

Abstract
Objective
This study examined the effects of a collaborative care intervention for anxiety disorders in primary care on lower income participants relative to those with higher incomes. The authors hypothesized that lower income patients might show less improvement or improve at a lower rate given that they experience greater economic stress over the treatment course. Alternatively, lower income patients could improve at a higher rate because the intervention facilitates access to evidence-based treatment, which typically is less available to persons with lower incomes.
Method
The authors compared baseline demographic and clinical characteristics of patients with lower (n=287) and higher (n=717) income using t-tests and chi-square tests for continuous and categorical variables respectively. For the longitudinal analysis of intervention effects by income group, the authors jointly modeled the outcomes at the four assessment times by study site; income; time; intervention; time and intervention; income and time; income and intervention; and time, intervention and income.
Results
Although lower-income participants were more ill and disabled at baseline than those in the higher income group, the two income groups were very similar in their clinical response. The lower income participants experienced a comparable degree of clinical improvement, despite receiving fewer treatment sessions, less relapse prevention, and less continuous care.
Conclusions
These findings contribute to the ongoing discussion as to whether or not, and to what extent, quality improvement interventions work equally well across income groups or require tailoring for specific vulnerable populations.
INTRODUCTION
Ideally, interventions to improve the quality of mental health care should be broadly effective across populations, including those with lower socioeconomic status. Quality improvement programs tailored for lower income groups have been shown to be effective. For example, cognitive behavioral therapy (CBT), antidepressants, and extensive outreach and support were effective for low income depressed Latina and African American women (1); group support and antidepressants were effective for impoverished Chilean patients (2); and medication and problem-solving therapy were effective for low income depressed patients with cancer (3). But more universal quality improvement interventions designed for broader segments of the population may or may not have equivalent effects across vulnerable subpopulations. Some universal quality improvement interventions have been shown to benefit all participants uniformly (4) and others have been shown not only to be broadly clinically effective but to have a differentially positive effect on vulnerable populations, namely ethnic minorities (5, 6). For example, Partners in Care, a primary care effectiveness quality improvement study, found greater outcome improvement for minorities than whites and reduced outcome disparities for minorities relative to whites compared to enhanced usual care, over 9 years of follow-up (1, 7, 8). Such interventions serve a dual purpose in that they improve quality broadly while, at the same time, reducing disparities in outcomes.
Attention has focused on racial or ethnic disparities but other factors that increase risk for substandard treatment, such as lower socioeconomic status, warrant further exploration. Researchers cite poverty’s contributions to the development of poor mental health, in particular the environmental toxins, food insecurity, geographic barriers to health care, violence, limited economic opportunities, crime, and increased stress. But less is known about how lower socioeconomic status impacts mental health treatment outcomes. Anxiety is more prevalent in the disadvantaged (9, 10) and poorer persons have been shown to have poorer outcomes (11, 12). Chronic economic deprivation increases levels of both anxiety and depression (13). Having fewer resources, such as funds for transportation, child care, or health insurance may also indirectly impact clinical outcomes and continued engagement in care or adherence to treatment (14-16).
Recently, we found evidence that a flexible treatment-delivery model for primary care anxiety disorders was superior to usual care (17). The Coordinated Anxiety Learning and Management (CALM) intervention, a collaborative care intervention for anxiety disorders in primary care, resulted in greater improvement in anxiety symptoms, functional disability and quality of care over 18 months relative to treatment as usual. In this paper we examine the clinical effectiveness of the CALM intervention relative to income. While more work has been done for depression, evidence for the impact of quality improvement programs for anxiety disorders on lower income populations is lacking. Our prior work with persons with panic disorder found a comparable clinical response of lower income individuals relative to higher income individuals in a collaborative care intervention (medication and CBT) over 12 months of follow-up (4). Other than this prior work, we know of no other study of quality improvement or collaborative care interventions specifically for anxiety disorders that has focused on the potentially moderating effect of income on clinical outcomes. Since our study population was relatively wealthy and about 50% of lower income patients were white, this study offers an opportunity to examine the association between incomes and clinical outcomes without substantial confounding by race. In addition, since most poorer persons receive mental health treatment in primary care rather than in specialty care settings (18), data from the CALM study are broadly relevant to the examination of lower income and clinical outcomes.
The purpose of this analysis is to examine the effect of the CALM collaborative care intervention on lower income participants relative to those with higher incomes. We hypothesized that lower income patients might show less improvement with CALM or might improve at a lower rate than higher income patients. We reasoned that they would not only be more ill at baseline but would be likely to have more continual economic stress over the course of the 12 month treatment program, placing them at risk for a less robust clinical response. On the other hand, it is also possible that lower income patients could improve at a higher rate since CALM facilitates access to evidence-based treatment, which may be less available to persons with lower incomes in the usual care group. These findings contribute to the ongoing discussion as to whether or not, and to what extent, quality improvement interventions should be universal vs. targeted or tailored for specific vulnerable populations (19).
