

Abstract
Objective
To determine the relationship between whole body vibration (WBV) induced helicopter flights and degenerative changes of the cervical and lumbar spine.
Methods
We examined 186 helicopter pilots who were exposed to WBV and 94 military clerical workers at a military hospital. Questionnaires and interviews were completed for 164 of the 186 pilots (response rate, 88.2%) and 88 of the 94 clerical workers (response rate, 93.6%). Radiographic examinations of the cervical and the lumbar spines were performed after obtaining informed consent in both groups. Degenerative changes of the cervical and lumbar spines were determined using four radiographs per subject, and diagnosed by two independent, blinded radiologists.
Results
There was no significant difference in general and work-related characteristics except for flight hours and frequency between helicopter pilots and clerical workers. Degenerative changes in the cervical spine were significantly more prevalent in the helicopter pilots compared with control group. In the cervical spine multivariate model, accumulated flight hours (per 100 hours) was associated with degenerative changes. And in the lumbar spine multivariate model, accumulated flight hours (per 100 hours) and age were associated with degenerative changes.
Conclusion
Accumulated flight hours were associated with degenerative changes of the cervical and lumbar spines in helicopter pilots.
Keywords: Vibration, Spine, Degenerative changes, Aircraft
INTRODUCTION
Transportation systems such as airplanes, trains, sea vessels, and cars induce whole body vibrations (WBV) that affect pilots and passengers. WBV refers to the transfer of low-frequency vibrations to the whole body from the body contact area, such as the seat of a truck, tractor, bus or other vehicle, or the floor of a workplace. Prolonged exposure to WBV causes physiological effects and is associated with musculoskeletal disorders and diseases of the nervous, digestive, and circulatory systems [1-5].
In musculoskeletal disorders, the incidence of low back pain, degenerative osteoarthritis, disc changes, and herniated nucleus pulposus in spines are higher in employees with job categories involving WBV exposure than in those without WBV exposure [6-8].
Helicopter pilots are exposed to higher WBV levels than fixed-wing aircraft pilots [9]. Helicopters are increasingly used for firefighting, rescue, sightseeing tours, and military operations. Recent studies have observed lower back and neck pain in helicopter pilots [10-14].
Causes include occupational conditions, such as long work duration, flight time, flight accelerations, WBV, helmets and headgear, and awkward postures during the flight, as well as general conditions, such as age, being overweight, smoking, and drinking [15-17].
Some studies have shown that fixed-wing aircraft pilots and helicopter pilots have more degenerative changes in the cervical and lumbar spines than non-flying controls [18,19], but other studies have reported no relationships between musculoskeletal disorders suffered by pilots and job-related factors, especially regarding WBV [20,21]. There is currently insufficient evidence to indicate an exposure-response relationship between exposure to seated WBV and lower back disorders [22,23]. This study was carried out to examine the relationship between helicopter flight and degenerative changes in the cervical and lumbar spines.
MATERIALS AND METHODS
Subjects
We examined 186 military helicopter pilots who had undergone annual pilot physical examinations at a military hospital and 94 military clerical workers who had also received annual general physical examinations. The helicopter pilots were exposed to WBV, and 0.76 m/s2 was the mean overall level of exposure to WBV per pilot according to the ISO 2631-1 method of International Organization for Standardization [24].
The helicopter pilots examined in this study regularly wore standard flight helmets of Korea Air Force during the day. During night operations they may also have had night vision goggles attached to their helmets. Pilots fly 12 hours per week during the daytime and three hours per week during the nighttime.
Unlike helicopter pilots, clerical workers are not exposed to WBV. The military clerical workers examined in this study otherwise worked in the same workplaces as the exposed group and there were few differences in the office working conditions between the two groups. Considering the similarity of the working conditions in both groups, except for exposure to WBV, and in order to reduce the bias due to the healthy worker effect, we decided to use military clerical workers as a control group. The clerical workers each worked eight hours per day typing and correcting official documents using computers.
