

Abstract
Background
Non-adherence to anti tuberculosis treatment is one of the crucial challenges in improving tuberculosis cure-rates and reducing further healthcare costs. The poor adherence to anti-tuberculosis treatment among patients with tuberculosis is a major problem in Ethiopia. Hence, this study assessed level of non-adherence to anti-tuberculosis therapy and associated factors among patients with tuberculosis in northwest Ethiopia.
Methods
An institution based cross-sectional survey was conducted among tuberculosis patients who were following anti-tuberculosis treatment in North Gondar zone from February 20 – March 30, 2013. Data were collected by trained data collectors using a structured and pre-tested questionnaire. Data were entered to EPI INFO version 3.5.3 and analyzed using statistical package for social sciences (SPSS) version 20. Multiple logistic regressions were fitted to identify associations and to control potential confounding variables. Odds ratio (OR) with 95% confidence interval was calculated and p-values<0.05 were considered statistically significant.
Results
A total of 280 tuberculosis patients were interviewed; 55.7% were males and nearly three quarters (72.5%) were urban dwellers. The overall non-adherence for the last one month and the last four days before the survey were 10% and 13.6% respectively. Non-adherence was high if the patients had forgetfulness (AOR 7.04, 95% CI 1.40–35.13), is on the continuation phase of chemotherapy (AOR: 6.95, 95% CI 1.81–26.73), had symptoms of tuberculosis during the interview (AOR: 4.29, 95% CI 1.53–12.03), and had co-infection with HIV (AOR: 4.06, 95% CI 1.70–9.70).
Conclusions
Non-adherence to anti-tuberculosis treatment was high. Forgetfulness, being in the continuation phases of chemotherapy, having symptoms of tuberculosis during the interview, and co-infected with HIV were significantly associated with non-adherence to anti-tuberculosis therapy. Special attention on adherence counseling should be given to symptomatic patients, TB/HIV co-infected patients, and those in the continuation phase of the tuberculosis therapy.
Introduction
Tuberculosis (TB), one of the oldest diseases known to affect humans, is a major cause of death worldwide. It usually affects the lungs, although other organs are involved in up to one-third of the cases. If left untreated, 50–65% of TB cases will die within 5 years [1]. In 2010, there were 8.8 million new cases of TB and 1.45 million deaths from TB worldwide. The human immunodeficiency virus (HIV) pandemic presents a significant challenge to global TB control. TB is the second leading cause of death from an infectious disease worldwide among all people and the leading preventable cause of death among people living with HIV. About 13% of TB cases occur among people living with HIV [2], [3].
According to recent estimates, Ethiopia stands 7th in the list of high TB burden countries. In Ethiopia, TB is the leading cause of morbidity, the third cause of hospital admission, and the second cause of death. The estimated TB incidence in Ethiopia was 261/ 100,000 inhabitants in 2011. The lifetime risk of developing TB in Ethiopia is estimated to be 50–60% for HIV-infected people, only 10% for HIV-negative counterparts [3], [4].
Poor adherence to treatment of chronic diseases including TB is a worldwide problem of striking magnitude [5]. However, patients with TB are expected to have adherence levels greater than 90% in order to facilitate cure [6], [7]. The failure for cure increases the risk of development of drug resistant strains and further spread of TB in the community, which in turn increases morbidity and mortality. Adherence to TB treatment is crucial to achieve cure and avoid emergence of drug resistance [7]. In sub Saharan Africa, there is high rate of losses to follow up of TB patients that ranged from 11.3% to 29.6% [8]. Ethiopia is one of the seven countries that reported lower rates of treatment success (84%) [3]. Patients who take their TB treatment in an irregular and unreliable way are at greatly increased risk of treatment failure, relapse and the development of drug-resistant TB strains. Furthermore, the emergence and spread of multi drug resistant (MDR) and extensive drug resistant (XDR) TB further reinforces the absolute necessity of helping TB patients to not miss any doses of anti TB [9], [10]. However, it is very difficult to have regular supervision and support of TB patients in developing countries like Ethiopia. Hence, this study assessed the level of non-adherence to anti-TB therapy and associated factors among TB patients in northwest Ethiopia.