Methods
Sample
We enrolled 1004 primary care patients with panic disorder, social anxiety disorder, generalized anxiety disorder or posttraumatic stress disorder between June 2006 and April 2008 in the Coordinated Anxiety Learning and Management (CALM) study. CALM is the largest randomized trial of collaborative care for anxiety disorders conducted to date (17, 20).
Four sites coordinated patient recruitment: University of Washington, Seattle, University of California at San Diego and Los Angeles, and the University of Arkansas for Medical Sciences at Little Rock, Arkansas. Each of the four sites selected clinics in their geographic area to participate. Candidate clinics were evaluated and 17 were purposively selected based on a number of considerations, including provider interest, space availability, size and diversity of the patient population, and insurance mix (public and private) with the goal of recruiting a diverse population of patients and clinics.
A “facilitated referral” approach was used to recruit participants. Primary care providers and clinic nursing staff directly referred potential participants. In addition, sites actively publicized the study within each clinic, allowing for self-referral. Referred participants met with a study anxiety clinical specialist to determine eligibility for CALM. Eligible participants had to be patients at one of the participating clinics, be at least 18 years old, meet DSM-IV criteria for generalized anxiety disorder, panic disorder, social anxiety disorder, or posttraumatic stress disorder (based on the Mini International Neuropsychiatric Interview (21)), score at least 8 (moderate but clinically significant anxiety symptoms on a scale ranging from 0-20) on the Overall Anxiety Severity and Impairment Scale (22), be willing to participate in CALM, and be able to provide written, informed consent. Exclusion criteria included serious alcohol or drug use (specifically, alcohol or marijuana dependence or any other drug abuse or dependence, including methadone – 4% were excluded for this reason), unstable medical conditions, marked cognitive impairment, active suicidal intent or plan, psychosis, or bipolar I disorder. Individuals already receiving ongoing CBT and persons without routine access to a telephone, or who could not speak English or Spanish were excluded.
Of 1620 patients referred and interviewed for eligibility, 1062 were eligible and, after the study procedures were explained, 1036 provided written informed consent for the study. After a baseline interview, 1004 participants were randomized to CALM or usual care using an automated computer program at RAND. The RAND Survey Research Group conducted all baseline and follow-up assessments (at 6, 12, and 18 months) by phone. Randomization was stratified by clinic and presence of co-morbid major depression using a permuted block design. Block size was masked to all clinical site study members.
Intervention Design
CALM is a flexible, collaborative care delivery model for primary care anxiety treatment that addresses any of four common anxiety disorders in primary care; provides strategies to enhance patient engagement in treatment, including allowing choice of CBT, medication, or both; and provides the option for additional treatment over the course of a year. It utilizes a web based outcomes system to optimize treatment decisions and a computer-assisted program to allow CBT-inexperienced care managers to optimize delivery of CBT and to optimize fidelity to the CBT model. Medication is prescribed by primary care physicians with care manager assistance in promoting adherence, dose optimization, and medication switches/augmentation. Although the CALM intervention was not specifically tailored for special groups of participants, an ethnicity advisory group reviewed all materials and content of the intervention to assure that it was appropriate for African-Americans, Asians, Latinos, and whites.
CALM patients initially received their preferred course of treatment over 10 to 12 weeks. The CBT program included five generic modules (education, self-monitoring, hierarchy development, breathing training, relapse prevention) and three modules (cognitive restructuring, exposure to internal and external stimuli) tailored to the four specific anxiety disorders. Patients who had multiple anxiety disorders (about 2/3 of the participants) were asked to choose the most disabling or distressing disorder to focus on within CBT with the expectation that their co-morbid disorders would also improve. CBT was administered by the care manager, called the anxiety clinical specialist. A local study psychiatrist provided single session medication management training to providers, as needed consultation by phone or e-mail, and occasionally a face-to-face assessment for complex patients. The algorithm emphasized first line use of SSRI or SNRI antidepressants, dose optimization, and side effect monitoring. If needed these were followed by second and third step combinations of two antidepressants or an antidepressant and benzodiazepine. The anxiety clinical specialist monitored adherence and related medication suggestions from the supervising psychiatrist to the primary care provider.