Questionnaire
Basic demographic variables and past disease histories of the subjects were surveyed using written questionnaires and interviews that were given during the medical examinations. Among the survey subjects, all who commuted long distances by car, were exposed to WBV while enjoying hobbies like motorcycle riding, mountain terrain bicycle riding, off road driving or had suffered any injury or disease that could trigger musculoskeletal diseases like ligament injury of knee and ankle joint, spondylolisthesis or scoliosis, were excluded. Questionnaires and interviews were completed for 164 of the 186 helicopter pilots (response rate, 88.2%) and 88 of the 94 clerical workers (response rate, 93.6%).
The questionnaire consisted of items relating to general and work-related characteristics. Information was obtained regarding age, height, weight, smoking, alcohol consumption (any alcoholic beverages more than once a week or less than once a week), and exercise (exercise more than three times per week for more than 1 hour each time, or not). Participant body mass indexes (BMI) were categorized as normal (<23 kg/m2), overweight (≥23, <25 kg/m2), or obese (≥25 kg/m2) according to the Korean Society for the Study of Obesity standards for Koreans [25]. Questions concerning work-related characteristics included length of service, accumulated flight hours, and average flight hours per day.
Radiographic examinations
Since radiographic examinations of the cervical and the lumbar spines were not included in the annual health examinations of either the helicopter pilots or the clerical workers, radiographic examinations of the cervical and the lumber spines were performed after obtaining informed consent from the study subjects. Four views of the cervical and lumbar spines (anteroposterior, lateral, and both obliques) of each subject were obtained. All radiographs were independently reviewed by two radiologists. To reduce bias, the radiologists were given no information relating to the subjects' occupations. Degenerative changes of the lumbar spine were defined when there were severe disc height changes (<25% of adjacent discs), any osteophyte formation or any endplate sclerosis [26]. Degenerative changes of the cervical spines were defined when there were any abnormalities such as irregular odontoid processes, suggestions of narrowed foramina, hypertrophic or subluxated facets, lipping and/or narrowing of disk spaces, or any other osteophytic or ankylosis findings of the cervical spine [27]. Severe vertebral problems such as spondylolysis, spondylolisthesis, kyphosis, and scoliosis were excluded from the degenerative changes considered in this study.
Statistical analyses
To determine the significance of any differences between the exposed and control groups in general and work-related characteristics and radiologic findings, the chi-square test was used for discrete variables and Student t-test was used for continuous variables. To identify factors affecting degenerative changes in the cervical and lumbar spines of the two groups, a logistic regression analysis was used to obtain crude odds ratios. Flight hours, flight frequency, service length, and age were set as each variable because they are correlated with each other. Adjusted BMI, drinking, smoking, and exercise were set as common variables. Multivariate logistic regression analyses were also used to correct for the effects of age, length of service (<10 years, ≥10 years), flight hours, and flight frequency.
Accumulated flight hours were used for the statistical analysis because it was impossible to directly measure accumulated WBV. The accumulated flight hours and flight frequency were analyzed and expressed in units of 100 hours and 100 times, respectively. Statistical analyses were based on a significance level of 0.05.
RESULTS
The age of the pilots was younger than that of the control group. However, the average BMI of the pilots (mean±standard deviation [SD], 24.1±2.30 kg/m2) was significantly higher than that of the control group (mean±SD, 23.5±2.64 kg/m2; p<0.05). Conversely, there were more smokers in the control group (exposed group vs. control group, 51.2% vs. 77.3%; p<0.05). Most members of both groups exercised regularly, but the number of pilots who exercised regularly was slightly higher (exposed group vs. control group, 90.2% vs. 80.7%; p<0.05). There was no significant difference in drinking habits between the two groups (82.9% vs. 80.7%). The average length of service was longer in the control group. The pilots averaged 1,409.8 accumulated flight hours, with an average of 2.5 flight hours per day, and 824.4 times of cumulative flight frequency.
Degenerative changes in the cervical spine were significantly more prevalent in the pilots. The prevalence of lumbar spine degenerative changes was also a little higher in the pilots, but the difference was not significant (Table 1).