Methods
Study Setting
The study was conducted in the North Gondar zone, northwest Ethiopia. The zone has 22 districts with a total population of 2,921,470. All health facilities providing anti-TB services in three major towns of north Gondar (Gondar, Metema and Debark) were included. Newly diagnosed TB patients receive six months of standard TB chemotherapy in two phases- an intensive phase for two months and a continuation phase of four months. A fixed dose combination of RHZE (Rifampicin, Isoniazid, Pirazinamide and Ethambutol) is given in the intensive phase of anti-TB therapy while only RH during the continuation phase. Patients collect anti-TB drugs daily during the intensive phase except weekends while weekly or monthly during the continuation phase. Provider initiated voluntary counseling and testing for HIV infection was also offered currently to all TB patients.
Study Design and Participants
An institution based cross-sectional survey was conducted from February 20 – March 30, 2013. Eligible patients were new TB patients aged at least 15 years regardless of the site or the smear status of their TB. To be eligible for this study, patients must have also taken anti-TB at least for a month.
Sample Size and Sampling Procedures
The sample size was calculated using a single population proportion formula; considering 21% proportion of non- adherence level according to previous similar study from southwest Ethiopia (16), a 5% margin of error, and 10% possible non-response rate. The sample size was estimated to be 281. All adult TB patients (≥15 years old) on anti-TB at tuberculosis follow up clinics in the three (Gondar, Metema and Dabark) towns within the study period were interviewed.
Data Collection and Assessment of Non - adherence
Data were collected using an interviewer-administered questionnaire. The questionnaire was composed of socio-demographic characteristics, patient related; therapy or drug related information, social and health system /health provider related variables and pre-tested before the actual data collection. Data were collected after verbal informed consent was obtained. Six nurses who were trained for this purpose collected the data. Data collectors were also not part of the health facilities where TB patients interviewed.
Recent non- adherence (last 4 days) and non-adherence during the last one month before the survey were assessed. Patients were asked to report the total number of anti-TB pills they missed 4 days before the survey. These numbers of pills were compared to the number of pills prescribed to the patient. Adherence to TB medication in the last 4 days was classified as non-adherent (missed at least 1 (25%) of the pills prescribed over 4 days) and completely adherent (no missed pill in the last 4 days before the survey). Similarly, the last one month non-adherence was calculated as total reported missed pills over the total prescribed pills within that month and classified as adherent (no more than 10% of pills missed) and otherwise non- adherent. Patients were also asked to report why they missed anti-TB drugs. A patient who scores three or more than three from a six item questions asked to measure TB knowledge were considered to have good knowledge about TB. These questions were obtained from information routinely provided to patients as part of the national TB program.
Data Analysis
Data were entered to EPI INFO version 3.5.3 and analysis was conducted using statistical package for social sciences (SPSS) version 20. Descriptive statistics like frequencies and cross tabulation were made for most selected variables. Multiple logistic regression analysis was used to assess the association between the dependent variable and each independent variable. Variables with p-values ≤0.2 in bivariate analysis were fitted in the final multiple logistic regression model to assess the strength of association and control confounding effects. Both Crude Odds Ratio (COR) and Adjusted Odds Ratio (AOR) with 95% confidence interval (CI) were used to show an association between selected variables. Variables having p-value ≤0.05 in the final model were taken as significant determinants.
Ethical Considerations
The ethical clearance was obtained from the Institutional Review Board of the University of Gondar. The Institutional Review Board approved the oral informed consent since it was anticipated that many of the study subjects could not read and write. In addition to this, the Institutional Review Board approved all ethical procedures, based on the awareness about the type of study (that it was harmless to study subjects) and the education level of study subjects. An official permission letter was obtained from each health facility administration office. During data collection, oral informed consent was obtained from all participants after they were introduced to the purpose of the study and informed about their rights to interrupt the interview at any time. To ensure confidentiality, names were avoided in the questionnaire and reporting the results of the study. In addition, the collected information was locked with a key (hard copies) and by passwords (soft copies). Informed oral consent was also obtained from parents or guardians for subjects under 18 years old.
