

Abstract
The current decade has witnessed the evolution of Minimal Access Surgery (MAS) from Multi port Laparoscopy to Single Port Laparoscopy. The reduction of ports, subsequent scars and pain makes MAS more patients friendly. Symptomatic Subxiphoid Incisional hernias in patients having post CABG Sternotomy are surgically challenging. This is because of the difficult anatomical position i.e. sternum and the ribs superiorly and the diaphragm posteriorly. Another reason is high intra-abdominal pressure with the shearing forces of the musculature in the upper abdomen. Consequently the conventional open primary anatomical or mesh repairs are difficult to perform and have a high recurrence rate. Laparoscopy promises to be an effective technique to treat this condition. In this case report we describe the use of Laparoscopy in particular: Single Incision for the repair of CABG Sternotomy Subxiphoid Hernia along with relevant literature. This is the first report in English Language Literature.
Keywords: Incisional Hernia, intra peritoneal onlay mesh, Post CABG Sternotomy, single incision laparoscopic surgery, sub xiphoid hernia
INTRODUCTION
Now a days with an increase in the number of CABGs, the incidence of Subxiphoid Incisional hernia after median Sternotomy is on the rise. The precise incidence is not known, but the reported incidence is 1% to 4.2%.[1,2,3] The repair of Subxiphoid hernia is a difficult procedure which results in a high rate of recurrence. Laparoscopic approach is a promising new technique for more efficacious treatment of this condition.[2] In this case report we describe the use of Single Incision Laparoscopy for the repair of Post CABG Subxiphoid Hernia as Single Incision. Such Transumbilical Single Incision minimises surgical invasion without compromising accessibility, exposure and operating time. It also almost completely abolishes post-operative pain and ensures early ambulation.
CASE REPORT
Our patient: Male, 65 yrs; BMI 28; 4 yrs post CABG presented with a painful, increasing Subxiphoid Hernia. [Figure 1]. CT scan was done in view of the unusual hernia site to rule out thoracic defect (diaphragm) and the defect was 4cm × 4cm [Figure 2]. Under Combined General Epidural Anaesthesia the hernia was repaired with Transumbilical Single Incision Intra Peritoneal Onlay Dual layered Meshplasty with four transfascial sutures and absorbable tacks for mesh fixation. A Covidien SILS port [Figure 3] and standard laparoscopic straight instruments [Figure 4] were used for hernioplasty. The transfacial sutures were placed as follows: just below the xiphoid process, in the right and left subcostal region and above the umbilicus.
Figure 1.

Post cabg subxiphoid incisional hernia
Figure 2.
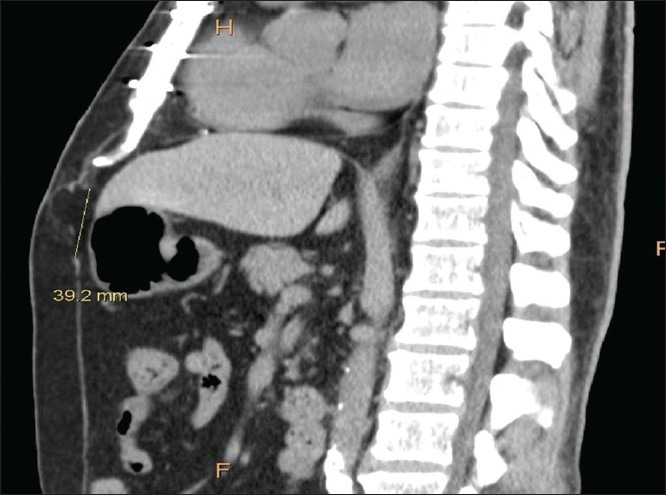
Computed tomogram
Figure 3.

Single incision port
Figure 4.
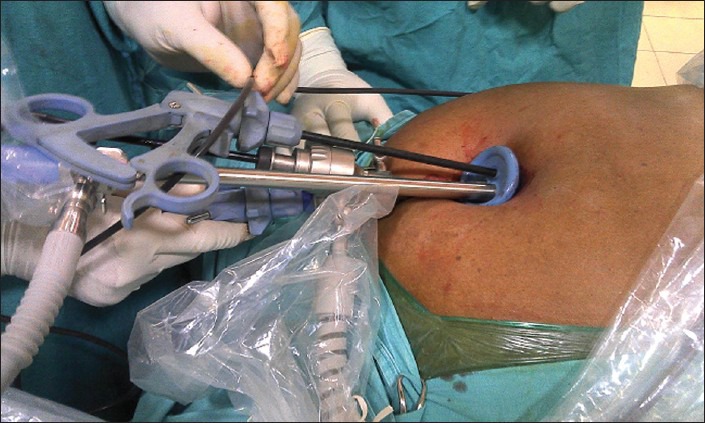
2.5-cm single transumbilical port
In between the transfascial sutures [Figure 5], the mesh was secured with 5 mm absorbable tacks [Figure 6]. The total operative time for the hernioplasty was 40 minutes.
Figure 5.

