

Abstract
Purpose
Peri-implant sulcular fluid (PISF) has a production mechanism similar to gingival crevicular fluid (GCF). However, limited research has been performed comparing their behavior in response to inflammation. Hence, the aim of the present study was to comparatively evaluate PISF and GCF volume with varying degrees of clinical inflammatory parameters.
Methods
Screening of patients was conducted. Based on the perimucosal inflammatory status, 39 loaded implant sites were selected from 24 patients, with equal numbers of sites in healthy, peri-implant mucositis, and peri-implantitis subgroups. GCF collection was done from age- and sex-matched dentate patients, selected with gingival inflammatory status corresponding to the implant sites. Assessment of the inflammatory status for dental/implant sites was performed using probing depth (PD), plaque index/modified plaque index (PI/mPI), gingival index/simplified gingival index (GI/sGI), and modified sulcular bleeding index (BI). Sample collection was done using standardized absorbent paper strips with volumetric evaluation performed via an electronic volume quantification device.
Results
Positive correlation of the PISF and GCF volume was seen with increasing PD and clinical inflammatory parameters. A higher correlation of GCF with PD (0.843) was found when compared to PISF (0.771). PISF expressed a higher covariation with increasing grades of sGI (0.885), BI (0.841), and mPI (0.734), while GCF established a moderately positive correlation with GI (0.694), BI (0.696), and PI (0.729).
Conclusions
Within the limitations of this study, except for minor fluctuations, GCF and PISF volumes demonstrated a similar nature and volumetric pattern through increasing grades of inflammation, with PISF showing better correlation with the clinical parameters.
Keywords: Dental implants, Gingival crevicular fluid, Inflammation, Peri-implantitis
INTRODUCTION
Inflammation is the cellular and vascular response of tissues to an injurious stimulus [1], which can be due to a physical, chemical, or microbial insult. The periodontal inflammation is a localized protective response elicited by the periodontal tissues to proximate microbes and/or tissue injury and serves to destroy, dilute, or wall off both the injurious agent and the injured tissue [1]. There have been many attempts to categorize the inflammatory status of periodontal tissues [2-4]. Clinical indices such as the gingival index (GI) [2] and modified sulcular bleeding index (BI) [4] are based on the characteristics of gingival tissues during various stages of inflammation. In addition, the plaque index (PI) [3] gives an estimate of the prime factor, which is primarily responsible for the resultant inflammation. Similar indices have been developed for the measurement and quantification of the peri-implant inflammatory response [4-6]. These indices, along with probing depth (PD) measurement [7] and radiographic examination, form the traditional means of detecting peri-implant pathologies. Although easily applicable, these indices lack the capability to objectively assess the onset and progression of periodontal and peri-implant destructive changes [8]. In the context of implants, it is crucial to detect the presence of inflammation in its early stages, as early implant morbidity and failure pose a great financial burden to both the patient and the clinician.
The gingival crevicular fluid (GCF) is a tissue fluid that seeps through the crevicular and junctional epithelium [1]. In 1899, Black [9] first reported the presence of a fluid in the periodontal sulcus. However, the exact nature of the fluid, its origin, and its composition has been controversial. Brill [10] and Egelberg [11,12] suggested that GCF production was due to an increase in the permeability of the vessels underlying the junctional and sulcular epithelium, which might occur due to inflammation, trauma, or mechanical stimulation. Later, Alfano [13] suggested that even the presence of highly osmotic substances in the gingival sulcus (bacterial products, plaque) might lead to production of an initial transudate fluid. This hypothesis was supported by Pashley [14], who predicted that when the rate of capillary filtrate exceeds that of lymphatic uptake, fluid will accumulate as edema and/or leave the area as GCF. Factors that alter this process include the filtration coefficients of the capillary endothelium and the osmotic pressure within the different compartments.
Various attempts have been made to quantitate and interpret the relationship of GCF with increasing grades of inflammation [15,16]. Raised levels of GCF have been reported as the first sign of developing gingival inflammation [17]. Stewart et al. [18] suggested that crevicular fluid measurement should be viewed as an objective indicator of the degree of periodontal tissue inflammation. In 1989, Apse et al. [19] demonstrated the presence of a similar fluid in the peri-implant sulcus, which was termed the peri-implant sulcular fluid (PISF). It was noted that crevicular fluid was present in the osseointegrated implant sulcus, but its flow did not differ from that observed from tooth sites in either partially edentulous or edentulous patients. It was thus concluded that the characteristics of implant sulci appeared to be similar to periodontal sulci with respect to crevicular fluid flow and microflora.
Although the mechanism and rate of PISF production was reported to be similar to GCF, some volumetric differences might occur due to the presence of structural and vascular dissimilarities in the peri-implant and gingival mucosa [20]. Furthermore, it is essential to validate the association of the PISF volume with the peri-implant clinical parameters, as compared to a standardized fluid, GCF, the behavior of which has been extensively studied. As there has been limited research on the comparative volumetric assessment of these two fluids with regard to the inflammatory clinical indices, the aim of our study was to quantify GCF and PISF levels and comparatively assess their relationship with the various clinical indices used to estimate the gingival and peri-implant inflammation.
MATERIALS AND METHODS
Patient selection
The project was carried out in the Department of Periodontology, Krishnadevaraya College of Dental Sciences, Bangalore, India. The study protocol was approved by the institutional ethics committee (approval KCDS/302/PG/2011-12). Written informed consent was obtained from all of the subjects included in the study. While conducting the study, the ethical principles outlined in the Declaration of Helsinki for research involving human subjects, as revised in 2000, were followed. For the purpose of PISF estimation, 59 implant sites from 34 patients were screened, from which 39 loaded dental implant (Tapered select implant system, Nobel Biocare, Göteborg, Sweden) sites from 24 patients were selected. The patient ages ranged from 35 to 60 years, with a mean of 47 years. All of the patients had undergone two-stage implant placement procedure, with more than 6 months of prosthetic rehabilitation. Patients having an unremarkable medical history, no known allergies or metabolic diseases, no smoking habit, and no history of any antibiotic treatment within three months, were included in this study. GCF collection and estimation was done from age- and sex-matched subjects, from corresponding maxillary and mandibular sites with inflammatory status equable to the implant sites. The patients were required to be systemically healthy, with no antibiotic exposure or oral prophylaxis treatment three months prior to project commencement. The procedure for patient selection and conduction of the study is presented in Fig. 1.
