

Abstract
Introduction:
Empty sella is usually an incidental finding. Empty sella is an anatomical condition characterized by the presence of cerebrospinal fluid within the sella with a small pituitary gland compressed above the pituitary floor causing endocrine abnormalities.
Aim:
The aim of this study is to evaluate hormonal abnormalities associated with empty sella in tertiary care center.
Materials and Methods:
This ongoing study was carried out in patients attending to endocrine out-patient departments from August 2012 to July 2013. A detailed history and examination was done. Hormonal evaluation including free thyroid hormones, thyroid stimulating hormone, growth hormone (GH), follicular stimulating hormone, luteinizing hormone, cortisol and prolactin was done.
Results:
A total of 16 patients diagnosed clinically and biochemically of hormonal abnormalities were found to have empty sella on magnetic resonance imaging. Hypocortisolemia in 62.5% of cases, hypothyroidism in 50% of cases, in 18.75% hypogonadism, hyper prolactinemia in 18.7.5%, GH deficiency in 12.5% of cases and in 12.5% cases posterior pituitary involvement is seen.
Conclusion:
The high incidence of endocrine abnormalities associated with empty sella necessitates the need for prompt evaluation and early replacement of hormones for better quality-of-life.
Keywords: Empty sella, hypocortisolemia, hyper prolactinemia, hypothyroidism
INTRODUCTION
After Busch used the term empty sella for the first time in 1951, empty sella syndrome was reported in two articles in 1968. Presence of an empty sella is fairly common.[1,2] Hormonal abnormalities due to empty sella constitute a wide spectrum, affecting every endocrine function. About 30% of hormonal abnormalities are due to empty sella. Sometimes empty sella is diagnosed incidentally in a magnetic resonance imaging (MRI) scan. Current usage is to call cases of sellar enlargement that are not related to a previously treated pituitary tumor primary empty sella syndrome, whereas those found following treatment of a pituitary tumor are denoted secondary empty sella syndrome The primary empty sella is evidently a multicausal syndrome, arising from several different pathogenetic processes. Factors to be considered in the formation of the primary empty sella are pituitary cysts, arachnoidal cysts, increased intracranial pressure, the prevalence of diaphragmatic incompetence and ablative intrasellar events such as infarction or hemorrhage.[3,4] A secondary empty sella results from herniation of the subarachnoid space into a vacant sella turcica following extirpation of pathologic sellar contents, whether by surgery or by radiation or by both. The usual lesion is an adenoma and herniation may occur in the setting of either a congenitally deficient diaphragma or one that was weakened by tumor or therapeutic intervention.[5]
AIM
The aim of this study is to evaluate hormonal abnormalities associated with empty sella in a tertiary care center.
MATERIALS AND METHODS
This ongoing study was done in patients attending to endocrine out-patient departments from August 2012 to July 2013. A detailed history examination was carried out. Hormonal evaluation including free thyroid hormones, thyroid stimulating hormone, growth hormone (GH), follicular stimulating hormone, luteinizing hormone, 8 a.m. cortisol and prolactin were done in tertiary care center by chemiluminiscence (Beckmann coulter). Stimulation tests were done as per the requirement. Synacthin stimulation testing with 0.25 mg synacthin was done among patients with 8 a.m. cortisol between 5 and 10 μg/dL.
RESULTS
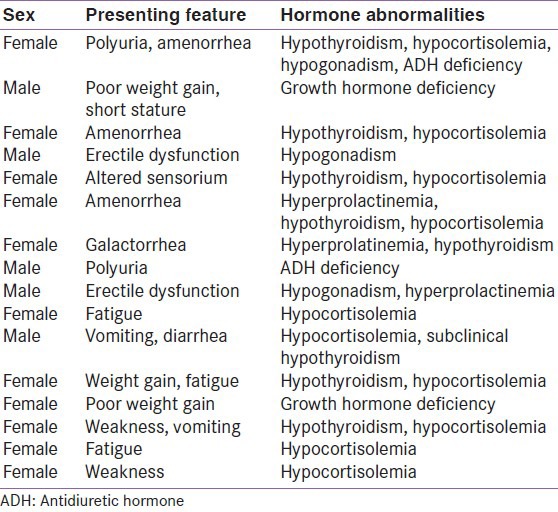
A total of 16 patients diagnosed clinically and biochemically of hormonal abnormalities were found to have empty sella on MRI. Mean age at diagnosis was 41 ± 9 years out of 16 cases 11 were females. Obesity was observed in 25% of cases. In the majority of the cases presenting complaints were weakness, vomiting and diarrhea. Two cases presented with amenorrhea. Dyslipidimea was observed in three cases. Hypocortisolemia was seen in 10 patients (62.5%), hypothyroidism in 8 patients (50%) hyper prolactinemia in 3 patients (18.75%), hypogonadism was observed in 3 patients (18.75%), GH deficiency in 2 patients (12.5%), antidiuretic hormone (ADH) deficiency in two cases (12.5%). Pan hypopituitarism is seen in one case. Combined hormone deficiencies observed among the cases is represented in the Table 1.
