

Abstract
Germ cell tumors may lead to incomplete isosexual male precocity and are commonly located in the pineal gland. Germinomas of the basal ganglia are almost always unilateral and precocious puberty is a rare manifestation in them. We report a 9.5-year-old boy who presented with incomplete isosexual precocity due to bilateral basal ganglia germinoma.
Keywords: Basal ganglia germinoma, precocious puberty
INTRODUCTION
Germ cell tumors secreting human chorionic gonadotropin (hCG) may lead to incomplete isosexual precocity in boys. Germinomas account for approximately two-thirds of germ cell tumors and usually develop in the midline at the pineal and suprasellar regions.[1,2] However, they may rarely arise from “ectopic sites” most notably the basal ganglia and thalamus when they usually present with gradually progressive hemiparesis and are almost always unilateral.[1,2]
CASE REPORT
A 9.5-year-old boy presented with enlargement of penis and appearance of pubic hair for 1 year and breaking of voice for 6 months. There was no history suggestive of raised intracranial tension and no history of head trauma, radiation exposure, cranial surgery or seizure. He was the first born child of a non-consanguineous union and had a younger brother who was healthy. He had a normal perinatal and developmental history had no history of any central nervous system infection or androgen exposure and his family history was non-contributory.
On examination, his height was 124.4 cm (standard deviation score [SDS] – 1.7), weight was 24.8 kg (SDS – 1.3) and his target height was 156.4 cm (SDS – 2.9). Testes were 5 ml in volume each and were firm, symmetric and without any irregularity. SPL was 8 cm and pubic hair was tanner stage 4 [Figure 1]. Examination of other systems including a detailed examination of the nervous system (with fundoscopic examination) revealed no abnormality.
Figure 1.

External genitalia and pubic hair suggestive of puberty
Biochemical tests showed an elevated testosterone (637 ng/dl) with prepubertal basal luteinizing hormone (LH) (0.128 mIU/ml) and post decapeptyl LH levels (30 min = 0.325 mIU/ml and 60 min = 0.334 mIU/ml) and a bone age of 12 years. Serum β-hCG was elevated (22.47 mIU/ml; normal = non-detectable to 5.3 mIU/ml) while 17-hydroxyprogesterone was normal (1.96 ng/ml). Ultrasonography of the abdomen and testes and chest X-ray were normal. Gadolinium contrast enhanced magnetic resonance imaging (MRI) revealed an ill-defined, heterogenous patchy enhancing lesion in bilateral basal ganglia with minimal compression and contralateral diaplacement of the third ventricle [Figures 2 and 3]. Cerebrospinal fluid (CSF) β-hCG was elevated (47.9 miU/ml; normal = non-detectable to 5.3 mIU/ml) but α-fetoprotein was normal (0.02 IU/ml; normal = 0-5.5). The next investigative step entailed a biopsy of the lesion, which could not be done in our institution for logistic reasons.
Figure 2.
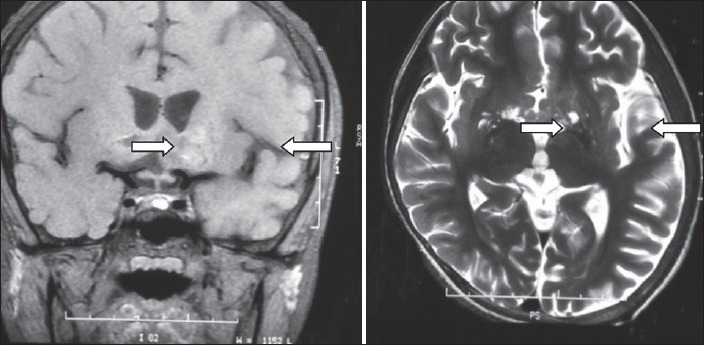
T1W coronal and T2W axial magnetic resonance imaging showing ill-defined, heterogeneous hyperintense lesion in bilateral basal ganglia
Figure 3.
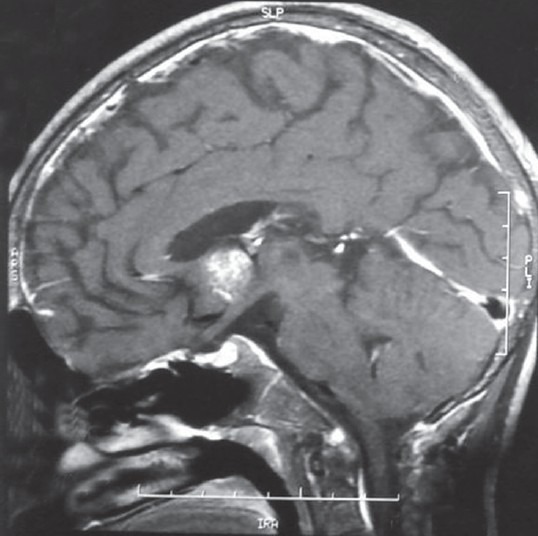
Gd-contrast sagittal magnetic resonance imaging showing heterogeneous patchy uptake in lesion in basal ganglia
He was diagnosed to have isosexual precocity due to germ cell tumor involving bilateral basal ganglia, which in all likelihood was a germinoma and was referred to a specialty oncology institute. He received conformal radiotherapy following which serum testosterone dropped down to 137 ng/dl and MRI showed a slight decrease in the size of the lesion [Figure 4].