Figure 1.

Schematic diagram for the pattern followed during the course of the study. PD: probing depth, PISF: peri-implant sulcular fluid, GCF: gingival crevicular fluid, GI: gingival index, n: number of sampling sites.
Clinical examination
To avoid the risk of volumetric fluctuation due to mechanical irritation, the clinical examination was performed a week before PISF and GCF sampling. For the assessment of the dental clinical status, the PD (6 sites per tooth), PI [3], GI [2], and modified sulcular BI [4] were employed. The clinical status of peri-implant tissues was evaluated by assessing the PD (6 sites per implant) and corresponding indices for implants, including a modified plaque index (mPI) [4], simplified gingival index (sGI) [6], and a modified bleeding index (mBI) [4].
Examiner calibration
Calibration exercises for clinical parameters and fluid volume estimation were performed in five patients before the actual study. Clinical recordings were done twice by a single examiner (Smiti Bhardwaj, SB), within the duration of a week. The order of patients was masked and changed in between the examinations. The examiner received training prior to the study regarding the use of each index employed for periodontal and peri-implant examination. PD was measured using a pressure-sensitive probe (Florida Probe, Gainesville, FL, USA), and the estimation was judged to be reproducible if the agreement within ±1 mm between repeated measurements was at least 90%. The intraexaminer agreement between the two measurements was found to be 91%. A different examiner (M.L.V.P.), who was blinded to the clinical records of the patients, carried out the fluid sampling.
Determination of groups
According to the clinical examination, the sites were divided into healthy, gingivitis/peri-implant mucositis, and periodontitis/peri-implantitis groups. Intragroup volumetric assessments were also performed separately for maxillary and mandibular sites. The grouping criteria used is displayed in Fig. 2.
Figure 2.

Criteria for formulation of subgroups. PD: probing depth, GI: gingival index.
Sample collection
Both implant and dentate patients were scheduled for sample collection during the morning hours that is, from 9 AM to 11 AM, to prevent any diurnal variations affecting the crevicular fluid volume. To ensure accessibility, isolation, and standardization, sampling was performed only in corresponding dental/implant mesio-buccal sites. For the purpose of standardization, the GCF/PISF samples were collected from individuals matched by age group and demonstrating similar inflammatory gingival and peri-implant mucosal conditions. Because the diameter of the sulcus and the area of the sulcular epithelium are known to influence the crevicular fluid volume [21], sample collection was confined to the implants and teeth present in the anterior sextant.
The patients were instructed to refrain from food and vigorous oral hygiene measures 90 minutes prior to sample collection. To avoid salivary contamination, the selected sites were rinsed with water, isolated by cotton rolls, and dried with a gentle air spray. A saliva ejector was being concurrently used during the sampling protocol. The fluid sample was collected from both the test groups by standardized absorbent paper strips (PerioPaper, Periocol, Oraflow Inc., Amityville, NY, USA), the volumetric evaluation for which was accomplished by an electronic fluid volume quantification device (Periotron 8000, Ora Flow Inc., Amityville, NY, USA). Supragingival plaque was removed with a dry gauze, and a standardized paper strip was inserted 1-2 mm into the sulcus. The strip was held in place for 30 seconds and transferred to a precalibrated electronic fluid quantification device.
PISF/GCF volume determination
The electronic fluid quantification device was calibrated before beginning the sample collection procedure using standardized paper strips and loaded with a test fluid (distilled water) from a standardized graduated syringe (Hamilton 0-5.0 µL micro syringe, Hamilton Co., Reno, NV, USA); a calibration curve was then generated. To eliminate the risk of evaporation, the paper strips were transferred to the device within 0-5 seconds [22]. The test paper strip was placed at a standard distance between the electrodes of the device [23]. A digital readout was obtained in the form of Periotron Units and was converted to microliters using specialized software (MLCONVERT.EXE ver. 2.52, OraFlow Inc., New York, NY, USA). The electrodes of the device were dried after each measurement using dry cotton. The device was recalibrated periodically.
Statistical analysis
The sample size and power estimation was performed using results from a pilot study, by a statistical software (PASS ver. XI, NCSS, Kaysville, UT, USA). With a minimum difference of 0.12 µL in the volumes of peri-implantitis and healthy peri-implant sulcular fluid and standard deviations of 0.08 and 0.13, respectively, the effect size was around 1.1428. With an α-error of 5% and a power of 80%, the required sample size was estimated to be 13 in each sub-group. A normality assumption for the data was tested using the Shapiro-Wilk test. Mean comparisons within the group were computed using analysis of variance, after which multiple comparisons within the groups were conducted using the Sidak test. The intergroup comparisons were carried out using Tukey test. For nonparametric data, the Kruskal-Wallis and Mann Whitney U tests were used. Pearson correlation coefficient was calculated to analyze the relationship between PISF and GCF values, with regard to the different clinical parameters. For all parameters, P values <0.05 were considered to be statistically significant.
RESULTS
The present study included a total of 39 loaded implant and dentate sites. The implants were treated with a fixed implant supported prosthesis, and the measurements were recorded in the loaded state.
