

Abstract
The nonsurgical correction of congenital ear deformities has been reported in the world literature. To date, there has been little interest in this procedure in pediatric centres and no reports in the Canadian literature. Two case reports are presented with a review of the literature. A description of this simple, user friendly office procedure is presented.
Keywords: Ears, Nonsurgical, Protruding
Abstract
La correction non chirurgicale des malformations congénitales des oreilles est présentée dans la documentation médicale mondiale. Jusqu’à présent, on s’est peu intéressé à ces interventions dans les centres pédiatriques, et on ne trouve aucun compte rendu à ce sujet dans la documentation canadienne. Deux rapports de cas sont présentés, de même qu’une analyse bibliographique. Une description de cette intervention simple et conviviale effectuée en cabinet est exposée.
The concept of nonsurgical correction of congenital ear abnormalities is present in the world literature (1,2). However, this treatment modality has not been widely adopted by pediatric centres in Canada and has not been reported in the Canadian literature. Two cases of protruding ears treated with this simple nonsurgical method are presented.
CASE PRESENTATIONS
Case 1
The patient was first reviewed at six months of age. The patient’s mother had not noticed any abnormality of the ears at birth. By three months of age, the ears appeared to be protruding, with the left worse than the right. The initial measurement of the distance from the medial aspect of the upper helix to the scalp was 1.5 cm (right ear). After discussion, the mother requested an intervention, which began at six months of age. The hair above the ear was shaved (5 cm). The outer helix of the left ear was waxed with dental wax (Utility Wax Rods Round-Kerr, Sybron, USA) and the ear was taped (Hypafix Tape, Medipore 3M, USA) (Figure 1). The tape was left on for a month and removed before the monthly visit. The patient’s mother obtained pictures before any intervention and then after one, two and three months (Figure 2). The final measurement of the protruding ear was 1.0 cm. The patient’s mother declared the results to be excellent, “the auricle was delicately corrected into a desirable form and satisfied the patient/parent” (3).
Figure 1).

A Wax, tape ear; B Wax applied to ear; C Tape applied to ear
Figure 2).
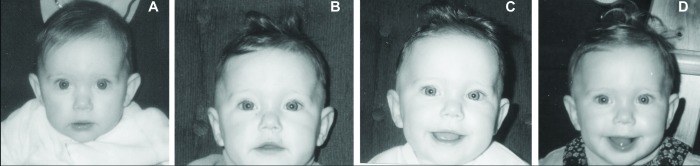
Case 1: A Before intervention; B One month following intervention; C Two months following intervention; D Three months following intervention
Case 2
The patient was first reviewed at five months of age. The patient’s mother first noticed that the right ear was protruding at two months of age. She was initially told that this would correct with age, and was then directed to a plastic surgeon at five months (JWT) and redirected to the pediatrician’s office. The initial evaluation revealed somewhat protruding ears with the right more protruding than the left. The distance measured from the medial aspect of the upper helix to the scalp was 1.6 cm (right ear). After discussion, the patient’s mother requested intervention. The hair was shaved at home 5 cm above the ear. Dental wax was placed in the helix and taped. The tape was removed before each monthly visit. The mother obtained photographs at the end of each month’s taping (Figure 3). The final measurement of the protruding ear was 1.1 cm (right ear). The mother declared the results to be excellent (3).
Figure 3).
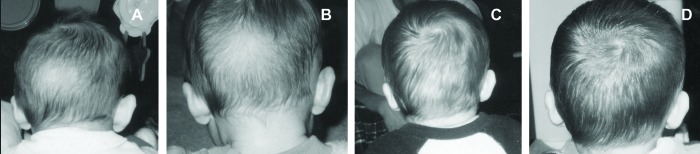
Case 2: A Before intervention; B One month following intervention; C Two months following intervention; D Three months following intervention
DISCUSSION:
We first became interested in the concept of nonsurgical treatment of congenital ear abnormalities in 1994. The plastic surgeon (JWT) at our Level 2 (secondary) Perinatal Center indicated to the pediatric group that there may be alternatives to surgical correction for a wide range of congenital ear deformities (1,2). After reviewing the literature, we began to use dental wax and Hypafix tape in the newborn period to correct deformities such as lop, cup, Stahls and protruding ears. We recognized that a number of abnormalities corrected spontaneously (61% auricular deformity overall at birth and 38% remained at one year), but were unable to determine with certainty which group would improve (4,5) Taping and other modalities have been used as both initial therapy and in conjunction with surgery (6–8). There are significant potential complications associated with external ear surgery (9).
