bmj.b2376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Blaha MJ, Nasir K, Blumenthal RS. Statin therapy for healthy men identified as “increased risk”. JAMA: the journal of the American Medical Association. 2012;307:1489–90. doi: 10.1001/jama.2012.425. [DOI] [PubMed] [Google Scholar]
- 11.Hedenmalm K, Alvan G, Ohagen P, Dahl ML. Muscle toxicity with statins. Pharmacoepidemiology and drug safety. 2010;19:223–31. doi: 10.1002/pds.1895. [DOI] [PubMed] [Google Scholar]
- 12.Ahn SC. Neuromuscular complications of statins. Physical medicine and rehabilitation clinics of North America. 2008;19:47–59. vi. doi: 10.1016/j.pmr.2007.10.002. [DOI] [PubMed] [Google Scholar]
- 13.Gray J, Edwards SJ, Lip GY. Comparison of sequential rosuvastatin doses in hypercholesterolaemia: a meta-analysis of randomised controlled trials. Current medical research and opinion. 2010;26:537–47. doi: 10.1185/03007990903513980. [DOI] [PubMed] [Google Scholar]
- 14.Kasiske BL, Wanner C, O’Neill WC. An assessment of statin safety by nephrologists. The American journal of cardiology. 2006;97:82C–5C. doi: 10.1016/j.amjcard.2005.12.015. [DOI] [PubMed] [Google Scholar]
- 15.McKenney JM, Davidson MH, Jacobson TA, Guyton JR. Final conclusions and recommendations of the National Lipid Association Statin Safety Assessment Task Force. The American journal of cardiology. 2006;97:89C–94C. doi: 10.1016/j.amjcard.2006.02.030. [DOI] [PubMed] [Google Scholar]
- 16.Sakaeda T, Kadoyama K, Okuno Y. Statin-associated muscular and renal adverse events: data mining of the public version of the FDA adverse event reporting system. PloS one. 2011;6:e28124. doi: 10.1371/journal.pone.0028124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hippisley-Cox J, Coupland C. Unintended effects of statins in men and women in England and Wales: population based cohort study using the QResearch database. Bmj. 2010;340:c2197-c. doi: 10.1136/bmj.c2197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dormuth CR, Hemmelgarn BR, Paterson JM, et al. Use of high potency statins and rates of admission for acute kidney injury: multicenter, retrospective observational analysis of administrative databases. Bmj. 2013;346:f880. doi: 10.1136/bmj.f880. [DOI] [PubMed] [Google Scholar]
- 19.Keys DO, Edelstein CL. High-potency statins are associated with increased hospitalisations with acute kidney injury. Evidence-based medicine. 2013 doi: 10.1136/eb-2013-101357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Schneeweiss S, Patrick AR, Sturmer T, et al. Increasing levels of restriction pharmacoepidemiologic database studies of elderly and comparison with randomized trial results. Med Care. 2007;45:S131–S42. doi: 10.1097/MLR.0b013e318070c08e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ray WA. Evaluating Medication Effects Outside of Clinical Trials: New-User Designs. American Journal of Epidemiology. 2003;158:915–20. doi: 10.1093/aje/kwg231. [DOI] [PubMed] [Google Scholar]
- 22.Graham DJ, Staffa JA, Shatin D, et al. Incidence of hospitalized rhabdomyolysis in patients treated with lipid-lowering drugs. JAMA: the journal of the American Medical Association. 2004;292:2585–90. doi: 10.1001/jama.292.21.2585. [DOI] [PubMed] [Google Scholar]
- 23.Cziraky MJ, Willey VJ, McKenney JM, et al. Statin safety: an assessment using an administrative claims database. The American journal of cardiology. 2006;97:61C–8C. doi: 10.1016/j.amjcard.2005.12.011. [DOI] [PubMed] [Google Scholar]
- 24.Waikar SS, Wald R, Chertow GM, et al. Validity of International Classification of Diseases, Ninth Revision, Clinical Modification Codes for Acute Renal Failure. Journal of the American Society of Nephrology: JASN. 2006;17:1688–94. doi: 10.1681/ASN.2006010073. [DOI] [PubMed] [Google Scholar]
