

Abstract
Athletes have been misusing growth hormone (GH) for its anabolic and metabolic effects since the early 1980s, at least a decade before endocrinologists began to treat adults with GH deficiency. Although there is an ongoing debate about whether GH is performance enhancing, recent studies suggest that GH improves strength and sprint capacity, particularly when combined with anabolic steroids. The detection of GH misuse is challenging because it is an endogenous hormone. Two approaches have been developed to detect GH misuse; the first is based on the measurement of pituitary GH isoforms and the ratio of 22-kDa isoform to total GH. The second is based on the measurement of insulin like growth factor-I (IGF-I) and N-terminal propeptide of type III procollagen (P-III-NP) which increase in a dose-dependent manner in response to GH administration. Both methodologies have been approved by the World Anti-Doping Agency (WADA) and have led to the detection of a number of athletes misusing GH.
Keywords: Athletes, clinical trial, discriminant function, growth hormone, IGF-I, misuse, performance, P-III-NP
INTRODUCTION
Growth hormone (GH) is secreted by the anterior pituitary gland and plays an important role in maintaining body composition, well-being, physical performance, and cardiovascular health in adults as well as children.[1,2] These features have led to its misuse by professional sportsmen and women who wish to improve their athletic performance.[3] GH use was prohibited by the International Olympic Committee (IOC) in 1989 and it appears on the current World Anti-Doping Agency (WADA) list of prohibited substances.[4] The true prevalence of GH misuse is unknown because of the secrecy that surrounds its misuse but there are sufficient high profile cases to suggest that the scale of misuse warrants the concern of WADA. It is unclear when GH was first used to enhance performance but “The Underground Steroid Handbook” was the earliest publication to describe the potential beneficial effects of GH,[5] at least 10 years before clinical endocrinologists started treating adults with GH deficiency.[6,7]
This review will examine whether GH is performance enhancing properties and will discuss the challenges involved in the detection of exogenous GH administration and the work undertaken to develop a robust test to detect its misuse.
WHY ATHLETES MISUSE GH?
Exercise depends on an adequate supply of nutrients and oxygen to the muscle fibers. Glucose for short-term high-intensity activity and free fatty acids (FFAs) for more prolonged activity are combusted to release kinetic energy. GH has a number of effects on protein anabolism and intermediate metabolism that may improve exercise performance through increased fuel and oxygen delivery to exercising muscle, increased muscle strength or any combination of these factors.[8] In addition, it may improve cardiovascular function[9,10] and thermoregulation.[11]
The potent physiological actions of GH have been demonstrated through a series of randomized controlled trials of GH replacement in people with GH deficiency. Prior to treatment, adults with GH deficiency lose lean tissue while accumulating fat, in particular visceral fat.[12,13] Skeletal muscle mass and strength[14,15,16] is reduced with a consequent impairment of physical performance, exercise capacity, and VO2 max (aerobic capacity or the maximum ability to take in and use oxygen).[17] Following treatment with recombinant human GH (rhGH), body composition normalizes[6,7] and physical performance improves.[18]
It does not necessarily follow, however, that the administration of supraphysiological GH doses will lead to further performance advantage in healthy adults. Indeed the opposite is suggested by acromegaly, which is characterized by marked abnormalities in protein and carbohydrate metabolism,[19,20] muscle weakness rather than excessive strength,[21] and cardiomyopathy.[22] A systematic review of 44 articles describing 27 studies reported that although GH administration was associated with increase in lean body mass and decrease in fat mass, it did not improve a number of measures of performance.[23]
Most recently trials have begun to show a performance benefit for GH. The first was undertaken in abstinent anabolic steroid users and demonstrated significant improvements in strength, peak power output, and VO2 max as well as the expected changes in body composition.[24] It is possible that the prior use of steroids may have rendered the athletes particularly sensitive to the anabolic actions of GH. A further randomized, placebo-controlled trial of 6-weeks’ treatment with rhGH demonstrated a short-lived improvement in sprint capacity in both men and women with GH and a synergistic effect with testosterone in men.[25]