Analysis of clinical parameters in GCF and PISF groups
In the comparisons among subgroups of GCF (healthy, gingivitis, periodontitis) and PISF (healthy, mucositis, peri-implantitis), several differences and similarities were detected (Tables 1 and 2). The assessment of gingival inflammation by the GI and sGI revealed significant differences between the healthy and gingivitis/peri-implant mucositis groups and between the healthy and periodontitis/peri-implantitis subgroups (P<0.05). However, for both the dentate and implant sites, the degree of gingival inflammation between gingivitis and periodontitis and between peri-implant mucositis and peri-implantitis was nonsignificant (P>0.05). The PI for the GCF group presented a significant increase within intragroup comparisons, with P<0.05 (healthy<gingivitis<periodontitis). At the implant sites, although the plaque levels were highest in the peri-implantitis subgroup, when compared, the peri-implant mucositis and peri-implantitis subgroups failed to show any significant difference (P>0.05). The BI showed similar significant patterns among the intragroup comparisons (healthy<mucositis<peri-implantitis), except in the gingivitis versus periodontitis comparison, where no statistically significant difference was found (P>0.05). The PD for both groups, GCF and PISF, and all subgroup comparisons showed a constant and significant increase (P<0.05; healthy<gingivitis<periodontitis; healthy<mucositis<peri-implantitis).
Table 1.
Intergroup comparison of clinical parameters and PISF volume.
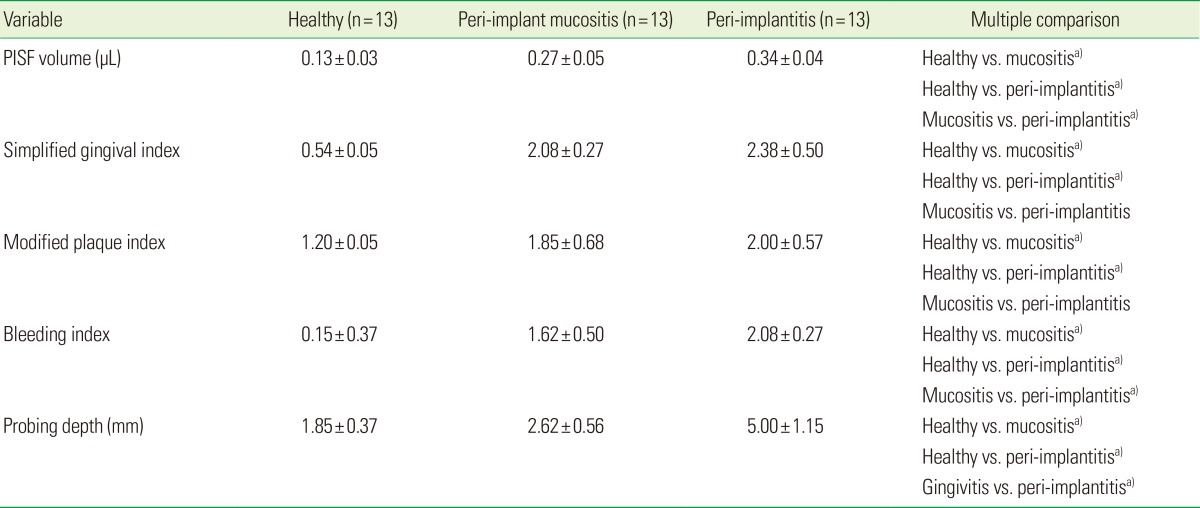
Values are presented as mean±standard deviation.
PISF: peri-implant sulcular fluid.
a)P-value≤0.05.
Table 2.
Intergroup comparison of clinical parameters and GCF volume.
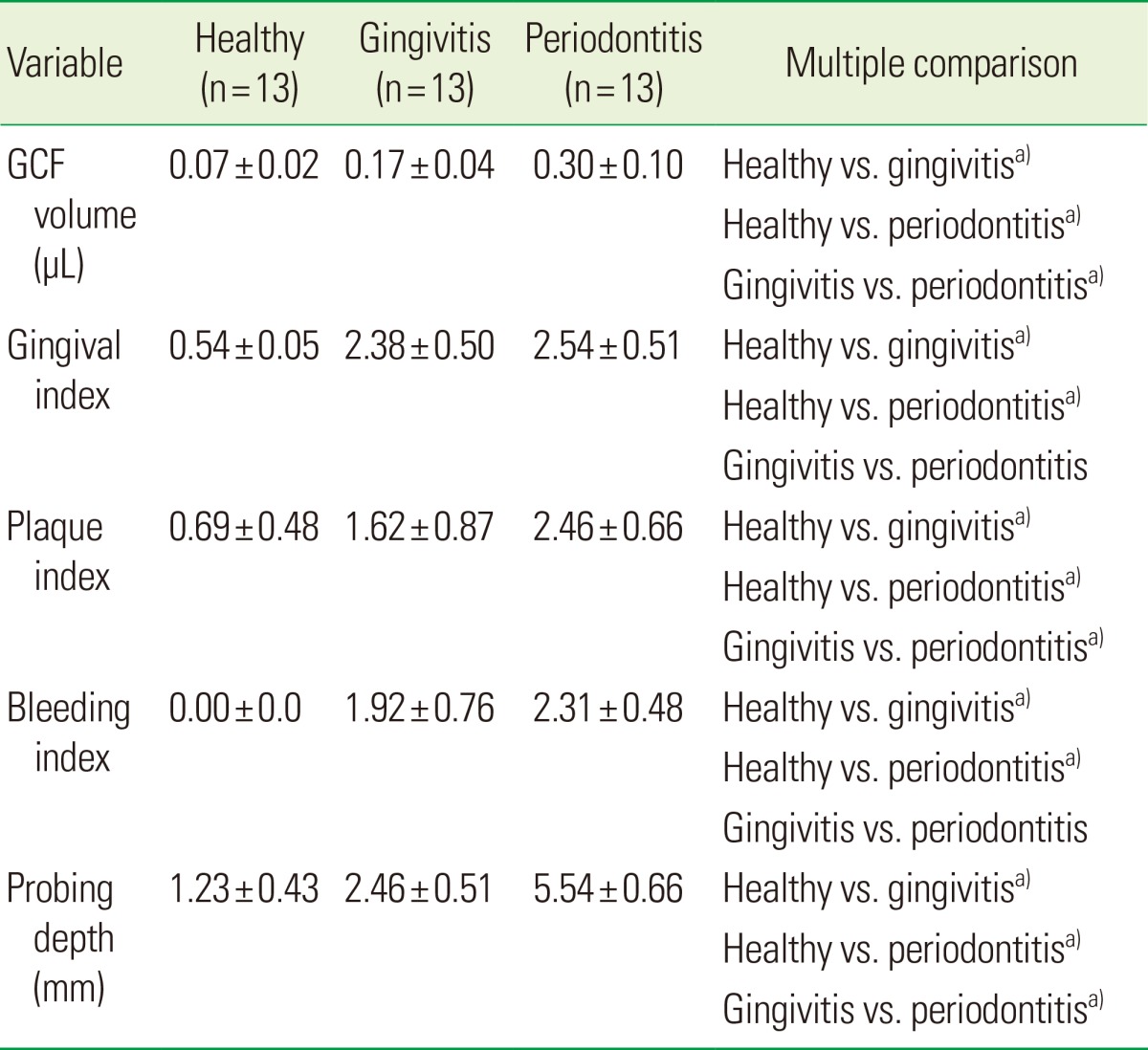
Values are presented as mean±standard deviation.
