

Abstract
Laparoscopic cholecystectomy has become the standard treatment for symptomatic cholelithiasis in patients with situs inversus totalis (SIT). In an effort to reduce morbidity and improve the cosmesis single-port laparoscopic cholecystectomy has recently emerged, where the surgery is done through a single port, typically the patient's navel. This improves the cosmesis, lessens post-operative pain and ensures virtually a “scar less” surgery. We report a case of successful single-port laparoscopic cholecystectomy for a patient with SIT, and describe its technical advantages and review of literature.
Keywords: Cholelithiasis, glove port, laparoscopic cholecystectomy, single incision laparoscopic surgery, situs inversus totalis, single port cholecystectomy
INTRODUCTION
Situs inversus totalis (SIT) is a rare congenital disorder, found in just 0.005% to 0.01% of the population.[1,2]
Laparoscopic cholecystectomy is today widely accepted as the treatment of choice for symptomatic cholelithiasis in patients with situs inversus.[3,4,5] However, the laparoscopic treatment may have technical difficulties because of the mirror-image anatomy.
Herein, we present a case of single port laparoscopic cholecystectomy in a SIT, discuss the technical aspects, and describe the role of E.K. glove port[6] as the access port.
CASE REPORT
A 65-year-old man presented with 1-year history of intermittent epigastric and left upper quadrant discomfort and concomitant digestive problems. Abdominal ultrasonography revealed gallstones, and that the liver and gallbladder were located in the left upper quadrant, whereas the spleen and stomach were located on the right side. A pre-operative chest X-ray showed dextrocardia [Figure 1]. Laboratory data were normal. After obtaining the patient's informed consent, surgery was performed.
Figure 1.
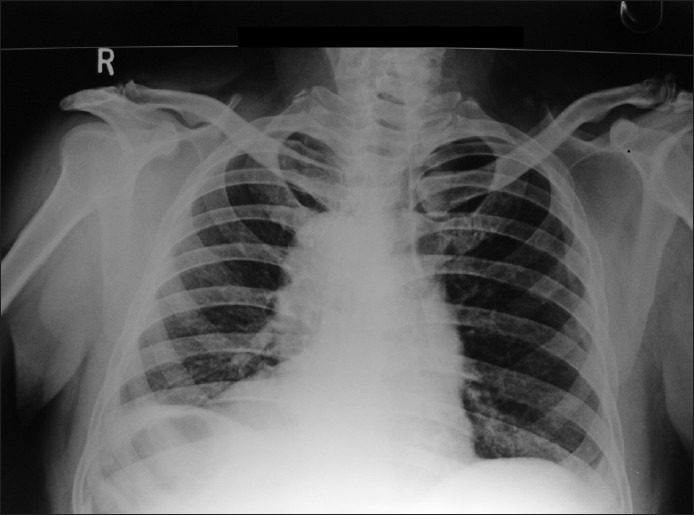
Chest X-Ray Showing dextrocardia
The patient underwent general anaesthesia and was positioned supine on the operating table. The surgeon stood on the right side of the patient with the assistant on the left side of the surgeon. The scrub nurse and the monitor were on the left side of the patient [Figure 2]. A standard 10 mm, 30o angled rigid laparoscope with a vertical light cable was used. One articulating laparoscopic grasper (roticulator endo grasp, Covidien), for the left hand and standard rigid 5 mm laparoscopic instruments for the right hand were used in this operation.
Figure 2.

Position of the surgical team and the E.K. Glove port in the umbilicus
A 2.5 cm completely intra-umbilical, vertical skin incision was performed. The incision was deepened to enter the peritoneal cavity. The inner flexible ring, fitted with the glove was then introduced into the abdomen. The open end of the glove was then wrapped around the outer rigid ring [Figure 3]. Co2 pneumoperitoneum was induced and the patient was then put in reverse Trendelenburg position and tilted slightly right laterally for the remainder of the procedure.
Figure 3.