Table 1.
General and work-related characteristics and radiographic results for subjects
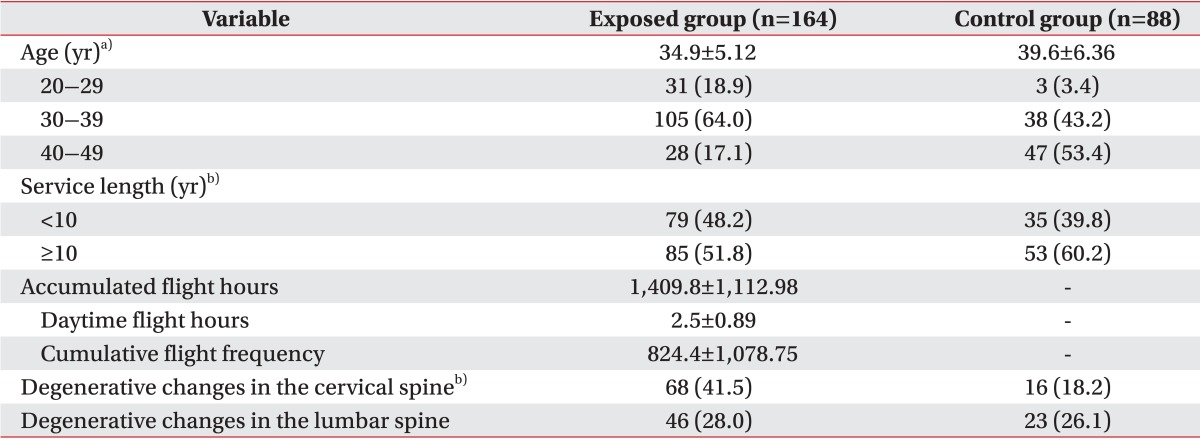
Values are presented as mean±standard deviation or number (%).
p<0.05 by a)Student t-test, b)chi-square test.
The univariate and multivariate logistic regression models for the associations between risk factors and degenerative changes in the cervical and lumbar spines are presented in Table 2. In the cervical spine multivariate model, accumulated flight hours (per 100 hours) was associated with degenerative changes. And in the lumbar spine multivariate model, accumulated flight hours (per 100 hours) and age were associated with degenerative changes (Table 2).
Table 2.
Odds ratio (OR) of degenerative changes in the spine (results of logistic regression analysis)

CI, confidence interval; Adjusted, adjusted by body mass index, smoking, drinking, and exercise.
a)Statistical significance at 95% CI.
DISCUSSION
Degenerative changes in the cervical and lumbar spines are related to age [18-20], gender, obesity, smoking, traumatic injury, and disease [2,6,20]. Degenerative changes do not necessarily lead to clinical symptoms such as pain or other functional limitations [28]. However, as observed in previous studies of the associations between lower back pain and WBV [10,11,17,20,29], severe degenerative changes may aggravate existing clinical symptoms and cause motion impairments.
In the present study, radiographs of the cervical and lumbar spines of subjects showed that degenerative changes in the cervical spine were significantly more frequent in subjects exposed to WBV, but that degenerative changes in the lumbar spine were not significantly different between the two groups. Interestingly, previous studies reported more degenerative changes in the lumbar spines of people exposed to WBV [10,20,29], which may indicate that helicopter pilots could also develop degenerative changes of the spine, especially in the lumbar discs, from continuous WBV exposure during flights [22,30,31]. Our findings may be confounded by the fact that the exposed group was younger, smoked less, and participated in more regular exercise than the control group.
However, differences in degenerative changes in the cervical spine between our two groups were observed. This is especially noteworthy, given that our results for lumbar spine degeneration were affected by differences in demographic variables. Indeed, firm conclusions have never been drawn about the relationship between exposure to seated WBV and neck disorders [32,33]. It seems likely that occupational factors that may have affected our results, such as helmet weight [15,18,34,35] and neck posture [36-38], were not sufficiently accounted for in the present study. Since our subjects regularly wear helmets and goggles, it is possible that, along with WBV, effects of the helmets and goggles on neck posture and weight were responsible for the degenerative changes in the necks of the helicopter pilots.