GCF: gingival crevicular fluid.
a)P-value ≤0.05.
Analysis of PISF and GCF volumes based on inflammation
The PISF volumes were significantly higher at sites with peri-implant mucositis (0.27±0.04 µL) and peri-implantitis (0.34±0.04 µL) compared to clinically healthy sites (0.13±0.03 µL) (P<0.0001). The data for the same has been presented in Tables 1 and 2. Analyses demonstrated the trend of an increase in PISF volume with greater severity of peri-implant inflammation (healthy<peri-implant mucositis<peri-implantitis). The peri-implantitis group also showed a significant raise in the PISF volume over the peri-implant mucositis group. This finding was comparable to the GCF subgroups, wherein the healthy (0.07±0.02), gingivitis (0.17±0.04), and periodontitis (0.30±0.10) groups had significant differences in their volumes (P<0.05).
Analysis of PISF and GCF volumes based on location: maxillary/mandibular
When the GCF and PISF subgroups were compared with respect to the location of the teeth and implants, that is, maxillary or mandibular (Table 3), distinct features came to the fore. Although the GCF subgroups showed a higher volume in the maxillary sites, only the gingivitis subgroup demonstrated a statistically significant difference (maxillary, 0.20 µL; mandibular, 0.14 µL; P<0.005). Conversely, the PISF group failed to show any relationship with the site of sample collection. The healthy and peri-implantitis subgroups displayed an insignificant edge in mandibular volume over maxillary volumes. On the other hand, the peri-implant mucositis subgroup showed an increase in maxillary PISF levels.
Table 3.
Data of subgroups based on location of dental implants (maxillary/mandibular).
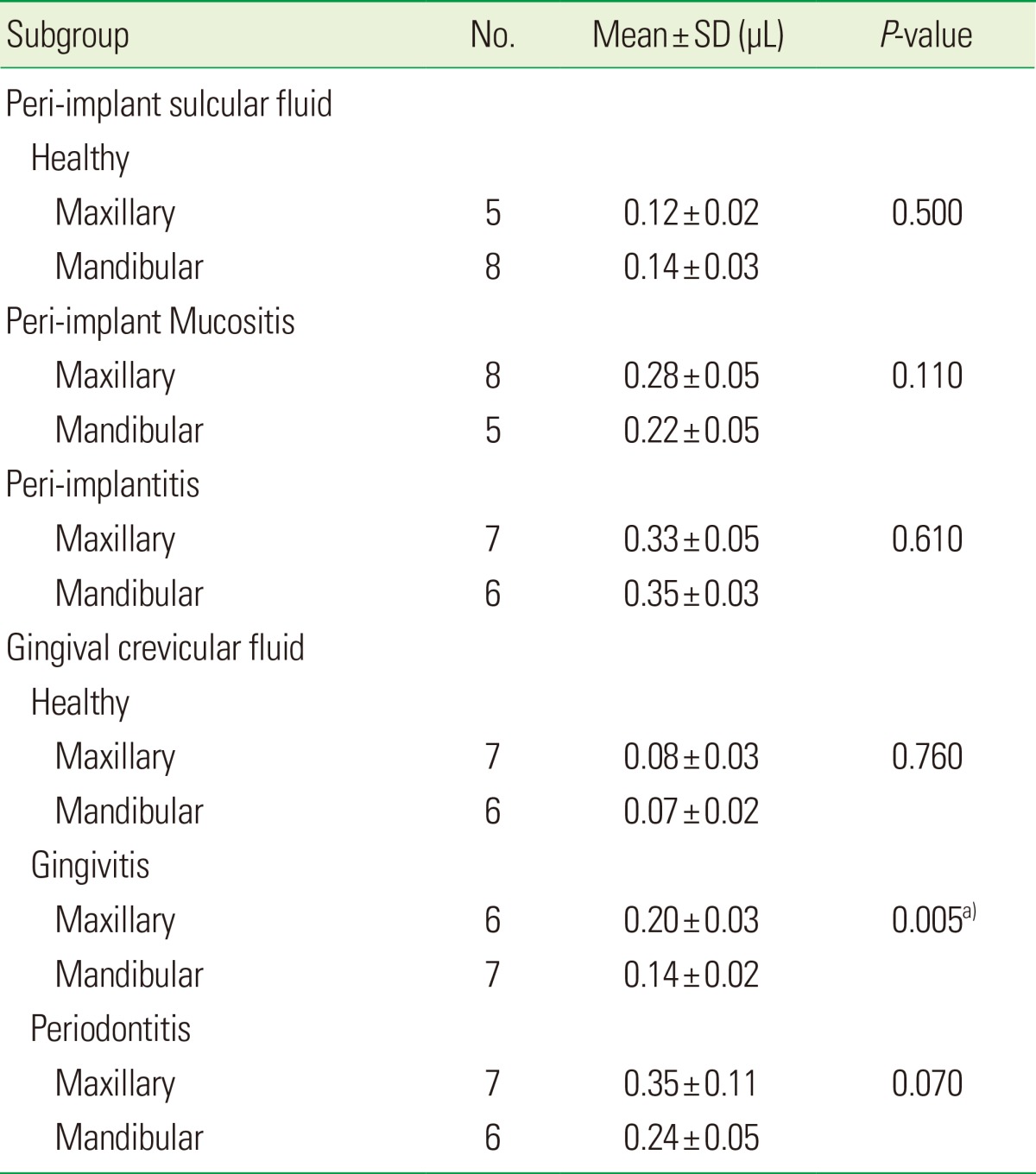
SD: standard deviation.