Construction of the E.K. Glove port
SIT was confirmed with the telescope inserted via the E.K. Glove port[6] in the umbilicus. The liver and the gallbladder were confirmed to be on the left-side [Figure 4a], whereas the spleen, the stomach and the heart beat were seen on the right.
Figure 4.
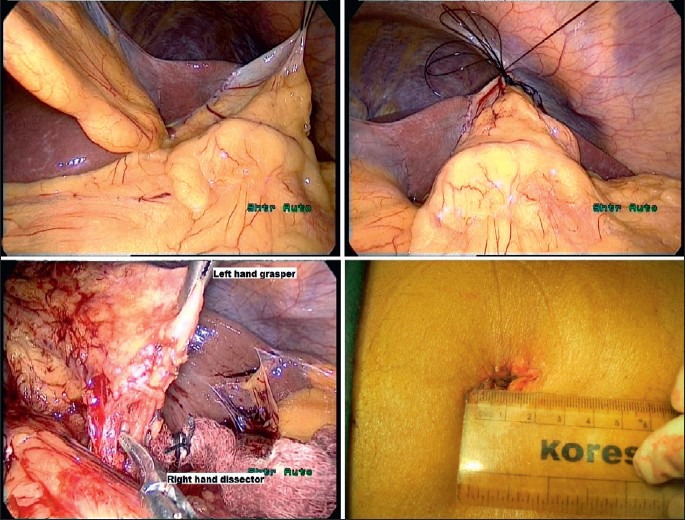
(a) Intra operative picture showing gall bladder covered with adhesions on left of Ligamentum Teres (b) Ethilon suture used as the fundal retractor (c) Dissection at the Calot's triangle (d) Skin closed with vicryl rapide
A tuft or bun was made with the tail end of the No.1-0 nylon suture. The needle was passed through the fundus of the gall bladder, care being taken to pass the needle through the serosa without puncturing the lumen. It was next passed through the peritoneum below the diaphragm. The needle was then brought out through the left subcostal region. When the thread was pulled from outside and fixed with a haemostat, a good retraction of the gallbladder imitating retraction accordance to conventional technique for safe cholecystectomy was achieved [Figure 4b]. The entire gallbladder, except for the fundus was covered with dense adhesions, which were lysed using the Maryland grasper and monopolar diathermy current. The cystic artery and duct were identified, dissected [Figure 4c] and clipped with 10 mm clip applicators separately and divided with a pair of scissors.
Next, the gallbladder was grasped with the left hand grasper and retracted in various directions so that it could be dissected from the liver bed by hook electrocautery in an infundibulum-to-fundal direction.
The specimen was retrieved through the E.K. Glove port.[6] The fascial defect was closed using 1-0 Prolene (Ethicon) and the skin was approximated using 3-0 polyglycolic Rapide suture (Ethicon) [Figure 4d]. The procedure took 70 min and the operative blood loss was minimal. Our patient had an uneventful post-operative course and was discharged on the second post-operative day. Pathologic examination confirmed cholelithiasis with chronic cholecystitis. The patient was followed up and has remained well.
DISCUSSION
In the published literature, there have only been about 40 reports of standard laparoscopic cholecystectomy in patients with situs inversus.[7] The most challenging factor for performing laparoscopic cholecystectomy in patients with situs inversus is the “mirror image” anatomy. This uninvited condition, together with the two- dimensional effect of laparoscopy may lead to some problems in orientation and dissection during the procedure with the possibility to high-risk of iatrogenic injuries.[4]
In an effort to reduce morbidity and improve the cosmesis of laparoscopic surgery, single port surgery has recently emerged, which improves the cosmesis, lessens post-operative pain and ensures virtually a “scar less” surgery. A comprehensive search of the PubMed and Google scholar was performed in October 2012 using medical subject headings ‘cholecystectomy, laparoscopic’ and “situs inversus.” There are only four published report on single-incision or single port laparoscopic cholecystectomy in patient with SIT[1,2,7,8] [Table 1]. Of these, two are males and two females. The age group is from 45 to 65 years. Han et al. first published a single-incision laparoscopic cholecystectomy in a patient with SIT in 2011.[1,2] They used the Alexis wound retractor and a glove as the access port. Uludag et al.[7] and Ozsoy et al.[8] used the “SILS port®” (Covidien) to perform the surgery whereas de Campos et al.[1] used the ‘SITRACC Port’ to complete the surgery. In the present study, we employed the E.K. Glove port as the access port. This improvised E.K. glove port[6] is very cheap in comparison to the commercially available single port access system and is more cost effective than the home made transumbilical port where an Alexis wound retractor® is required.
Table 1.
Publications on situs inversus and single port/single incision cholecystectomy

Although, standard laparoscopic cholecystectomy in SIT poses some technical difficulties for right-handed surgeons, single port cholecystectomy confers some advantages for dissection with the right-hand.[7] Using the innovative E.K. Glove port[6] and a roticulator in the left-hand, with the surgeons positioned on the right-side of the patient, an advantageous observation was that, neither the working elements nor the hands of the surgeon crossed at any point of time during the surgery.
In conclusion, single-port laparoscopic cholecystectomy in SIT is feasible and a safe procedure in a specialist setting. The procedure can be safely completed with proper training and careful planning.
Footnotes
Source of Support: None
Conflict of Interest: None declared.
REFERENCES
- 1.de Campos Martins MV, Falcão JL, Skinovsky J, de Faria GM. Single-port cholecystectomy in a patient with situs inversus totalis presenting with cholelithiasis: A case report. J Med Case Rep. 2012;6:96. doi: 10.1186/1752-1947-6-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Han HJ, Choi SB, Kim CY, Kim WB, Song TJ, Choi SY. Single-incision multiport laparoscopic cholecystectomy for a patient with situs inversus totalis: Report of a case. Surg Today. 2011;41:877–80. doi: 10.1007/s00595-010-4387-9. [DOI] [PubMed] [Google Scholar]
- 3.Pitiakoudis M, Tsaroucha AK, Katotomichelakis M, Polychronidis A, Simopoulos C. Laparoscopic cholecystectomy in a patient with situs inversus using ultrasonically activated coagulating scissors. Report of a case and review of the literature. Acta Chir Belg. 2005;105:114–7. [PubMed] [Google Scholar]
- 4.Aydin U, Unalp O, Yazici P, Gurcu B, Sozbilen M, Coker A. Laparoscopic cholecystectomy in a patient with situs inversus totalis. World J Gastroenterol. 2006;12:7717–9. doi: 10.3748/wjg.v12.i47.7717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Patle NM, Tantia O, Sasmal PK, Khanna S, Sen B. Laparoscopic cholecystectomy in situs inversus-our experience of 6 cases. Indian J Surg. 2010;72:391–4. doi: 10.1007/s12262-010-0159-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Khiangte E, Newme I, Phukan P, Medhi S. Improvised transumbilical glove port: A cost effective method for single port laparoscopic surgery. Indian J Surg. 2011;73:142–5. doi: 10.1007/s12262-010-0215-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Uludag M, Yetkin G, Kartal A. Single-incision laparoscopic cholecystectomy in situs inversus totalis. JSLS. 2011;15:239–43. doi: 10.4293/108680811X13071180407032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ozsoy M, Haskaraca MF, Terzioglu A. Single incision laparoscopic cholecystectomy (SILS) for a patient with situs inversus totalis. BMJ Case Rep 2011. 2011;28:2011. doi: 10.1136/bcr.08.2011.4581. [DOI] [PMC free article] [PubMed] [Google Scholar]