Results
Socio-demographic Characteristics
A total of 280 TB patients (with a response rate of 99.6%) were interviewed. Nearly three quarters (72.5%) were urban dwellers and had a mean age of 32.9 (±14.8 SD) years. About half of them (50.4%) did not attend any formal education and nearly one fifth of them were farmers. Amhara (98.2%) and Orthodox Christianity (89.6%) were the most common ethnicity and religion respectively (Table 1).
Table 1. Socio-demographic characteristics of respondents’, North Gondar zone, Northwest Ethiopia, May 2013 (n = 280).
| Characteristics | Frequency | Percent | |
| Residence | Urban | 203 | 72.5 |
| Rural | 77 | 27.5 | |
| Sex | Male | 156 | 55.7 |
| Female | 124 | 44.3 | |
| Age (years) | ≤32 | 171 | 61.1 |
| >32 | 109 | 38.9 | |
| Marital status | Single | 121 | 43.2 |
| Married | 118 | 42.1 | |
| Divorced | 31 | 11.1 | |
| Widowed | 10 | 3.6 | |
| Education level | No formal education | 141 | 50.4 |
| Primary level | 85 | 30.4 | |
| Secondary level &above | 54 | 19.3 | |
| Occupation | Farmer | 58 | 20.7 |
| Merchant | 48 | 17.1 | |
| Daily laborer | 43 | 15.4 | |
| Housewife | 48 | 17.1 | |
| Students | 39 | 13.9 | |
| Government employee | 17 | 6.1 | |
| Jobless | 19 | 6.8 | |
| Others | 8 | 2.9 | |
| Religion | Orthodox | 251 | 89.6 |
| Muslim | 29 | 10.4 | |
| Ethnicity | Amhara | 275 | 98.2 |
| Tigrie | 5 | 1.8 | |
Non-adherence to Anti-TB Treatment and Reasons of Pill Missing
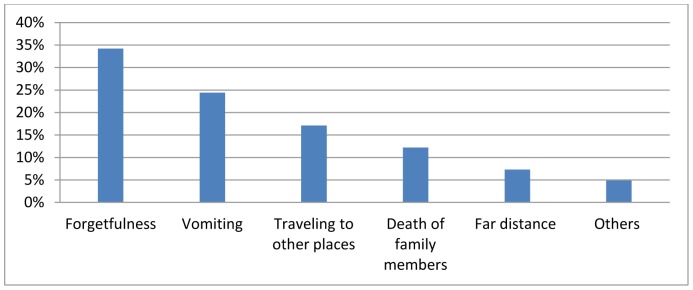
The overall calculated non-adherence over one month and the last four days before the survey were 10% and 13.6% respectively. Forgetfulness (34%), vomiting (24%) and traveling to other places (17%) were the most frequent reasons for missing the anti-TB pills (Figure 1).
Figure 1. Reasons of anti-TB pills missing, North Gondar zone, Northwest Ethiopia, May 2013.
Patient Related Characteristics
About 6% of TB patients reported that they had a problem of forgetfulness. Almost all (98.9%) participants had good knowledge about TB but 3.6% of participants reported they had stopped taking their medication without telling their health care provider because they felt worse when they took it. Similarly, 3.6% of participants reported that they stopped taking their anti-TB medication when they felt better. About 6% of participants were substance users.
Healthcare System and Other Related Characteristics
Ninety five percent of TB patients walked to and from the health facilities and 26.8% of participants reported that it took them more than half an hour to reach the nearby health facility providing them the anti-TB drugs. Nearly half of participants (54.3%) reported that the health workers were very friendly to them.