a)P-value≤0.05.
Analysis of PISF and GCF volumes based on clinical parameters
For the purpose of comparative assessment between GCF and PISF volumes, their Pearson coefficient correlation was determined against the clinical parameters (Table 4).
Table 4.
Correlation between clinical parameters and corresponding GCF and PISF volume.
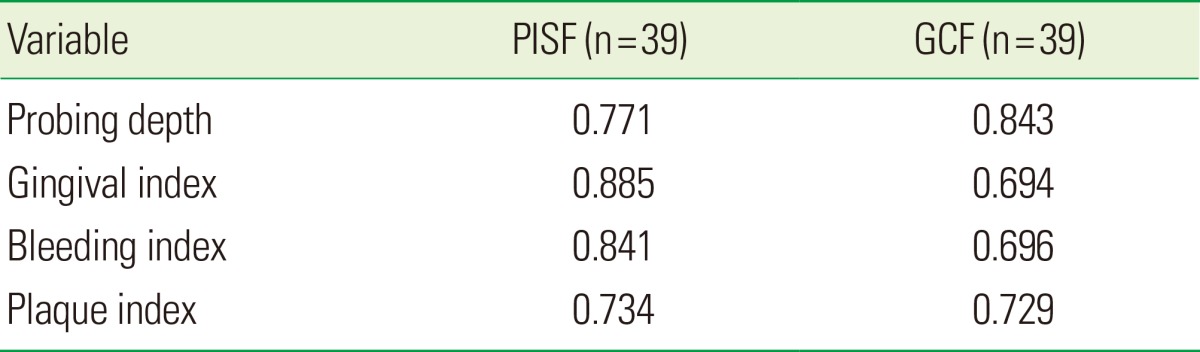
PISF: peri-implant sulcular fluid, GCF: gingival crevicular fluid.
Probing depth
When the overall GCF and PISF volumes were compared with increasing probing depths, both fluids showed a strongly positive correlation (Fig. 3A). However, GCF demonstrated a better correlation with increasing probing depths (0.843) when compared to PISF (0.771).
Figure 3.

Diagrammatic representation of correlation between clinical parameters and corresponding PISF and GCF volumes (µL). (A) PISF-GCF vs. PD. (B) PISF-GCF vs. GI/sGI. (C) PISF-GCF vs. BI. (D) PISF-GCF vs. PI/mPI. PISF: peri-implant sulcular fluid, GCF: gingival crevicular fluid, PD: probing depth, GI: gingival index, sGI: simplified gingival index, BI: bleeding index, PI: plaque index, mPI: modified plaque index.
GI/sGI
PISF expressed a higher covariation with increasing grades of sGI (0.885), while a moderately positive correlation of 0.694 was established for GCF with GI (Fig. 3B).
BI
The comparison between the correlation of GCF and PISF with the BI demonstrated a higher PISF modulation (0.841) with increasing BI grades than that of GCF (0.696) (Fig. 3C).
PI/mPI
Both PISF (0.734) and GCF (0.729) registered a positive correlation with the mPI/PI (Fig. 3D).
DISCUSSION
The clinical assessment of peri-implant tissues is necessary to detect early signs of disease and appropriately plan therapeutic interventions. Peri-implant mucositis describes an inflammatory lesion that resides in the mucosa, while peri-implantitis also affects the supporting bone [24]. As stated by Lindhe et al. [24] in 2008, peri-implant mucositis can be identified clinically by redness and swelling of the soft tissue, but bleeding on probing still forms the primary feature depicting the onset and progression of inflammation. In peri-implantitis, however, the mucosal lesion is often associated with suppuration and deepened pockets, and is always accompanied by the loss of supporting marginal bone. It has been noted previously that the conditions of peri-implant mucositis and peri-implantitis are comparable to gingivitis and periodontitis, respectively [20]. Considering this fact, comparable groupings were created for the crevicular fluid comparison, where direct comparisons between healthy, gingivitis versus peri-implant mucositis, and periodontitis versus peri-implantitis were performed. However, inflamed peri-implant tissues show a faster rate of conversion to destructive peri-implantitis than gingival tissues [25]. Hence, for an early, unbiased, and objective assessment of the peri-implant tissues in health and disease, the stages of peri-implant disease should be appropriately defined according to justifiably measureable, sensitive clinical parameters and indices.
Froum and Rosen [26] stated that a ≥4 mm probing depth should be present on at least two aspects of the concerned implant along with bone loss to classify it as peri-implantitis. This definition was used in the present study to distinguish conditions of peri-implant mucositis from peri-implantitis. The probing depth around implants may vary according to the condition of the overlying mucosa, amount of keratinized tissue, the probing pressure, and the restoration design [27]. To alleviate variations caused by these parameters, the baseline probing depths at the time of prosthesis insertion (not included) were taken into consideration and recordings were made using a pressure-sensitive probe. The access to the base of the implant sulcus during probing depth measurement might be obviated by the restoration design, which entails the consideration of its removal. However, during the examinations, no difficulty in access to the sulcular base was observed. Hence, all of the measurements were performed during loaded conditions only.