Suture passer
Figure 6.

Absorbable tacks
DISCUSSION
Post-strenotomy sub-xiphoid incisional hernia is uncommon and is a difficult location for hernia repair like the Flank and Suprapubic Hernias. The hernia defect is located in the caudad portion of the Sternotomy, where the incision enters the epigastrium. The defect is relatively protected from intestinal incarceration by the anterior surface of the liver.
Factors predisposing this area to herniation include lateral traction forces on the abdominal wall,[2] male sex, obesity, postoperative wound infection, and left heart failure.[1] As with all hernias, operative repair of Subxiphoid hernias is indicated for symptoms or incarceration. Due to its anatomical position in the epigastrium, open hernia repair is cumbersome.[2] Adequate exposure of the hernia and mesh placement usually requires dissection of the falciform ligament. Securing the mesh in this region is especially difficult due to the proximity of the ribs, diaphragm, and central tendon of the diaphragm. Abdominal pressure secures the mesh and adds strength to the repair, and the left lobe of the liver and stomach make this region relatively protected. Conventional open primary repair of abdominal wall hernias has a high recurrence rate. A recurrence rate of 43% to 80% has been reported with primary midline reapproximation of the fascia. Proper placement of mesh requires dissection of the retro-xiphoid space to allow a subfascial position and adequate overlap [Figure 7]. The laparoscopic approach to repair of Subxiphoid epigastric hernias has been described in few reports in the literature with good success.[1,2,3] Laparoscopy is useful because it allows for excellent sub fascial visualization of the epigastrium and edges of the defect, avoidance of the previous incision and minimal tissue trauma. As with all laparoscopic ventral hernia repairs, proper fixation of the mesh depends on the use of both transfascial sutures [Figure 5] and absorbable tacks [Figure 6]. The use of only a 2.5-cm Single Transumbilical Incision [Figure 4] further minimizes surgical invasion without compromising on the surgical accessibility, exposure, technique or increasing the time of surgery [Figure 7]. The use of Combined General Epidural Anaesthesia here was advantageous as it decreases the requirement of anaesthetic agent and ensures better post-operative analgesia and early ambulation decreases thromboembolic, cardiac, pulmonary and gastrointestinal postoperative morbidity. The patient returned early to work.[5]
Figure 7.

Final look
CONCLUSION
Post CABG Sub xiphoid hernioplasty is undoubtedly better managed by Laparoscopy than by Open Surgery. Laparoendoscopic Single Site Surgery is definitely cosmetically better and less invasive than Multiport Laparoscopy for this kind of hernia repair.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Davidson BR, Bailey JS. Incisional herniae following median Sternotomy incisions: Their incidence and aetiology. Br J Surg. 1986;73:995–6. doi: 10.1002/bjs.1800731216. [DOI] [PubMed] [Google Scholar]
- 2.Landau O, Raziel A, Matz A, Kyzer S, Haruzi I. Laparoscopic repair of poststernotomy subxiphoid epigastric hernia. Surg Endosc. 2001;15:1313–4. doi: 10.1007/s004640090011. [DOI] [PubMed] [Google Scholar]
- 3.Mackey RA, Brody FJ, Berber E, Chand B, Henderson JM. Subxiphoid incisional hernias after median sternotomy. J Am Coll Surg. 2005;201:71–6. doi: 10.1016/j.jamcollsurg.2005.01.025. [DOI] [PubMed] [Google Scholar]
- 4.Cohen MJ, Starling JR. Repair of Subxiphoid Incisional hernia with Marlex mesh after median Sternotomy. Arch Surg. 1985;120:1270–1. doi: 10.1001/archsurg.1985.01390350052011. [DOI] [PubMed] [Google Scholar]
- 5.Eldor J. Combined spinal-epidural-general anesthesia. Med Hypotheses. 1995;45:86–90. doi: 10.1016/0306-9877(95)90209-0. [DOI] [PubMed] [Google Scholar]