Patient outcomes were tracked by the anxiety clinical specialist on a web-based system. The goal was either clinical remission, defined as an anxiety scale score of <5 or sufficient improvement such that the patient did not want further treatment (23). Symptomatic patients could receive additional treatment with CBT or medication for up to twelve months. After treatment was completed, patients received monthly relapse prevention follow-up phone calls to reinforce CBT skills and/or medication adherence. Most CALM participants completed the treatment course in six months, but occasionally the course of treatment was interrupted, usually by life events or the emergence of substance abuse or dependence. Usual care patients were treated by their physicians in the usual manner which could include referral to a mental health specialist.
Measures
Mental Health Outcomes
An assessment battery was administered at baseline, 6, 12 and 18 months via telephone. The primary outcome for the secondary analyses reported here included two key components of all anxiety disorders, psychic (psychological symptoms) and somatic (physical symptoms) aspects of anxiety as measured by the Brief Symptom Inventory-12 subscales for anxiety and somatization. Lower Brief Symptom Inventory-12 scores indicate fewer symptoms. Other measures included the global mental health and physical health scales of the Medical Outcomes Study 12-Item Short-Form Health Survey (24), and the Center for Disease Control and Prevention’s (CDC) Healthy Days Measure, a single-item estimate of restricted activity days or days (in the past 30) in which poor physical or mental health kept the participant from doing usual activities (25). For the global mental health and physical health scales, higher scores indicate better functioning, while on the CDC healthy days measure, lower scores reflect better functioning.
Income
Income was assessed at baseline. We derived a dichotomous measure of high and low income by first calculating weighted average income thresholds based on Federal Poverty Guidelines (26) adjusted for family size, age of respondent and number of children less than 18 years. Family income divided by this threshold value created a poverty ratio. We divided the sample into those with incomes at or below 200%of the poverty level and those with incomes higher than this. Among CALM participants, 287 were designated low income, including 133 in the intervention group and 154 in the control group, and the remaining 717 were designated high income, including 370 in the intervention group and 347 in the control group.
Statistical Analysis
We compared baseline demographic and clinical characteristics of patients with lower and higher income using t-tests and chi-square tests for continuous and categorical variables respectively. For the longitudinal analysis of intervention effects by income group, we jointly modeled the outcomes at the four assessment times (baseline and 6, 12, and 18 month follow-ups) by study site, income, time, intervention; the two way interactions of time and intervention, income and time, income and intervention; and the three-way interaction of time, intervention and income. We fitted the models using a restricted maximum likelihood approach, which produces valid estimates under the missing-at-random assumption. This approach uses all available data to obtain unbiased estimates of model parameters. The statistical software used was SAS version 9.3. All P values were 2-tailed.
Results