Bacterial plaque is considered the key inducer of several periodontal diseases. In 1967, Loe [3] detailed a highly utilitarian and objective system for plaque assessment, which was used in the present study for the appraisal of individual tooth sites. For the assessment of bleeding on probing, Mombelli et al. [4]'s BI was used instead of a dichotomous score. This is because we intended to analyze the characteristics of bleeding rather than its mere presence or absence. The GI was used for the characterization of the periodontal inflammation [2].
Indices specifically modulated and customized for implants were used for implant site assessment. Mombelli et al. [4] modified the original PI introduced by Loe and Silness [2] to assess biofilm formation in the marginal area around implants (mPI). This index eased the applicability and assessment at the implant sites, and therefore, its usage appeared meaningful for monitoring and quantifying plaque accumulation. In 2006, Strbac et al. [28], demonstrated a positive correlation between increasing grades of periodontal inflammation and mPI and mBI. The present study demonstrated that the plaque levels, although higher in th eperi-implantitis group, were not significantly different from those of the peri-implant mucositis group, suggesting that an increase in the severity of inflammation around implants may not necessarily require an increase in plaque accumulation.
The modified sulcular BI was adopted from Mombelli et al. [4] in 1987 for the purpose of this study, as it has been modified for application to implant assessment as well [29]. Chronic gingivitis and peri-implant mucositis lesions showing bleeding suggest conspicuous epithelial changes and vascular transfiguration [25]. A study by Luterbacher et al. [30] in 2000 demonstrated a higher diagnostic accuracy for bleeding on probing around implants when compared with that around teeth. This was confirmed in the current study, wherein periodontitis sites failed to show a significant rise in the BI over gingivitis, while all of the three implant subgroups displayed a significant rise in BI. This indicates that peri-implant mucosa gives a bleeding response more readily than periodontal sites.
The tissue texture and color of the peri-implant mucosa may be influenced by the appearance of the recipient tissues before implant placement, their keratinization status (with nonkeratinized tissues appearing redder than keratinized tissues), and the material characteristics of the implant surface [31,32]. These features carry the potential to jeopardize the interpretations of the GI and have resulted in a poor correlation between GI scores and changes in peri-implant crestal bone levels [32]. However, it is essential to correlate the changes in PISF levels according to the changes in mucosal inflammation around implants. Hence, a sGI [6] modified from the original GI [2] for easy applicability around implants was used for the peri-implant mucosal inflammation assessment. The current study showed a similar manifestation of inflammation in peri-implant mucosa and gingiva, with the GI and sGI revealing no statistically significant differences.
GCF measurement has been considered an objective indicator of the degree of periodontal tissue inflammation [18]. It has also been suggested that both GCF and PISF could be useful markers of early inflammation in both gingival and peri-implant tissues [33]. The production mechanism of PISF has been shown to be similar to GCF [19]; this study, however, concentrates on whether there are variations between the two fluids depending upon the clinical inflammatory variants. Pearsons' correlation coefficient was estimated and compared within the GCF and PISF groups and inflammatory subgroups to directly compare the effects of clinical parameters on PISF and GCF volumes. The volumes of PISF and GCF were not concurrently compared to each other; rather, the relative changes in their volumes with varying clinical parameters were each compared. This is due to the fact that the dimensions of the sulci might influence the volume recordings for both dentate and implant sites [34].
In studies determining the volumetric features of PISF [34-37] and GCF [38,39], an increased volume was seen with an increasing grade and extent of inflammation. Similar results were reported in the present study. An overall GCF and PISF volumetric comparison with increasing probing depths revealed a positive correlation for both fluids. The correlation of GCF with increasing probing depth was 0.843, which was higher when compared to PISF (0.771).
Chaytor et al. [32] concluded that the GI insufficiently portrays deeper inflammatory changes and corresponding bone levels. However, as production of the crevicular fluid is a mucosal phenomenon, the recording of gingival and peri-implant mucosal inflammation was considered essential for depicting soft-tissue inflammatory changes. The results indicate that the soft tissue inflammation demonstrates a strongly positive influence over the fluid volumes produced. In addition, the covariation of the PISF volume appeared higher than that of the GCF volume when compared against increasing grades of GI/sGI. In a pilot study, Niimi and Ueda [40] demonstrated increased PISF volume at implant sites with increasing grades of GI and PI. This is in agreement with the present study, where correlations between the PISF/GCF volume and all of the clinical indices (PI, BI, and GI) were also strongly positive and significant. A better correlation was observed with PISF and the clinical parameters rather than GCF. Hence, if the GCF volume is considered to be a reliable objective indicator for increasing grades of periodontal inflammation, then the PISF volume could be considered an indicator more adept for analyzing the development of peri-implant mucosal inflammation.
When fluid volumes were compared according to their location, GCF sites depicted a trend towards increased volume in maxillary sites. This is in accordance with the study conducted by Griffiths et al. [15], where it was shown that both the flow rate and resting volumes of GCF were higher in the maxillary sites when compared to those of the mandibular sites. The PISF sites failed to show any correlation with the location of the implants. Gunday et al. [34] suggested a reverse pattern in relation to PISF volume, with mandibular sites, rather than maxillary sites, demonstrating an increased volume. However, this was not confirmed in the present study.