Most of TB patients (97.1%) in the current study disclosed their illness to their relatives and most (75%) of those who had not disclosed were due to fear of stigma. The rest had no relatives with whom to share their problem. About one in eight (12.9%) participants visited quacks (i.e. Traditional healers) while they were taking their chemotherapy (Table 2).
Table 2. Healthcare system and other related characteristics of respondents’, North Gondar zone, Northwest Ethiopia, May 2013.
| Characteristics | Frequency | Percent | |
| Time to reach to the health facility | ≤30 minutes | 205 | 73.2 |
| >30 minutes | 75 | 26.8 | |
| Transportation | On foot | 266 | 95 |
| Public transport | 14 | 5.0 | |
| Waiting time in the health facilities | ≤30 minutes | 269 | 96.1 |
| >30 minutes | 11 | 3.9 | |
| Availability of drugs | Always available | 278 | 99.3 |
| Not always available | 2 | 0.7 | |
| Counseling | Yes | 204 | 72.9 |
| No | 76 | 27.1 | |
| Relationship with health workers | Very friendly | 152 | 54.3 |
| Friendly | 126 | 45.0 | |
| Unfriendly | 2 | 0.7 | |
| TB status disclosure to the family | Yes | 272 | 97.1 |
| No | 8 | 2.9 | |
| Treatment supporter | Health facility worker | 166 | 59.3 |
| Health extension worker | 4 | 1.4 | |
| A family member | 182 | 65 | |
| Religious leaders | 10 | 3.6 | |
| No treatment supporter | 22 | 7.9 | |
| Visited quacks | Yes | 36 | 12.9 |
| No | 244 | 87.1 |
Quacks are ‘Traditional healers’.
TB Disease and Treatment Related Characteristics
A significant proportion of TB patients (38.9%) reported some kind of anti-TB medication adverse effects. Three quarters (75.2%) and 37% of participants complained of minor adverse effects such as urine discolorations and headache or dizziness, respectively. Most patients (87.5%) were naive for anti-TB medication. Almost all (97.5%) of the TB patients were screened for HIV and nearly one quarter (23.4%) of them were positive (Table 3).
Table 3. Anti-TB therapy and diseases related characteristics of TB patients, North Gondar zone, Northwest Ethiopia, May 2013.
| Characteristics | Frequency | Percent | |
| Experience of side effects | Yes | 109 | 38.9 |
| No | 171 | 61.1 | |
| Types of side effects (n = 109) | Skin rash | 17 | 15.6 |
| Headache & dizziness | 42 | 36.7 | |
| Yellow eyes | 13 | 11.9 | |
| Vomiting | 32 | 29.4 | |
| Urine discoloration | 82 | 75.2 | |
| Symptoms of TB during the interview | Yes | 36 | 12.9 |
| No | 244 | 87.1 | |
| Treatment category | New | 245 | 87.5 |
| Re-treatment | 35 | 12.5 | |
| Types of TB | PTB-SM+ | 116 | 41.4 |
| PTB-SM− | 97 | 34.7 | |
| EPTB | 67 | 23.9 | |
| HIV screening status | Screened | 273 | 97.5 |
| Not screened | 7 | 2.5 | |
| HIV status (n = 273) | Positive | 64 | 23.4 |
| Negative | 209 | 76.6 | |
| ART status (n = 64) | Started | 44 | 68.8 |
| Not started | 20 | 31.2 | |
| OIs other than TB (n = 64) | Yes | 17 | 26.6 |
| No | 47 | 73.4 | |
| Drugs other than anti-TB & HAART (n) | None | 221 | 93.6 |
| CPT | 15 | 6.4 | |
| Phases of chemotherapy | Intensive phase | 86 | 30.7 |
| Continuation phase | 194 | 69.3 |
CPT = cotrimoxazole preventive therapy, EPTB = Extra pulmonary TB, PTB-SM+ = Smear positive pulmonary TB, PTB-SM− = Smear negative pulmonary TB, OI = Opportunistic Infections.