- 25.Vlasschaert ME, Bejaimal SA, Hackam DG, et al. Validity of administrative database coding for kidney disease: a systematic review. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2011;57:29–43. doi: 10.1053/j.ajkd.2010.08.031. [DOI] [PubMed] [Google Scholar]
- 26.Chubak J, Pocobelli G, Weiss NS. Tradeoffs between accuracy measures for electronic health care data algorithms. Journal of clinical epidemiology. 2012;65:343–9. e2. doi: 10.1016/j.jclinepi.2011.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Greenland S, Lash TL. Bias analysis. In: Rothman KJ, Greenland S, Lash TL, editors. Modern Epidemiology. 3. Philadelphia, PA: Lippincott Williams & Wilkins; 2008. [Google Scholar]
- 28.Parsons LS. Reducing bias in a propensity score matched-pair sample using greedy matching techniques. SAS Institute Inc; 2001. pp. 214–26. [Google Scholar]
- 29.Sturmer T, Rothman KJ, Glynn RJ. Insights into different results from different causal contrasts in the presence of effect-measure modification. Pharmacoepidemiology and drug safety. 2006;15:698–709. doi: 10.1002/pds.1231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Backes JM, Howard PA, Ruisinger JF, Moriarty PM. Does simvastatin cause more myotoxicity compared with other statins? The Annals of pharmacotherapy. 2009;43:2012–20. doi: 10.1345/aph.1M410. [DOI] [PubMed] [Google Scholar]
- 31.Administration USFaD. FDA Drug Safety Communication: New restrictions, contraindications, and dose limitations for Zocor (simvastatin) to reduce the risk of muscle injury. Rockville, MD: 2011. Jun 08, [Google Scholar]
- 32.Kashani A, Phillips CO, Foody JM, et al. Risks associated with statin therapy: a systematic overview of randomized clinical trials. Circulation. 2006;114:2788–97. doi: 10.1161/CIRCULATIONAHA.106.624890. [DOI] [PubMed] [Google Scholar]
- 33.Abeygunasekara SC, Horner CW. High prevalence of undiagnosed kidney disease in those presenting with troponin positive acute coronary syndrome. Renal failure. 2012;34:845–8. doi: 10.3109/0886022X.2012.690716. [DOI] [PubMed] [Google Scholar]
- 34.Llisterri Caro JL, Gorriz Teruel JL, Alonso Moreno FJ, et al. Prevalence of undetected chronic kidney disease in dyslipidemic population treated in primary care LIPICAP study. Medicina clinica. 2008;130:127–32. doi: 10.1157/13115785. [DOI] [PubMed] [Google Scholar]
- 35.Whaley-Connell AT, Sowers JR, Stevens LA, et al. CKD in the United States: Kidney Early Evaluation Program (KEEP) and National Health and Nutrition Examination Survey (NHANES) 1999–2004. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2008;51:S13–20. doi: 10.1053/j.ajkd.2007.12.016. [DOI] [PubMed] [Google Scholar]
- 36.Winkelmayer WC, Schneeweiss S, Mogun H, Patrick AR, Avorn J, Solomon DH. Identification of individuals with CKD from Medicare claims data: a validation study. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2005;46:225–32. doi: 10.1053/j.ajkd.2005.04.029. [DOI] [PubMed] [Google Scholar]
- 37.Kaufman J, Dhakal M, Patel B, Hamburger R. Community-acquired acute renal failure. American journal of kidney diseases: the official journal of the National Kidney Foundation. 1991;17:191–8. doi: 10.1016/s0272-6386(12)81128-0. [DOI] [PubMed] [Google Scholar]
- 38.Feest TG, Round A, Hamad S. Incidence of severe acute renal failure in adults: results of a community based study. Bmj. 1993;306:481–3. doi: 10.1136/bmj.306.6876.481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Liano F, Pascual J. Epidemiology of acute renal failure: a prospective, multicenter, community-based study. Madrid Acute Renal Failure Study Group. Kidney Int. 1996;50:811–8. doi: 10.1038/ki.1996.380. [DOI] [PubMed] [Google Scholar]
- 40.Obialo CI, Okonofua EC, Tayade AS, Riley LJ. Epidemiology of de novo acute renal failure in hospitalized African Americans: comparing community-acquired vs hospital-acquired disease. Arch Intern Med. 2000;160:1309–13. doi: 10.1001/archinte.160.9.1309. [DOI] [PubMed] [Google Scholar]