Crevicular fluid volumes are highly variable within subjects; hence, methods to devise a definitive volume range could not be successfully applied to categorize inflammation. However, for a particular patient, by keeping the time, site, and method of GCF/PISF collection constant, a follow-up routine can be maintained. Major positive fluctuations in PISF volumes for an implant site, when compared with previous measurements, might thus reveal a developing subclinical inflammation. The use of indices specifically reformulated for implant assessment ensures ease and precision in clinical applicability and should be encouraged. This study demonstrated that the relationships of GCF and PISF volumes to clinical parameters do not significantly differ from each other. Hence, this finding could be applied while collecting full mouth crevicular fluid samples, where samples from both dental and implant sites could be collected, without suppositions of abrupt volumetric changes affecting dental and implant sites differently. Thus, it could be concluded that within the limitations of this study, except for minor fluctuations, GCF and PISF volumes show a similar nature and pattern through increasing grades of inflammation, with PISF showing marginally better correlation with the clinical indices. Future studiesshould be conducted to confirm these results, employing a larger sample size; in addition, further research should be carried out with a larger sample size to determine the factors that modulate PISF volume production.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.American Academy of Periodontology. Glossary of periodontal terms. Chicago: American Academy of Periodontology; 2001. [Google Scholar]
- 2.Loe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand. 1963;21:533–551. doi: 10.3109/00016356309011240. [DOI] [PubMed] [Google Scholar]
- 3.Loe H. The gingival index, the plaque index and the retention index systems. J Periodontol. 1967;38(6) Suppl:610–616. doi: 10.1902/jop.1967.38.6.610. [DOI] [PubMed] [Google Scholar]
- 4.Mombelli A, van Oosten MA, Schurch E, Jr, Land NP. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol Immunol. 1987;2:145–151. doi: 10.1111/j.1399-302x.1987.tb00298.x. [DOI] [PubMed] [Google Scholar]
- 5.Lindquist LW, Rockler B, Carlsson GE. Bone resorption around fixtures in edentulous patients treated with mandibular fixed tissue-integrated prostheses. J Prosthet Dent. 1988;59:59–63. doi: 10.1016/0022-3913(88)90109-6. [DOI] [PubMed] [Google Scholar]
- 6.Apse P, Zarb GA, Schmitt A, Lewis DW. The longitudinal effectiveness of osseointegrated dental implants. The Toronto Study: peri-implant mucosal response. Int J Periodontics Restorative Dent. 1991;11:94–111. [PubMed] [Google Scholar]
- 7.Gargiulo AW, Wentz FM, Orban B. Dimensions and relations of dentogingival junctions in humans. J Periodontol. 1961;32:261–267. [Google Scholar]
- 8.Karbach J, Callaway A, Kwon YD, d'Hoedt B, Al-Nawas B. Comparison of five parameters as risk factors for peri-mucositis. Int J Oral Maxillofac Implants. 2009;24:491–496. [PubMed] [Google Scholar]
- 9.Black GV. The fibers and glands of the peridental membrane. Dent Cosmos. 1899;41:101–122. [Google Scholar]
- 10.Brill N. Influence of capillary permeability on flow of tissue fluid into gingival pockets. Acta Odontol Scand. 1959;17:23–33. [Google Scholar]
- 11.Egelberg J. Permeability of the dento-gingival blood vessels. 1. Application of the vascular labelling method and gingival fluid measurements. J Periodontal Res. 1966;1:180–191. doi: 10.1111/j.1600-0765.1966.tb01858.x. [DOI] [PubMed] [Google Scholar]
- 12.Egelberg J. Permeability of the dento-gingival blood vessels. III. Chronically inflamed gingivae. J Periodontal Res. 1966;1:287–296. doi: 10.1111/j.1600-0765.1966.tb01873.x. [DOI] [PubMed] [Google Scholar]
- 13.Alfano MC. The origin of gingival fluid. J Theor Biol. 1974;47:127–136. doi: 10.1016/0022-5193(74)90103-9. [DOI] [PubMed] [Google Scholar]
- 14.Pashley DH. A mechanistic analysis of gingival fluid production. J Periodontal Res. 1976;11:121–134. doi: 10.1111/j.1600-0765.1976.tb00060.x. [DOI] [PubMed] [Google Scholar]
- 15.Griffiths GS, Sterne JA, Wilton JM, Eaton KA, Johnson NW. Associations between volume and flow rate of gingival crevicular fluid and clinical assessments of gingival inflammation in a population of British male adolescents. J Clin Periodontol. 1992;19:464–470. doi: 10.1111/j.1600-051x.1992.tb01158.x. [DOI] [PubMed] [Google Scholar]
- 16.Ozkavaf A, Aras H, Huri CB, Mottaghian-Dini F, Tozum TF, Etikan I, et al. Relationship between the quantity of gingival crevicular fluid and clinical periodontal status. J Oral Sci. 2000;42:231–238. doi: 10.2334/josnusd.42.231. [DOI] [PubMed] [Google Scholar]
- 17.Lindhe J, Hamp SE, Loe H. Experimental periodontitis in the beagle dog. Int Dent J. 1973;23:432–437. [PubMed] [Google Scholar]
- 18.Stewart JE, Christenson PD, Maeder LA, Palmer MA. Reliability of filter-strip sampling of gingival crevicular fluid for volume determination using the Periotron. J Periodontal Res. 1993;28:227–230. doi: 10.1111/j.1600-0765.1993.tb01073.x. [DOI] [PubMed] [Google Scholar]
- 19.Apse P, Ellen RP, Overall CM, Zarb GA. Microbiota and crevicular fluid collagenase activity in the osseointegrated dental implant sulcus: a comparison of sites in edentulous and partially edentulous patients. J Periodontal Res. 1989;24:96–105. doi: 10.1111/j.1600-0765.1989.tb00863.x. [DOI] [PubMed] [Google Scholar]