Table 1.
Characteristics and hormone deficiencies in empty sella
DISCUSSION
Empty sella was more prevalent in females (68.75%) than in males (32.75%) as seen in earlier studies. Obesity was noted in 25% of cases. The female preponderance is explained by enlargement of pituitary during pregnancy, which may lead to weakening of the sellar diaphragm, thus predisposing to herniation of cerebrospinal fluid (CSF) in to the sella.[6]
In accordance with the study done by De Marinis et al.,[6] in our study obesity was common. Obesity causes obstructive sleep apnea predisposing to hypercapnea and increased CSF pressure leading to empty sella.
In our study, the prevalence of hypocortisolemia, hypothyroidism, hyperprolactinemia, hypogonadism, GH deficiency and ADH deficiency was 62.5% (10/16), 50% (8/16), 18.75% (3/16), 18.75% (3/16), 12.5% (2/16) and 12.5% (2/16) respectively.
In one study done by De Marinis et al. prevalence of empty sella in the general population was 8-35% and hormone deficiencies was 19%.[6] According to Ghatnatti et al. 50% of empty sella were associated endocrine dysfunction, the most common being hyper prolactinemia in 20.8%. Isolated GH deficiency seen in 12.5%, isolated central hypothyroidism in 4.1%, isolated hypocortisolemia in 4.1%. Multiple pituitary hormone deficiency in 4.1%.[7]
In our study, the most prevalent hormonal abnormalities are hypocortisolemia and hypothyroidism.
CONCLUSION
From this study, we conclude that the high incidence of endocrine abnormalities associated with empty sella necessitates the need for prompt evaluation and early replacement of hormones for better quality-of-life.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Busch W. Morphology of sella turcica and its relation to the pituitary gland. Virchows Arch. 1951;320:437–58. doi: 10.1007/BF00957474. [DOI] [PubMed] [Google Scholar]
- 2.Giustina A, Aimaretti G, Bondanelli M, Buzi F, Cannavò S, Cirillo S, et al. Primary empty sella: Why and when to investigate hypothalamic-pituitary function. J Endocrinol Invest. 2010;33:343–6. doi: 10.1007/BF03346597. [DOI] [PubMed] [Google Scholar]
- 3.Maira G, Anile C, Mangiola A. Primary empty sella syndrome in a series of 142 patients. J Neurosurg. 2005;103:831–6. doi: 10.3171/jns.2005.103.5.0831. [DOI] [PubMed] [Google Scholar]
- 4.Del Monte P, Foppiani L, Cafferata C, Marugo A, Bernasconi D. Primary “empty sella” in adults: Endocrine findings. Endocr J. 2006;53:803–9. doi: 10.1507/endocrj.k06-024. [DOI] [PubMed] [Google Scholar]
- 5.McLachlan MS, Williams ED, Doyle FH. Applied anatomy of the pituitary gland and fossa: a radiological and histopathological study based on 50 necropsies. Br J Radiol. 1968;41:782–2. [Google Scholar]
- 6.De Marinis L, Bonadonna S, Bianchi A, Maira G, Giustina A. Primary empty sella. J Clin Endocrinol Metab. 2005;90:5471–7. doi: 10.1210/jc.2005-0288. [DOI] [PubMed] [Google Scholar]
- 7.Ghatnatti V, Sarma D, Saikia U. Empty sella syndrome - beyond being an incidental finding. Indian J Endocrinol Metab. 2012;16:S321–3. doi: 10.4103/2230-8210.104075. [DOI] [PMC free article] [PubMed] [Google Scholar]