Persons in the lower income group (n = 287) were younger, less educated, and less likely to have health insurance compared to those in the higher income group (n = 717) (table 1). Lower income patients tended to be sicker at baseline, as reflected by more medical and anxiety comorbidities, and had higher disability scores on both anxiety-specific (Sheehan Disability Score) and generic (global medical health scale) functioning measures, indicating poorer physical and mental functioning. While they were no more likely to meet criteria for panic disorder, generalized anxiety disorder or social anxiety disorder than higher income participants, they demonstrated a higher prevalence of both posttraumatic stress disorder and comorbid depression at baseline compared to those in the higher income group.
Table 1.
Baseline Patient Characteristics
| Participant Group | |||||||
|---|---|---|---|---|---|---|---|
|
|
|||||||
| Characteristic | Low Income | High Income | Total | ||||
| N = 287 (27.5) | N = 717 (72.5) | N = 1004 | |||||
|
| |||||||
| N | % | N | % | N | % | p-value | |
| Female | 212 | 73.9 | 502 | 70.0 | 714 | 71.1 | 0.224 |
| Education** | |||||||
| < High school | 33 | 11.5 | 22 | 3.0 | 55 | 5.5 | <0.001 |
| High school | 62 | 21.6 | 103 | 14.4 | 165 | 16.4 | |
| > High school | 192 | 66.9 | 592 | 82.6 | 784 | 78.1 | |
| Ethnicity | |||||||
| Hispanic | 61 | 21.3 | 135 | 18.8 | 196 | 19.5 | 0.068 |
| African American | 43 | 15.0 | 73 | 10.2 | 116 | 11.6 | |
| White | 146 | 50.9 | 422 | 58.9 | 568 | 56.6 | |
| Other | 37 | 12.9 | 87 | 12.1 | 124 | 12.4 | |
| Health insurance** | |||||||
| Yes | 221 | 77.3 | 640 | 89.4 | 861 | 85.9 | <0.001 |
| Number of chronic medical conditions | |||||||
| 0 | 50 | 17.4 | 153 | 21.3 | 203 | 20.2 | 0.185 |
| 1 | 58 | 20.2 | 161 | 22.5 | 219 | 21.8 | |
| ≥ 2 | 179 | 62.4 | 403 | 56.2 | 582 | 58.0 | |
| Anxiety disorder | |||||||
| Panic | 148 | 51.6 | 327 | 45.6 | 475 | 47.3 | 0.087 |
| Generalized anxiety | 214 | 74.6 | 542 | 75.6 | 756 | 75.3 | 0.733 |
| Social anxiety | 125 | 43.6 | 280 | 39.1 | 405 | 40.3 | 0.189 |
| Post-traumatic stress** | 75 | 26.1 | 106 | 14.8 | 181 | 18.0 | <0.001 |
| Major depressive disorder** | 215 | 74.9 | 433 | 60.4 | 648 | 64.5 | <0.001 |
| Number of anxiety disorders* | <0.001 | ||||||
| 1 | 99 | 34.5 | 322 | 44.9 | 421 | 41.9 | <0.001 |
| 2 | 110 | 38.3 | 277 | 38.6 | 387 | 38.6 | |
| 3-4 | 78 | 27.2 | 118 | 16.5 | 196 | 19.5 | |
| Mean | SD | Mean | SD | Mean | SD | p-value | |
| Age* | 42.25 | 14.24 | 43.96 | 13.09 | 43.47 | 13.44 | 0.048 |
| Sheehan Disability Score** a | 18.52 | 7.44 | 16.34 | 7.11 | 16.96 | 7.27 | <0.0001 |
| Global Physical Health Scale Score**b | 45.28 | 13.27 | 50.75 | 10.28 | 49.19 | 11.47 | <0.0001 |
| Global Mental Health Scale Score**b | 29.91 | 9.69 | 32.62 | 10.08 | 31.85 | 10.04 | 0.0001 |
| CDC Healthy Days Score**c | 14.28 | 10.56 | 10.14 | 9.32 | 11.30 | 9.85 | <0.0001 |
p<.05
p<.0001
Higher scores indicate greater disability
Higher scores indicate better functioning
Lower scores indicate better functioning
Figures 1-3 show baseline and follow-up predicted mean scores for low and high income patients in the CALM and usual care conditions from general linear mixed models using repeated measures for the three outcomes. In all three models, the three-way interaction of time, intervention and income was non-significant. Nor were the two-way interactions between time and income and between income and intervention significant; however the two-way interaction between time and intervention was significant in all three models (p<.0001, p<.0001 and p=.0025 respectively for Brief Symptom Inventory-12, global mental health scale, and restricted activity days).
Figure 1. Predicted Brief Symptom Inventory Scale-12 Score.
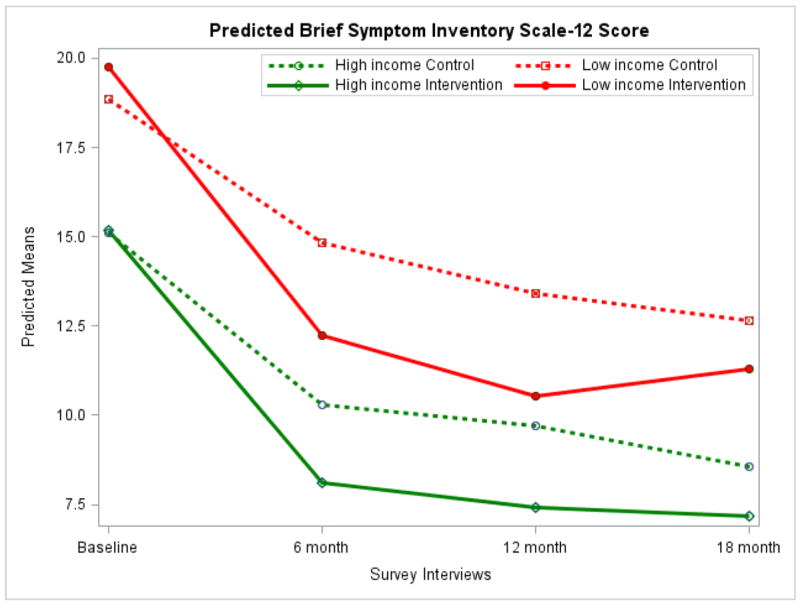
Among low income participants there was a significant difference in Brief Symptom Inventory-12 scores between intervention and control (usual care) groups at 6 (p = .012) and 12 (p = .007) months. Among high income participants there was a significant difference at 6 (p <.0001), 12 (p < .0001), and 18 (p = .031) months.
Figure 3. Predicted Restricted Activity Days Past Month.