We were impressed over the next eight years that this simple intervention in the newborn period seemed to make a significant difference to the outcome (as expressed by family members) after only three weeks of taping. We are presently engaged in a research trial to document these findings. The pediatric literature supports this approach (10,11–14). After further review of the literature, we have extended our treatment age over the past five years to children beyond the newborn period (3,15). Although the literature indicates success up to 14 years of age, we have found that children do not tolerate the taping or splinting (dental wax or OTO-FORM-K/c, Dreve-Otoplastik GmbH, Germany) after age three years, and our drop out rate is very high in the older age group. We are impressed, however, at the desire families have to correct these deformities and are intrigued by literature reports (16). We also recognize that ear abnormalities are a significant cosmetic concern to children and have resulted in an impressive catalogue of derogatory names used to describe these conditions (17). The two cases presented are representative of the results of this technique. The clinical improvement is especially significant in that protruding ears tend to worsen during the first year (0.4% at birth, 4.4% at one month and 5.5% at one year) (2,4). Both sets of parents rated the improvement as excellent (3). We present these case reports as examples of an effective, user friendly and safe office procedure for the treatment of a congenital ear abnormality (protruding ears).
REFERENCES
- 1.Matsuo K, Hirose T, Tomono T, et al. Nonsurgical correction of congenital auricular deformities in early neonate: A preliminary report. Plast Reconstr Surg. 1984;73:38. doi: 10.1097/00006534-198401000-00009. [DOI] [PubMed] [Google Scholar]
- 2.Matsuo K, Hayashi R, Kiyan M. Nonsurgical correction of congenital auricular deformities. Clin Plast Surg. 1990;17:383–95. [PubMed] [Google Scholar]
- 3.Yotsuyanagi T, Yokoi K, Urushidate S. Nonsurgical correction of congenital auricular deformities in children older than early neonates. Plast Reconstr Surg. 1998;101:907. doi: 10.1097/00006534-199804040-00004. [DOI] [PubMed] [Google Scholar]
- 4.Hirose T, Satoh R, Matsuo K, et al. Studies on the shape of the auricle-changes of the shape of the auricle after birth. In: Maneksha RJ, editor. Transactions of the 9th International Congress of Plastic and Reconstructive Surgery. New Delhi, India: Tata McGraw Hill; 1983. [Google Scholar]
- 5.Tan ST, Gault DT. When do ears become prominent? Br J Plast Surg. 1994;47:573–4. doi: 10.1016/0007-1226(94)90143-0. [DOI] [PubMed] [Google Scholar]
- 6.Ohmori S, Matsumoto K. Treatment of cryptotia, using Teflon string. Plast Reconstr Surg. 1972;49:1. doi: 10.1097/00006534-197201000-00006. [DOI] [PubMed] [Google Scholar]
- 7.Muraoka M, Nakai Y, Sasaki T, et al. Tape attachment therapy for correction of congenital malformations of the auricle: Clinical and experimental studies. Laryngoscope. 1985;95:167–76. doi: 10.1288/00005537-198502000-00008. [DOI] [PubMed] [Google Scholar]
- 8.Hirose T, Tomono T, Matsuo K, et al. Cryptotia: Our classification and treatment. Br J Plast Surg. 1985;38:352–60. doi: 10.1016/0007-1226(85)90241-3. [DOI] [PubMed] [Google Scholar]
- 9.Furnas D. Complications of surgery of the external ear. Clin Plast Surg. 1990;17:305–79. [PubMed] [Google Scholar]
- 10.Spinelli H. Congenital ear deformities. Pediatr Rev. 1993;14:473–4. [PubMed] [Google Scholar]
- 11.Furnas D. Nonsurgical treatment of auricular deformities in neonates and infants. Pediatr Ann. 1999;28:6. doi: 10.3928/0090-4481-19990601-10. [DOI] [PubMed] [Google Scholar]
- 12.Tan S, Abramson D, MacDonald D, et al. Molding therapy for infants with deformational auricular anomalies. Ann Plast Surg. 1997;38:263–8. doi: 10.1097/00000637-199703000-00013. [DOI] [PubMed] [Google Scholar]
- 13.Merlob P, Eshel Y, Mor N. Splinting therapy for congenital auricular deformities with the use of soft material. J Perinatol. 1995;15:293–6. [PubMed] [Google Scholar]
- 14.Brown FE, Colon LB, Addante RR, et al. Correction of congenital auricular deformities by splinting in the neonatal period. Pediatrics. 1986;78:406–11. [PubMed] [Google Scholar]
- 15.Tan S, Shibu M, Gault D. A splint for correction of congenital ear deformities. Br J Plast Surg. 1994;47:575–8. doi: 10.1016/0007-1226(94)90144-9. [DOI] [PubMed] [Google Scholar]
- 16.Perez-Barrero P, Rodrigo J, Marques M, et al. Auto-otoplasty using cyanoacrylate. Plast Reconstr Surg. 2001;108:7. doi: 10.1097/00006534-200112000-00062. [DOI] [PubMed] [Google Scholar]
- 17.Rogers B. Microptic, lop, cup and protruding ears (four directly inheritable deformities?) Plast Reconstr Surg. 1968;41:208–31. doi: 10.1097/00006534-196803000-00003. [DOI] [PubMed] [Google Scholar]