Factors Associated with Non-adherence to Anti-TB Treatment
In the bivariate analysis, forgetfulness, phases of chemotherapy, symptoms of TB during the interview, HIV co-infection, experience of drug side-effects, visiting quacks, and taking additional drugs other than anti-TB were significantly associated with anti-TB treatment non-adherence.
However, in the adjusted analysis, forgetfulness, phases of chemotherapy, symptoms of TB during the interview and HIV co-infection were remained significantly and independently associated with anti-TB medication non-adherence. Those patients who had a problem of forgetfulness were seven times more likely to be non-adherent than their counterparts (AOR: 7.04, 95% CI 1.40–35.13). TB patients who were in the continuation phases of chemotherapy were seven times (AOR: 6.95, 95% CI 1.81–26.73) more likely to be non-adherent to anti-TB medications. In addition to this, patients who had symptoms of TB during the interview (AOR: 4.29, 95% CI 1.53–12.03) and had co-infection with HIV (AOR: 4.06, 95% CI 1.70–9.70) were also at higher risk of non-adherence than those who were non-symptomatic during the interview and HIV sero-negatives respectively (Table 4).
Table 4. Logistic regression analysis of factors associated with non- adherence to anti-TB (last 1 month).
| Characteristics | Non-adherence | Crude OR | Adjusted OR | ||
| Yes | no | (95% CI) | (95% CI) | ||
| Forgetfulness | Yes | 4 | 7 | 5.83(1.59–21.36) | 7.04(1.40–35.13) |
| No | 24 | 245 | 1.00 | 1.00 | |
| Phases of Chemotherapy | Intensive phase | 3 | 87 | 1.00 | 1.00 |
| Continuation phase | 25 | 165 | 4.39(1.29–14.96) | 6.95(1.81–26.73) | |
| Symptoms of TB during the interview | Yes | 9 | 27 | 3.95(1.62–9.59) | 4.29(1.53–12.03) |
| No | 19 | 225 | 1.00 | 1.00 | |
| Visited quacks | Yes | 7 | 29 | 2.56(1.01–6.55) | |
| No | 21 | 223 | 1.00 | ||
| Experience side effects | Yes | 17 | 92 | 2.69(1.21–5.99) | |
| No | 11 | 160 | 1.00 | ||
| Co- infection with HIV | Yes | 14 | 50 | 3.90(1.75–8.71) | 4.06(1.70–9.70) |
| No | 14 | 195 | 1.00 | 1.00 | |
| Additional drugs | Yes | 9 | 38 | 2.67(1.12–6.34) | |
| No | 19 | 214 | 1.00 | ||
North Gondar zone, Northwest Ethiopia, May 2013.
Discussion
Adherence to anti-TB treatment is a major determinant of treatment outcome. In developing countries where inequities in access to health care are high and health resources are scarce the magnitude and impact of poor adherence is assumed to be higher. It is undeniable that many patients experience difficulties in following treatment recommendations [5], [11]. Hence, this study assessed the level and determinant factors of non-adherence to anti-TB medications.
Though a self-reported level of non-adherence is assumed to be under-estimated, a high proportion (10%) of non-adherence in the last one month before the survey was found in this study. Similarly, a higher proportion of non-adherence (13.6%) in the four days prior to the survey was reported. This finding is more than twice that reported from Kenya (4.8%).
However, the present non-adherence over one month was lower than the previous reports from Southern Ethiopia (20.8%), Uganda (25%), Kolkata, India (40.5%), and the Jiangsu Province of China (12.2%) [12]–[15]. This is probably due to variations in study populations. In this study we included both HIV-positive and HIV-negative patients. The former studies included only TB-HIV co-infected patients. HIV co-infected patients are much more likely to be non-adherent for several reasons. On the other hand, this variation may be attributable to the duration in which the adherence was calculated. In the case of the Ugandan study, adherence was estimated over the last five days and it was over the whole intensive phase in the case of Kolkata India.