POTENTIAL ADVERSE EFFECTS OF GH MISUSE
The side effects associated with GH administration in GH deficiency are well-documented and may affect any athlete receiving GH;[26] however, as anecdotal evidence suggests that many athletes are taking much higher doses than those used therapeutically, it is possible that features of acromegaly may become apparent with prolonged use. Additional long-term effects may include fluid retention, which may lead to ankle swelling, hypertension, headache, diabetes, and cardiomyopathy. There is also a potential for increased risk of certain cancers; including colorectal, thyroid, breast, and prostate cancer.[27] Cadaveric GH, with its attendant risk of the prion-induced Creutzfeldt-Jakob disease, is still available in the black market.[28]
CHALLENGES IN THE DETECTION OF GH MISUSE
Detecting the misuse of exogenous GH poses a formidable challenge for several reasons.[3] rhGH has an identical amino acid sequence to the native 22-kDaisoform of the hormone, while cadaveric GH is indistinguishable from endogenous GH. It has a short half-life (<20 min) and is secreted in a pulsatile manner leading to widely varying circulating GH concentration throughout the day. Exercise and stress are potent stimulators of GH secretion[29,30] and so high GH concentrations in the post-competition setting would be expected.
DEVELOPMENT OF A TEST TO DETECT GH MISUSE
Two different yet complementary approaches have been investigated to detect GH misuse; the first, pioneered by Christian Strasburger, Martin Bidlingmaier and Zida Wu in Germany, is based on the detection of different pituitary GH isoforms, while the second, which was developed by the GH-2000 and GH-2004 teams, utilizes the measurement of GH-sensitive markers.
THE ISOFORM METHOD
Endogenous pituitary GH occurs in multiple isoforms of which 70% is in the form of a 22 kDa polypeptide.[31] By contrast, rhGH comprises solely the 22-kDa isoform. When rhGH is administered, endogenous pituitary secretion is downregulated through negative feedback and the concentration of non-22-kDa isoforms is suppressed. The isoform method relies on the measurement of the ratio of 22 kDa GH to total GH.[32]
The proportions of GH isoforms are unaffected by age, sex, sporting discipline, and pathological states,[33,34] but exercise causes a transient relative increase in the 22-kDa isoform, thereby reducing the sensitivity of the test if samples are taken immediately after competition.[35,36] This method was introduced prior to the 2004 Athens Olympic Games and subsequently improved when the assays used for the method were commercialized.[37]
After testing over 1,000 samples, the first adverse analytical finding came in February 2010 when the British Rugby League player, Terry Newton, tested positive.[38] Since then, several other positive tests have been reported including the announcement in September 2010 from the Canadian Center for Ethics in Sport that Matt Socholotiuk, a University of Waterloo football player, had tested positive for GH use on 31 March 2010.[39] The following year, Colorado Sky Sox first baseman Mike Jacobs became the first baseball player to test positive for GH and was subsequently suspended for 50 games by Minor League Baseball.[40]
In 2011, Andrus Veerpalu, an Estonian Olympic gold medal winning skier, tested positive for GH. However, he pleaded his innocence and challenged the laboratory finding in the Court of Arbitration for Sport who subsequently acquitted Veerpalu on 25 March 2013 as the court was not convinced that the threshold for considering an adverse analytical finding was sufficiently reliable to uphold the doping conviction; nevertheless, the court stated “that there are many factors in this case which tend to indicate that the Athlete did in fact himself administer exogenous hGH”.[41]
The Achilles’ heel of the isoform method is its short window of detection.[42] Recombinant GH, even when injected subcutaneously, is cleared rapidly and GH is frequently undetectable in a blood sample taken the morning after an injection,[43] while spontaneous GH secretion returns to normal within 48 h of the last dose of rhGH.[44] Consequently, any athlete who ceases GH several days prior to a competition will not be detected. As such, the optimal use of this method is likely to be in unannounced ‘out of competition’ testing, as happened in the case of Terry Newton. A further disadvantage of this method is that it will not detect the use of cadaveric GH or GH secretagogues as these do not alter the isoform profile.