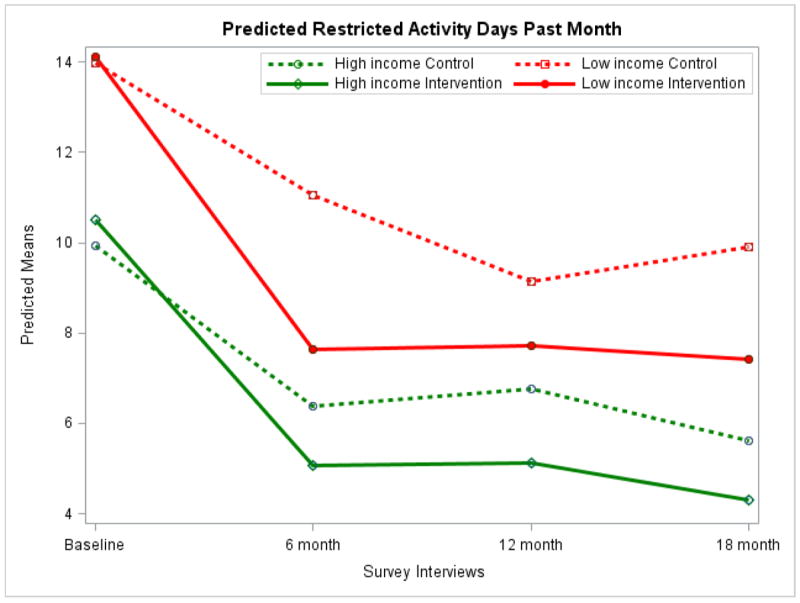
Among low income participants there was a significant difference in CDC Healthy Days score at 6 (p = .001) and 18 (p = .022) months. Among high income participants there was a significant difference at 6 (p = .047), 12 (p = .018), and 18 (p = .045) months.
Low income participants reported more symptoms at baseline on the Brief Symptom Inventory-12, regardless of whether or not they were assigned to CALM or usual care groups, than high income participants, but those low income patients assigned to CALM had higher Brief Symptom Inventory-12 scores at baseline. The CALM intervention lowered symptoms significantly more for both low and high income patients, relative to usual care over 6 and 12 months, but by 18 months there was no significant difference in Brief Symptom Inventory-12 scores between the two low-income groups (CALM vs. usual care) although the difference in Brief Symptom Inventory-12 scores between the two high income groups (CALM vs. usual care) persisted (figure 1). This may be due to fewer subjects followed in the low income group at eighteen months, especially for the CALM group. A similar pattern was seen for the global mental health scale score (figure 2), although the intervention effect was comparable and significant for both low and high income patients over all 18 months. At 6 months, the CALM intervention brought low income patients’ global mental health scale scores to the level of high income controls. The pattern for restricted activity days, shown in figure 3, is similar to the Brief Symptom Inventory-12 scores (figure 1). High income participants had fewer restricted activity days than low income participants at all times for both CALM and usual groups. There was no difference in the restricted activity days between CALM and usual care groups at baseline; however at follow-ups, the CALM group had significantly fewer restricted activity days than the usual care group for both lower and higher income groups, except at the twelve month interview for the low income group, where the difference became non-significant. Again, this may be due to fewer subjects followed in the low income group at this interview, especially for the CALM intervention group.
Figure 2. Predicted Global Mental Health Scale Score.
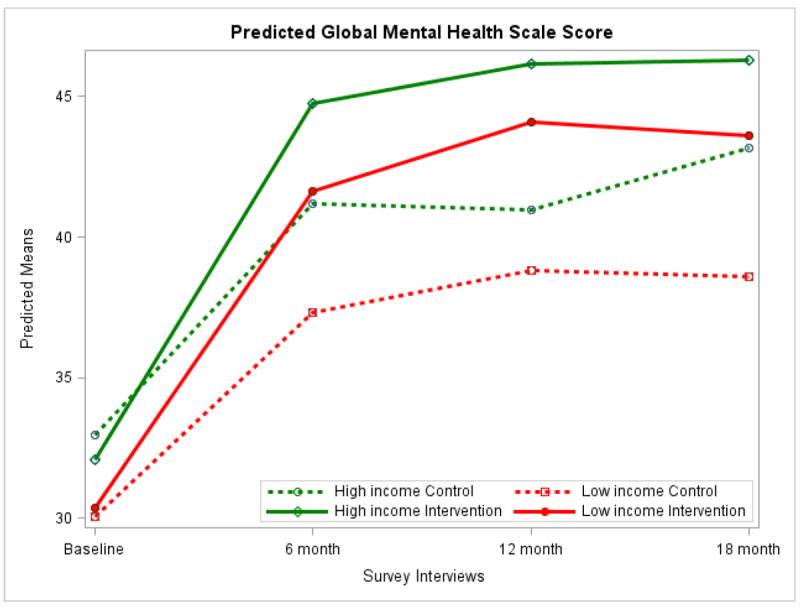
Among low income participants there was a significant difference in the Mental Health Component Scale Score at 6 (p = .002), 12 (p <.001) and 18 (p < .001) months. Among high income participants there was a significant difference at 6 (p < .0001), 12 (p < .0001), and 18 (p < .0001) months.