In the adjusted analysis; forgetfulness, being in continuation phases of chemotherapy, having symptoms of TB during the interview, and HIV co-infection were significantly associated with anti-TB medication non-adherence. Those TB patients who were in the continuation phase of the chemotherapy were about seven times more likely to be non-adherent than those who were in the intensive/directly observed treatment short-course strategy (DOTS). However, it is believed that DOTS with daily supervision is a difficult task for most patients and in particular HIV co-infected patients who needed to attend the clinics for ART. It is also believed that DOTS is too rigid a strategy [16]. Similar findings were also reported from Southern Ethiopia, Brazil, and Uganda, [13], [17], [18].
TB patients who were symptomatic during the interview were much more likely to be non-adherent than those who did not have symptoms of TB during the interview. Under normal circumstances patients whose TB symptoms were resolved quickly may be urged to leave treatment once they started feeling better. However, in this study the opposite was true. Patients may remain symptomatic as a result of their poor adherence. On the other hand, patients who remain symptomatic while sticking to treatment may be disappointed and intentionally miss their pills. However, a study conducted in Kolkata, India declared that the urge to leave treatment once patient started feeling better was a significant determinant of non-adherence to anti-TB medication [14].
The proportion of HIV co-infection among TB patients was 23.4%. About 69% of these patients were on ART. In this study, HIV co-infected TB patients were less likely to be adherent to their anti-TB medications. HIV/AIDS co-infected patients have many pills to take and the adverse effects of anti-TB medication are more common for HIV co-infected patients [7]. Similarly, HIV/AIDS co-infected patients may be less motivated to take their medication. This phenomenon has been reported in Brazil, Kenya and South Africa [18]–[20].
As previously reported from other studies [12], [21], forgetfulness was also an important problem associated with poor adherence to anti-TB. This problem may be related to older age, as older age was significantly associated with non- adherence over the last four days. This might be also explained by HIV/AIDS related encephalopathy or dementia.
However, previously confirmed factors like distance from a health facility, transportation cost, relationship with health worker, and proper counseling were not associated with non-adherence in this study. Currently, in Ethiopia, TB treatment is being provided freely at the community, grass root level. However, some patients still questioned the accessibility of TB related services. Furthermore, most TB patients had good relationship with their health care provider (99.3%). In general adherence is a dynamic issue and barriers are also liable to change over time, which necessitates continuation of multi-disciplinary collaborative researches. Finally, this study shares the limitations of cross-sectional studies and hence it might suffer from temporal relationship establishment with some variables and might not provide much stronger evidence of causality. In addition to this, this study only addressed a self-reported level of non-adherence and it might be under-estimated.
Conclusions
Non-adherence among TB patients was high. Forgetfulness, being in continuation phases of chemotherapy, having symptoms of TB during the interview, and HIV co-infection were significantly associated with anti-TB medication non-adherence. Thus, special attention and adherence counseling should be given for those who remained symptomatic, those who are co-infected with HIV, and those in the continuation phase of the chemotherapy. Further research is also recommended since the issue of adherence is dynamic.
Acknowledgments
The authors are indebted to the Research and Community Service Vice President’s Office of the University of Gondar and all study participants deserve appreciation for their cooperation.
Funding Statement
This research article was funded by Research and Community Service Vice President office of the University of Gondar. The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
References
- 1.Fauci A, Kasper D, Braunwald E (2008) Tuberculosis Harrison’s principle of internal medicine 17th ed. United States of America: The McGraw-Hill Companies.
- 2.Organization WH (2012) WHO policy on collaborative TB/HIV activities Guidelines for national programmes and other stakeholders. Geneva, Switzerland. 36 p. [PubMed] [Google Scholar]
- 3.Organisation WH (2011) WHO Report 2011 | Global Tuberculosis Control. France WHO. 258 p. [Google Scholar]
- 4.Ethiopia FMoH (2008) Tuberculosis, Leprosy and TB/HIV Prevention and Control Programme. Addis Ababa, Ethiopia 207 p. [Google Scholar]
- 5.Sabate E (2003) Adhernece to long-term therapies: Evidence for action. Geneva, Switzerland: WHO.