- 20.Lang NP, Berglundh T Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: where are we now? Consensus of the Seventh European Workshop on Periodontology. J Clin Periodontol. 2011;38(Suppl 11):178–181. doi: 10.1111/j.1600-051X.2010.01674.x. [DOI] [PubMed] [Google Scholar]
- 21.Hatipoglu H, Yamalik N, Berberoglu A, Eratalay K. Impact of the distinct sampling area on volumetric features of gingival crevicular fluid. J Periodontol. 2007;78:705–715. doi: 10.1902/jop.2007.060331. [DOI] [PubMed] [Google Scholar]
- 22.Tozum TF, Hatipoglu H, Yamalik N, Gursel M, Alptekin NO, Ataoglu T, et al. Critical steps in electronic volume quantification of gingival crevicular fluid: the potential impact of evaporation, fluid retention, local conditions and repeated measurements. J Periodontal Res. 2004;39:344–357. doi: 10.1111/j.1600-0765.2004.00758.x. [DOI] [PubMed] [Google Scholar]
- 23.Ciantar M, Caruana DJ. Periotron 8000: calibration characteristics and reliability. J Periodontal Res. 1998;33:259–264. doi: 10.1111/j.1600-0765.1998.tb02198.x. [DOI] [PubMed] [Google Scholar]
- 24.Lindhe J, Meyle J Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008;35(8 Suppl):282–285. doi: 10.1111/j.1600-051X.2008.01283.x. [DOI] [PubMed] [Google Scholar]
- 25.Lang NP, Bosshardt DD, Lulic M. Do mucositis lesions around implants differ from gingivitis lesions around teeth? J Clin Periodontol. 2011;38(Suppl 11):182–187. doi: 10.1111/j.1600-051X.2010.01667.x. [DOI] [PubMed] [Google Scholar]
- 26.Froum SJ, Rosen PS. A proposed classification for peri-implantitis. Int J Periodontics Restorative Dent. 2012;32:533–540. [PubMed] [Google Scholar]
- 27.Mombelli A, Graf H. Depth-force-patterns in periodontal probing. J Clin Periodontol. 1986;13:126–130. doi: 10.1111/j.1600-051x.1986.tb01444.x. [DOI] [PubMed] [Google Scholar]
- 28.Strbac GD, Monov G, Cei S, Kandler B, Watzek G, Gruber R. Cathepsin K levels in the crevicular fluid of dental implants: a pilot study. J Clin Periodontol. 2006;33:302–308. doi: 10.1111/j.1600-051X.2006.00904.x. [DOI] [PubMed] [Google Scholar]
- 29.Salvi GE, Lang NP. Diagnostic parameters for monitoring peri-implant conditions. Int J Oral Maxillofac Implants. 2004;19(Suppl):116–127. [PubMed] [Google Scholar]
- 30.Luterbacher S, Mayfield L, Bragger U, Lang NP. Diagnostic characteristics of clinical and microbiological tests for monitoring periodontal and peri-implant mucosal tissue conditions during supportive periodontal therapy (SPT) Clin Oral Implants Res. 2000;11:521–529. doi: 10.1034/j.1600-0501.2000.011006521.x. [DOI] [PubMed] [Google Scholar]
- 31.Listgarten MA, Lang NP, Schroeder HE, Schroeder A. Periodontal tissues and their counterparts around endosseous implants. Clin Oral Implants Res. 1991;2:1–19. doi: 10.1034/j.1600-0501.1991.020309.x. [DOI] [PubMed] [Google Scholar]
- 32.Chaytor DV, Zarb GA, Schmitt A, Lewis DW. The longitudinal effectiveness of osseointegrated dental implants. The Toronto Study: bone level changes. Int J Periodontics Restorative Dent. 1991;11:112–125. [PubMed] [Google Scholar]
- 33.Schierano G, Pejrone G, Brusco P, Trombetta A, Martinasso G, Preti G, et al. TNF-alpha TGF-beta2 and IL-1beta levels in gingival and peri-implant crevicular fluid before and after de novo plaque accumulation. J Clin Periodontol. 2008;35:532–538. doi: 10.1111/j.1600-051X.2008.01224.x. [DOI] [PubMed] [Google Scholar]
- 34.Gunday S, Topcu AO, Guncu GN, Akman CS, Karabulut E, Yamalik N. Analysis of potential factors affecting peri implant sulcus fluid volume. Clinical Dent Res. 2011;35:12–24. [Google Scholar]
- 35.Tozum TF, Turkyilmaz I, Yamalik N, Tumer C, Kilinc A, Kilinc K, et al. Analysis of thte possible impact of inflammation severity and early and delayed loading on nitric oxide metabolism around dental implants. Int J Oral Maxillofac Implants. 2005;20:547–556. [PubMed] [Google Scholar]
- 36.Guncu GN, Tozum TF, Guncu MB, Yamalik N, Tümer C, Karabulut E, et al. Myeloperoxidase as a measure of polymorphonuclear leukocyte response in inflammatory status around immediately and delayed loaded dental implants: a randomized controlled clinical trial. Clin Implant Dent Relat Res. 2008;10:30–39. doi: 10.1111/j.1708-8208.2007.00058.x. [DOI] [PubMed] [Google Scholar]
- 37.Tozum TF, Guncu GN, Yamalik N, Turkyilmaz I, Guncu MB. The impact of prosthetic design on the stability, marginal bone loss, peri-implant sulcus fluid volume, and nitric oxide metabolism of conventionally loaded endosseous dental implants: a 12-month clinical study. J Periodontol. 2008;79:55–63. doi: 10.1902/jop.2008.070351. [DOI] [PubMed] [Google Scholar]
- 38.Mann WV. The correlation of gingivitis pocket depth and exudate from the gingival crevice. J Periodontol. 1963;34:379–387. [Google Scholar]
- 39.Oliver RC, Holm-Pederen P, Loe H. The correlation between clinical scoring, exudate measurements and microscopic evaluation of inflammation in the gingiva. J Periodontol. 1969;40:201–209. doi: 10.1902/jop.1969.40.4.201. [DOI] [PubMed] [Google Scholar]
- 40.Niimi A, Ueda M. Crevicular fluid in the osseointegrated implant sulcus: a pilot study. Int J Oral Maxillofac Implants. 1995;10:434–436. [PubMed] [Google Scholar]