To examine whether or not lower income participants in the CALM intervention group differed in terms of treatment patterns, we assessed whether or not participants experienced interrupted treatment and whether they participated in the relapse prevention component of the program. (This information was available only for the intervention participants (n=503).) We also compared the number of completed CBT sessions across income groups. Lower income participants (n = 126) were significantly more likely to have interrupted treatment compared to higher income participants (n = 356) (12.7% vs. 7.0%, chi-square = 3.85; p = 0.0497); were significantly less likely to have participated in relapse prevention (61.9% vs. 72.2%, chi square = 4.65; p =0.0311); and completed fewer CBT sessions (mean=6.00 compared to mean=7.39; chi-square=10.42, p=0.0012 from Kruskal-Wallis Test). (These data were available for participants in the intervention group only.)
Discussion
As expected, lower income participants in the CALM study were more ill and disabled at baseline than those in the higher income group. At baseline, they were not only more burdened with symptoms but also more functionally impaired.
At the same time, the lower and higher income groups were very similar in terms of their clinical response to the CALM intervention, as depicted by the comparable slopes of the lines in Figures 1 - 3. The lower income participants began the study sicker and ended the study sicker than the high income group. They experienced a comparable degree of clinical improvement but the disparities related to income were not eliminated. These findings are similar to those in our previous study of collaborative care for panic disorder (4) as well as to the findings of Arean et al in the IMPACT collaborative care intervention for older adults (12). It is possible that the persistent differential in clinical outcomes across income groups results from having fewer resources available (e.g., child care, transportation) to assure continued access to treatment. But it could also relate to differential beliefs or attitudes about the relevance of CBT given very realistic life stressors in the lower income group. Regardless of the explanation, it is quite conceivable that had the lower income group received comparable numbers of CBT sessions, relapse prevention, and continuous care, they may have had a more robust clinical response relative to those with higher incomes.
Most participants in the CALM study completed treatment within the initial 6 month period but could be actively followed by the study clinicians for 12 months, after which they received only one follow-up assessment by phone from the survey group but no clinical interventions. Therefore, one might expect the greatest clinical response to occur at 6 months and to potentially deteriorate after that point, a pattern reflected in our data. However, given that the lower income group would continue to be subject to more economic stress, it may be especially remarkable that the lower income group did not experience significantly greater deterioration of clinical improvements after 6 months relative to the high income participants. This suggests that the effect of the CALM intervention was sustained equally well across participants regardless of income level and in spite of presumed differences in treatment intensity and continuity, at least over the first 12 months. This is in contrast to a recently reported depression intervention for low income women with co-morbid cancer in which marked recurrence of depression occurred post-intervention (3).
Our study suggests that if the goal is to obtain an equivalent clinical response across lower and higher income patients, clinic-based collaborative care for anxiety disorders as delivered in the CALM study is adequate and effective. It is possible, however, that the low income group might have benefited to a greater extent from tailored supplements to treatment, such as assistance with transportation or child care or even novel delivery approaches, such as treatment delivered in the home. Providing such features for lower income participants might be more likely to result in an intervention that not only improves quality of care but also even further reduces disparities in clinical outcomes. Studies are needed to address significant barriers to building collaborative care teams in safety net care populations, including approaches to facilitate communication across mental health and medical providers via newer health technologies.
Limitations
Because CALM participants were recruited from primary care settings, most had health insurance and the resources needed to get to the primary care clinics. Before entering the CALM study, 57% of participants were already receiving medication, much of it clinically appropriate. Hence, participants represent a select group that had failed to improve with first line medication treatment administered by the primary care provider. Participants as a whole were better off economically than many segments of the population who may not have ready access to primary care or who may live in even more stressful living situations in which meeting daily needs for survival are paramount. Our findings, therefore, should not be interpreted as applying to all groups of lower income persons. In addition, while the study used common and widely-accepted outcome measures, these measures capture symptoms at only one point in time and may, therefore, fail to reflect the often episodic nature of anxiety disorders.
In conclusion, this analysis illustrates that a collaborative care intervention for anxiety in primary care worked equally well for those with lower and higher incomes but did not eliminate baseline disparities in mental health status associated with economic disadvantage. Our findings should reduce the tendency to be nihilistic about the impact of mental health treatments for lower income individuals. Even when treatments were delivered with less intensity and frequency than desirable, clear and meaningful benefits were obtained.