- 6.Harries A, Maher D, Graham S (2004) TB/HIV:A CLINICAL MANUAL. Genva World Health Organization 212 p. [Google Scholar]
- 7.Awofeso N (2008) Antituberculous medication side-effects constitute major factor for poor adherence to tuberculosis treatment. Bulletin of WHO 86. [DOI] [PMC free article] [PubMed]
- 8. Castelnuovo B (2010) A review of compliance to anti tuberculosis treatment and risk factors for defaulting treatment in Sub Saharan Africa. Afr Health Sci 10: 320–324. [PMC free article] [PubMed] [Google Scholar]
- 9.Organization WH (2010) Antiretroviral therapy for HIV infection in adults and adolescents recommendations for a public health approach. Geneva Siwzerland WHO. [PubMed]
- 10. de Steenwinkel JE, ten Kate MT, de Knegt GJ, Verbrugh HA, Aarnoutse RE, et al. (2012) Consequences of noncompliance for therapy efficacy and emergence of resistance in murine tuberculosis caused by the Beijing genotype of Mycobacterium tuberculosis. Antimicrob Agents Chemother 56: 4937–4944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Rocha M, Pereira S, Ferreira L, Barros H (2003) The role of adherence in tuberculosis HIV-positive patients treated in ambulatory regimen. Eur Respir J 21: 785–788. [DOI] [PubMed] [Google Scholar]
- 12. Kebede A, Wabe NT (2012) Medication adherence and its determinants among patients on concomitant tuberculosis and antiretroviral therapy in South west ethiopia. N Am J Med Sci 4: 67–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Amuha MG, Kutyabami P, Kitutu FE, Odoi-Adome R, Kalyango JN (2009) Non-adherence to anti-TB drugs among TB/HIV co-infected patients in Mbarara Hospital Uganda: prevalence and associated factors. Afr Health Sci 9 Suppl 1S8–15. [PMC free article] [PubMed] [Google Scholar]
- 14. Sardar P, Jha A, Roy D, Roy S, Guha P, et al. (2010) Intensive phase non-compliance to anti tubercular treatment in patients with HIV-TB coinfection: a hospital-based cross-sectional study. J Community Health 35: 471–478. [DOI] [PubMed] [Google Scholar]
- 15. Weiguo X, Wei L, Zhou Y, Zhu L, Shen H, et al. (2009) Adherence to anti-tuberculosis treatment among pulmonary tuberculosis patients: a qualitative and quantitative study. BMC Health Services Research 9: 1472–6963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Gebremariam MK, Bjune GA, Frich JC (2010) Barriers and facilitators of adherence to TB treatment in patients on concomitant TB and HIV treatment: a qualitative study. BMC Public Health 10: 651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Shargie EB, Lindtjorn B (2007) Determinants of treatment adherence among smear-positive pulmonary tuberculosis patients in Southern Ethiopia. PLoS Med 4: e37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Garrido Mda S, Penna ML, Perez-Porcuna TM, de Souza AB, Marreiro Lda S, et al. (2012) Factors associated with tuberculosis treatment default in an endemic area of the brazilian Amazon: a case control-study. PLoS One 7: e39134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Muture BN, Keraka MN, Kimuu PK, Kabiru EW, Ombeka VO, et al. (2011) Factors associated with default from treatment among tuberculosis patients in Nairobi province, Kenya: a case control study. BMC Public Health 11: 696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Govender S, Mash R (2009) What are the reasons for patients not adhering to their anti-TB treatment in a South African district hospital? SA Fam Pract 51: 512–516. [Google Scholar]
- 21. Abula T, Worku A (2001) patient non compliance with drug regimens for chronic diseaes in northweat Ethiopia. EthiopJHealth Dev 15: 185–192. [Google Scholar]