In our multivariable analysis, factors affecting degenerative changes in the cervical spine included accumulated flight hours, and factors affecting degenerative changes in the lumbar spine included accumulated flight hours and age. Among these factors, accumulated flight hours was influential in both cervical and lumbar spines degeneration. This finding is consistent with those of previous studies showing that accumulated flight hours was related to degenerative changes of the cervical [19] and lumbar spines [10,29]. Although age is an important factor in degenerative changes of the spine, there was no statistically significant relationship between age and degenerative changes of the cervical spine in this study. We thought the reason for this result is that subjects of this study were soldiers and therefore, were restricted in age.
This study was limited by its cross-sectional approach. The temporal order and causal relationships between variables were difficult to assess while evaluating past exposures. There were differences in covariates, such as age and BMI between the exposed group and the control group, although these factors were corrected for by statistical methods to avoid distortion of the results. We did not consider the weights of helmets or pilot posture, although these factors may have contributed to degenerative changes in the neck as much as WBV. However, other factors that may affect degenerative changes in the spine, such as WBV from non-occupational sources (sports or trauma, etc.) were excluded in the study design, to minimize their impact.
We did not use precise measurement techniques, such as magnetic resonance imaging, so it is possible that minute degenerative changes in our subjects were missed. Additionally, accumulated WBV was not measured directly, but by using the proxy of accumulated flight hours. Despite these limitations, in the multivariate analysis, we found that long flight times were related to degenerative changes of the neck and lumbar spine in helicopter pilots. Our findings should be further considered in future studies.
In this study, we found that WBV, along with other factors, is related to degenerative changes of the spine in helicopter pilots. Factors affecting degenerative changes in the cervical spine included accumulated flight hours, and factors affecting degenerative changes in the lumbar spine included accumulated flight hours and age. We confirmed that accumulated flight hours was influential in both cervical and lumbar spines degeneration.
To protect pilots, more studies of WBV along the x-, y-, and z-axis, the use of back and neck rests, and assessments of the effects of age, would be beneficial, as well as examinations of anthropometric data including the weight of ergonomic peripheral devices worn by pilots. Such studies would aid the implementation of preventive measures to safeguard helicopter pilots in the future.
ACKNOWLEDGMENTS
This study was partially supported by a grant from Kosin University College of Medicine in 2011.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Griffin MJ. Handbook of human vibration. 1st ed. London: Academic Press; 1990. [Google Scholar]
- 2.Seidel H. Selected health risks caused by long-term, whole-body vibration. Am J Ind Med. 1993;23:589–604. doi: 10.1002/ajim.4700230407. [DOI] [PubMed] [Google Scholar]
- 3.Ishitake T, Miyazaki Y, Ando H, Matoba T. Suppressive mechanism of gastric motility by whole-body vibration. Int Arch Occup Environ Health. 1999;72:469–474. doi: 10.1007/s004200050400. [DOI] [PubMed] [Google Scholar]