Acknowledgments
Funding: This work was supported by the following grants from the National Institute of Mental Health: U01 MH057858 and K24 MH065324 (Dr. Roy-Byrne), U01 MH058915 (Dr. Craske), U01 MH070022 (Dr. Sullivan), U01 MH070018 (Dr. Sherbourne), U01MH057835 and K24 MH64122 (Dr. Stein); and from the National Institutes of Health, 1UL1RR029884 (Dr. Sullivan).
Footnotes
Disclosures: Dr Roy-Byrne has received research grant support from the National Institutes of Health; has served as Editor-in-Chief for Journal Watch Psychiatry (Massachusetts Medical Society), Depression and Anxiety (Wiley -Liss Inc), and UpToDate Psychiatry; and is a consultant for Valant Medical Solutions (Behavioral health EMR company). Dr Roy-Byrne has also provided legal consultation on multiple legal cases related to depression, anxiety and posttraumatic stress disorder.
Dr. Stein has received research support from the US Department of Defense, Eli Lilly and Company, GlaxoSmithKline, Hoffmann-La Roche, National Institutes of Health, and the US Veterans Affairs Research Program. Dr. Stein is currently or has been a paid consultant for AstraZeneca, Avera Pharmaceuticals, BrainCells Inc, Bristol-Myers Squibb, Comprehensive NeuroScience, Eli Lilly and Company, Forest Laboratories, GlaxoSmithKline, Hoffman-La Roche Pharmaceuticals, Jazz Pharmaceuticals, Johnson & Johnson, Mindsite, Pfizer, Sepracor, and Transcept Pharmaceuticals Inc.
Bibliography
- 1.Miranda J, Chung JY, Green BL, Krupnick J, Siddique J, Revicki DA, Belin T. Treating depression in predominantly low-income young minority women: a randomized controlled trial. JAMA. 2003;290(1):57–65. doi: 10.1001/jama.290.1.57. [DOI] [PubMed] [Google Scholar]
- 2.Araya R, Rojas G, Fritsch R, Gaete J, Rojas M, Simon G, Peters TJ. Treating depression in primary care in low-income women in Santiago, Chile: a randomised controlled trial. Lancet. 2003;361(9362):995–1000. doi: 10.1016/S0140-6736(03)12825-5. [DOI] [PubMed] [Google Scholar]
- 3.Ell K, Xie B, Kapetanovic S, Quinn DI, Lee PJ, Wells A, Chou CP. One-year follow-up of collaborative depression care for low-income, predominantly Hispanic patients with cancer. Psychiatr Serv. 2011;62(2):162–70. doi: 10.1176/ps.62.2.pss6202_0162. [DOI] [PubMed] [Google Scholar]
- 4.Roy-Byrne P, Sherbourne C, Miranda J, Stein M, Craske M, Golinelli D, Sullivan G. Poverty and response to treatment among panic disorder patients in primary care. Am J Psychiatry. 2006;163(8):1419–25. doi: 10.1176/ajp.2006.163.8.1419. [DOI] [PubMed] [Google Scholar]
- 5.Wells KB, Sherbourne C, Schoenbaum M, Duan N, Meredith L, Unutzer J, Miranda J, Carney MF, Rubenstein LV. Impact of disseminating quality improvement programs for depression in managed primary care: a randomized controlled trial. JAMA. 2000;283(2):212–20. doi: 10.1001/jama.283.2.212. [DOI] [PubMed] [Google Scholar]
- 6.Druss BG, Zhao L, von Esenwein SA, Bona JR, Fricks L, Jenkins-Tucker S, Sterling E, Diclemente R, Lorig K. The Health and Recovery Peer (HARP) Program: a peer-led intervention to improve medical self-management for persons with serious mental illness. Schizophr Res. 2010;118(1-3):264–70. doi: 10.1016/j.schres.2010.01.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wells K, Sherbourne C, Schoenbaum M, Ettner S, Duan N, Miranda J, Unutzer J, Rubenstein L. Five-year impact of quality improvement for depression: Results of a group-level randomized controlled trial. Arch Gen Psychiatry. 2004;61(4):378–86. doi: 10.1001/archpsyc.61.4.378. [DOI] [PubMed] [Google Scholar]
- 8.Wells KB, Sherbourne CD, Miranda J, Tang L, Benjamin B, Duan N. The cumulative effects of quality improvement for depression on outcome disparities over 9 years: results from a randomized, controlled group-level trial. Med Care. 2007;45(11):1052–9. doi: 10.1097/MLR.0b013e31813797e5. [DOI] [PubMed] [Google Scholar]
- 9.Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51(1):8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- 10.Bruce M, Lader M. DSM-III-R state anxiety symptoms in anxiety disorder patients. Biol Psychiatry. 1991;30(5):519–22. doi: 10.1016/0006-3223(91)90316-e. [DOI] [PubMed] [Google Scholar]