Figure 4.
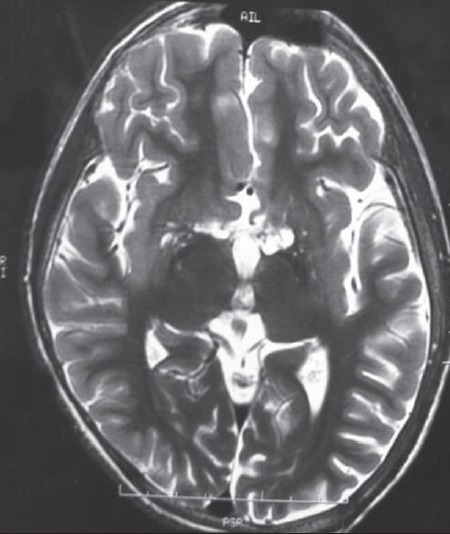
Post-radiotherapy T2W axial magnetic resonance imaging showing slight reduction in lesion
The germ cell tumor was most likely a germinoma considering the age group, location, absence of elevated CSF α-fetoprotein and response to radiotherapy.
DISCUSSION
Incomplete isosexual precocity in males may occur due to hCG secretion from intracranial germ cell tumors, which constitutes 2% of primary intracranial neoplasms below 20 years of age.[3] Of the non-midline germ cell tumors, those arising within the basal ganglia are most often germinomas.[4] The usual sites of intracranial germinoma are the pineal and suprasellar region and location in the basal ganglia is very rare occurring in only 5-10% of cases.[1,2] A higher incidence of basal ganglia germinoma is seen in Asian populations occurring in patients aged 7-20 years with a striking male predominance (20:1).[1] The major signs and symptoms include progressive hemiparesis, cognitive decline and psychosis with precocious puberty being a rare, atypical manifestation.[1] Signs of raised intracranial pressure are usually not present as these tumors are non-invasive and do not obstruct the ventricular system.[5] The clinical course is usually slow, with the duration of clinical symptoms ranging from 1 month to 4.5 years and diagnosis at an early stage is extremely difficult.[1] In this regard, our patient could be considered lucky as his atypical presentation led to the diagnosis of his condition before more sinister neurologic manifestations could creep in. An early diagnosis in this condition is of prime importance on account of its excellent response to radiotherapy and chemotherapy. There are only a handful of case reports of bilateral basal ganglia germinoma and only a single report of it presenting with precocious puberty in published medical literature.[6] This is only the 2nd report of bilateral basal ganglia germinoma presenting with precocious puberty and as providence would have it, his sexual precocity proved to be a blessing in disguise!.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Tamaki N, Lin T, Shirataki K, Hosoda K, Kurata H, Matsumoto S, et al. Germ cell tumors of the thalamus and the basal ganglia. Childs Nerv Syst. 1990;6:3–7. doi: 10.1007/BF00262257. [DOI] [PubMed] [Google Scholar]
- 2.Kim DI, Yoon PH, Ryu YH, Jeon P, Hwang GJ. MRI of germinomas arising from the basal ganglia and thalamus. Neuroradiology. 1998;40:507–11. doi: 10.1007/s002340050634. [DOI] [PubMed] [Google Scholar]
- 3.Kim CH, Paek SH, Park IA, Chi JG, Kim DG. Cerebral germinoma with hemiatrophy of the brain: Report of three cases. Acta Neurochir (Wien) 2002;144:145–50. doi: 10.1007/s007010200017. [DOI] [PubMed] [Google Scholar]
- 4.Jennings MT, Gelman R, Hochberg F. Intracranial germ-cell tumors: Natural history and pathogenesis. J Neurosurg. 1985;63:155–67. doi: 10.3171/jns.1985.63.2.0155. [DOI] [PubMed] [Google Scholar]
- 5.Elizabeth J, Menon G, Bhattacharya RN, Radhakrishnan VV. Germinoma of the basal ganglia: A case report and review of literature. Neurol India. 2002;50:84–6. [PubMed] [Google Scholar]
- 6.Sugiyama S, Kumabe T, Mino M, Fujimura M, Fujiwara I, Tominaga T. Precocious puberty caused by hCG-producing germinoma involving the bilateral basal ganglia and cerebral white matter without 1ypical radiologic findings: Case report. No Shinkei Geka. 2006;34:619–24. [PubMed] [Google Scholar]