- 4.Staines WR, McIlroy WE, Brooke JD. Cortical representation of whole-body movement is modulated by proprioceptive discharge in humans. Exp Brain Res. 2001;138:235–242. doi: 10.1007/s002210100691. [DOI] [PubMed] [Google Scholar]
- 5.Cohen R. Injuries caused by physical hazards. In: LaDou J, editor. Current occupational and environmental medicine. 3rd ed. New York: McGraw-Hill; 2004. pp. 122–151. [Google Scholar]
- 6.Alund M, Larsson SE, Lewin T. Work-related persistent neck impairment: a study on former steelworks grinders. Ergonomics. 1994;37:1253–1260. doi: 10.1080/00140139408964903. [DOI] [PubMed] [Google Scholar]
- 7.Langauer-Lewowicka H, Harazin B, Brzozowska I, Szlapa P. Evaluation of health risk in machine operators exposed to whole body vibration. Med Pr. 1996;47:97–106. [PubMed] [Google Scholar]
- 8.Walker-Bone K, Palmer KT. Musculoskeletal disorders in farmers and farm workers. Occup Med (Lond) 2002;52:441–450. doi: 10.1093/occmed/52.8.441. [DOI] [PubMed] [Google Scholar]
- 9.Hart SG. Helicopter human factors. In: Wiener EL, Nagel DC, editors. Human factors in aviation. San Diego: Academic Press; 1988. pp. 591–638. [Google Scholar]
- 10.Hansen OB, Wagstaff AS. Low back pain in Norwegian helicopter aircrew. Aviat Space Environ Med. 2001;72:161–164. [PubMed] [Google Scholar]
- 11.Lopez-Lopez JA, Vallejo P, Rios-Tejada F, Jimenez R, Sierra I, Garcia-Mora L. Determination of lumbar muscular activity in helicopter pilots: a new approach. Aviat Space Environ Med. 2001;72:38–43. [PubMed] [Google Scholar]
- 12.De Oliveira CG, Nadal J. Transmissibility of helicopter vibration in the spines of pilots in flight. Aviat Space Environ Med. 2005;76:576–580. [PubMed] [Google Scholar]
- 13.Pelham TW, White H, Holt LE, Lee SW. The etiology of low back pain in military helicopter aviators: prevention and treatment. Work. 2005;24:101–110. [PubMed] [Google Scholar]
- 14.Ang B, Harms-Ringdahl K. Neck pain and related disability in helicopter pilots: a survey of prevalence and risk factors. Aviat Space Environ Med. 2006;77:713–719. [PubMed] [Google Scholar]
- 15.Schall DG. Non-ejection cervical spine injuries due to +Gz in high performance aircraft. Aviat Space Environ Med. 1989;60:445–456. [PubMed] [Google Scholar]
- 16.Hamalainen O, Vanharanta H, Kuusela T. Degeneration of cervical intervertebral disks in fighter pilots frequently exposed to high +Gz forces. Aviat Space Environ Med. 1993;64:692–696. [PubMed] [Google Scholar]
- 17.Bridger RS, Groom MR, Jones H, Pethybridge RJ, Pullinger N. Task and postural factors are related to back pain in helicopter pilots. Aviat Space Environ Med. 2002;73:805–811. [PubMed] [Google Scholar]
- 18.Petren-Mallmin M, Linder J. Cervical spine degeneration in fighter pilots and controls: a 5-yr follow-up study. Aviat Space Environ Med. 2001;72:443–446. [PubMed] [Google Scholar]
- 19.Aydog ST, Turbedar E, Demirel AH, Tetik O, Akin A, Doral MN. Cervical and lumbar spinal changes diagnosed in four-view radiographs of 732 military pilots. Aviat Space Environ Med. 2004;75:154–157. [PubMed] [Google Scholar]
- 20.Thomae MK, Porteous JE, Brock JR, Allen GD, Heller RF. Back pain in Australian military helicopter pilots: a preliminary study. Aviat space Environ Med. 1998;69:468–473. [PubMed] [Google Scholar]
- 21.De Oliveira CG, Simpson DM, Nadal J. Lumbar back muscle activity of helicopter pilots and whole-body vibration. J Biomech. 2001;34:1309–1315. doi: 10.1016/s0021-9290(01)00090-2. [DOI] [PubMed] [Google Scholar]
- 22.Bovenzi M, Hulshof CT. An updated review of epidemiologic studies on the relationship between exposure to whole-body vibration and low back pain (1986-1997) Int Arch Occup Environ Health. 1999;72:351–365. doi: 10.1007/s004200050387. [DOI] [PubMed] [Google Scholar]