- 11.Murphy JM, Olivier DC, Monson RR, Sobol AM, Federman EB, Leighton AH. Depression and anxiety in relation to social status. A prospective epidemiologic study. Arch Gen Psychiatry. 1991;48(3):223–9. doi: 10.1001/archpsyc.1991.01810270035004. [DOI] [PubMed] [Google Scholar]
- 12.Arean PA, Gum AM, Tang L, Unutzer J. Service use and outcomes among elderly persons with low incomes being treated for depression. Psychiatr Serv. 2007;58(8):1057–4. doi: 10.1176/ps.2007.58.8.1057. [DOI] [PubMed] [Google Scholar]
- 13.Jagannathan R, Camasso MJ, Sambamoorthi U. Experimental evidence of welfare reform impact on clinical anxiety and depression levels among poor women. Soc Sci Med. 2010;71(1):152–60. doi: 10.1016/j.socscimed.2010.02.044. [DOI] [PubMed] [Google Scholar]
- 14.Bisgaier J, Rhodes KV. Cumulative adverse financial circumstances: associations with patient health status and behaviors. Health Soc Work. 2011;36(2):129–37. doi: 10.1093/hsw/36.2.129. [DOI] [PubMed] [Google Scholar]
- 15.Copeland VC, Snyder K. Barriers to mental health treatment services for low-income African American women whose children receive behavioral health services: an ethnographic investigation. Soc Work Public Health. 2011;26(1):78–95. doi: 10.1080/10911350903341036. [DOI] [PubMed] [Google Scholar]
- 16.Mojtabai R, Olfson M, Sampson NA, Jin R, Druss B, Wang PS, Wells KB, Pincus HA, Kessler RC. Barriers to mental health treatment: results from the National Comorbidity Survey Replication. Psychol Med. 2011;41(8):1751–61. doi: 10.1017/S0033291710002291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Roy-Byrne P, Craske MG, Sullivan G, Rose RD, Edlund MJ, Lang AJ, Bystritsky A, Welch SS, Chavira DA, Golinelli D, Campbell-Sills L, Sherbourne CD, Stein MB. Delivery of evidence-based treatment for multiple anxiety disorders in primary care: a randomized controlled trial. JAMA. 2010;303(19):1921–8. doi: 10.1001/jama.2010.608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.U.S. Department of Health and Human Services. Mental Health: Culture, Race, and Ethnicity--A Supplement to Mental Health: A Report of the Surgeon General. Rockville, MD: Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services; 2001. [Google Scholar]
- 19.Lau AS. Making the case for selective and directed cultural adaptations of evidence-based treatments: examples from parent training. Clin Psychol Sci Prac. 2006;13:295–310. [Google Scholar]
- 20.Sullivan G, Craske MG, Sherbourne C, Edlund MJ, Rose RD, Golinelli D, Chavira DA, Bystritsky A, Stein MB, Roy-Byrne PP. Design of the Coordinated Anxiety Learning and Management (CALM) study: Innovations in collaborative care for anxiety disorders. Gen Hosp Psychiatry. 2007;29(5):379–87. doi: 10.1016/j.genhosppsych.2007.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(Suppl 20):22–33. [PubMed] [Google Scholar]
- 22.Campbell-Sills L, Norman SB, Craske MG, Sullivan G, Lang AJ, Chavira DA, Bystritsky A, Sherbourne C, Roy-Byrne P, Stein MB. Validation of a brief measure of anxiety-related severity and impairment: the Overall Anxiety Severity and Impairment Scale (OASIS) J Affect Disord. 2009;112(1-3):92–101. doi: 10.1016/j.jad.2008.03.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stein MB, Roy-Byrne PP, Craske MG, Campbell-Sills L, Lang AJ, Golinelli D, Rose RD, Bystritsky A, Sullivan G, Sherbourne CD. Quality of and patient satisfaction with primary health care for anxiety disorders. J Clin Psychiatry. 2011 doi: 10.4088/JCP.09m05626blu. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Ware JE, Kosinski M, Bowker D, Gandek B. How to Score Version 2 of the SF-12 Health Survey (with a Supplement Documenting Version 1) Lincoln, RI: Quality Metric Incorporated; 2002. [Google Scholar]
- 25.Moriarty DG, Zack MM, Kobau R. The Centers for Disease Control and Prevention’s Healthy Days Measures - population tracking of perceived physical and mental health over time. Health Qual Life Outcomes. 2003;1:37. doi: 10.1186/1477-7525-1-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.U.S. Census Bureau. Poverty. [2012 August 10];2012 Available from: www.census.gov/hhes/www/poverty/poverty.html.