- 23.Lings S, Leboeuf-Yde C. Whole-body vibration and low back pain: a systematic, critical review of the epidemiological literature 1992-1999. Int Arch Occup Environ Health. 2000;73:290–297. doi: 10.1007/s004200000118. [DOI] [PubMed] [Google Scholar]
- 24.Cheung WS, Byeon JH. Measurements of whole-body vibration exposed from and their UH60-helicopter analysis results. Trans Korean Soc Noise Vibr Eng. 2005;15:1327–1331. [Google Scholar]
- 25.Internatinal Diabetes Institute; World Health Organization. The Asia-Pacific perspective: redefining obesity and its treatment. Balmain: Health Communications Australia; 2000. [Google Scholar]
- 26.Mimura M, Panjabi MM, Oxland TR, Crisco JJ, Yamamoto I, Vasavada A. Disc degeneration affects the multidirectional flexibility of the lumbar spine. Spine (Phila Pa 1976) 1994;19:1371–1380. doi: 10.1097/00007632-199406000-00011. [DOI] [PubMed] [Google Scholar]
- 27.Silberstein CE. The evolution of degenerative changes in the cervical spine and an investigation into the "Joints of Luschka". Clin Orthop Relat Res. 1965;40:184–204. [PubMed] [Google Scholar]
- 28.Cote P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, et al. The burden and determinants of neck pain in workers: results of the Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976) 2008;33(4 Suppl):S60–S74. doi: 10.1097/BRS.0b013e3181643ee4. [DOI] [PubMed] [Google Scholar]
- 29.Bongers PM, Hulshof CT, Dijkstra L, Boshuizen HC, Groenhout HJ, Valken E. Back pain and exposure to whole body vibration in helicopter pilots. Ergonomics. 1990;33:1007–1026. doi: 10.1080/00140139008925309. [DOI] [PubMed] [Google Scholar]
- 30.Froom P, Froom J, Van Dyk D, Caine Y, Ribak J, Margaliot S, et al. Lytic spondylolisthesis in helicopter pilots. Aviat Space Environ Med. 1984;55:556–557. [PubMed] [Google Scholar]
- 31.Landau DA, Chapnick L, Yoffe N, Azaria B, Goldstein L, Atar E. Cervical and lumbar MRI findings in aviators as a function of aircraft type. Aviat Space Environ Med. 2006;77:1158–1161. [PubMed] [Google Scholar]
- 32.Viikari-Juntura E, Riihimaki H, Tola S, Videman T, Mutanen P. Neck trouble in machine operating, dynamic physical work and sedentary work: a prospective study on occupational and individual risk factors. J Clin Epidemiol. 1996;47:1411–1422. doi: 10.1016/0895-4356(94)90085-x. [DOI] [PubMed] [Google Scholar]
- 33.Ariens GA, van Mechelen W, Bongers PM, Bouter LM, van der Wal G. Physical risk factors for neck pain. Scand J Work Environ Health. 2000;26:7–19. doi: 10.5271/sjweh.504. [DOI] [PubMed] [Google Scholar]
- 34.Ashrafiuon H, Alem NM, McEntire BJ. Effects of weight and center of gravity location of head-supported devices on neck loading. Aviat Space Environ Med. 1997;68:915–922. [PubMed] [Google Scholar]
- 35.Thuresson M, Ang B, Linder J, Harms-Ringdahl K. Neck muscle activity in helicopter pilots: effect of position and helmet-mounted equipment. Aviat Space Environ Med. 2003;74:527–532. [PubMed] [Google Scholar]
- 36.Hagberg M. Occupational musculoskeletal stress and disorders of the neck and shoulder: a review of possible pathophysiology. Int Arch Occup Environ Health. 1984;53:269–278. doi: 10.1007/BF00398820. [DOI] [PubMed] [Google Scholar]
- 37.Ariens GA, Bongers PM, Douwes M, Miedema MC, Hoogendoorn WE, van der Wal G, et al. Are neck flexion, neck rotation, and sitting at work risk factors for neck pain? Results of a prospective cohort study. Occup Environ Med. 2001;58:200–207. doi: 10.1136/oem.58.3.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Seidel H. On the relationship between whole-body vibration exposure and spinal health risk. Ind Health. 2005;43:361–377. doi: 10.2486/indhealth.43.361. [DOI] [PubMed] [Google Scholar]