THE GH-2000 MARKER METHOD
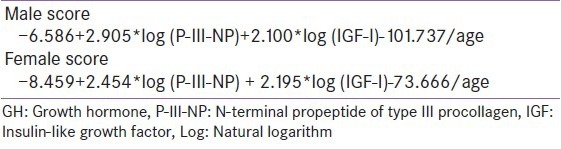
The GH-2000 marker method measures two serum proteins, insulin-like growth factor-I (IGF-I) and N-terminal propeptide of type III procollagen (P-III-NP), both of which increase in a dose-dependent manner in response to GH administration and therefore act as “markers” of GH administration. This method was first conceived by Peter Sönksen who established the large multicenter GH-2000 project, with funding from the European Union under their BIOMED 2 initiative, the International Olympic Committee and GH manufacturers Novo Nordisk and Pharmacia. Initially, 25 potential markers of GH action were considered;[45,46] but IGF-I and P-III-NP were chosen for the GH-2000 test because these provided the best discrimination between individuals receiving GH or placebo during a 28-day randomized controlled GH administration trial.[47] Both IGF-I and P-III-NP have little diurnal or day-to-day variation, low intraindividual variation[48] and only change minimally in response to exercise.[45,46] The markers are used in conjunction with the use of gender specific equations, “discriminant functions”, to improve the sensitivity and specificity of the test compared with single-marker analysis [Table 1].[47] The markers decline with age as endogenous GH secretion declines and a factor relating to the inverse of age is also included in the formulae.[49]
Table 1.
GH-2000 discriminant function equations
Although the principle of the method was approved at an IOC workshop in Rome in March 1999,[50] further work has been needed to ensure that a number of confounding factors including ethnicity,[51,52] injury,[53] sporting discipline,[49,54] exercise,[45,46,55] and body habitus[49,54] would not invalidate the test. The test has subsequently been validated in independent laboratories in Germany[56] and Australia.[57]
Although IGF-I and P-III-NP are more stable than GH, the markers still exhibit a wide interindividual variability that could mean that those with lower baseline marker concentrations are potentially harder to catch. Within individuals, however, there is much less variability which raises the possibility of the use of a biological “athlete passport” or “profiling” to improve the test sensitivity.[48]
The test was introduced at the London Olympic and Paralympic games which led to the disqualification of Nikolay Marfin and Vadim Rakitin, two Russian powerlifters, who admitted to misusing GH after an adverse analytical finding.[58]
CONCLUSION
It is widely believed that athletes are misusing GH for its anabolic and metabolic effects. Recent studies suggest that GH has a modest performance benefit in amateur athletes, particularly when combined with anabolic steroids. Over the last decade, there have been major advances in methodologies to detect GH and this should mean that athletes will no longer be able to take GH with impunity.
ACKNOWLEDGEMENTS
The author is the co-principal investigator of the GH-2004 project which is funded by the World Anti-Doping Agency, United States Anti-Doping Agency, and Partnership for Clean Competition. I would like to acknowledge the rest of the GH-2004 team and support from UK Anti-Doping. I would like to thank all the athletes, both amateur and professional, who volunteered to take part in the GH-2000 and GH-2004 studies. I thank the nurses of the Wellcome Trust Clinical Research Facility and medical students at the University of Southampton for their assistance in recruitment and follow-up of the GH-2004 subjects. The GH-2004 team is indebted to the GH-2000 team who left us a legacy of invaluable samples.
Footnotes
Source of Support: World Anti-Doping Agency, United States Anti-Doping Agency, and Partnership for Clean Competition
Conflict of Interest: None declared
REFERENCES
- 1.Cuneo RC, Salomon F, McGauley GA, Sonksen PH. The growth hormone deficiency syndrome in adults. Clin Endocrinol (Oxf) 1992;37:387–97. doi: 10.1111/j.1365-2265.1992.tb02347.x. [DOI] [PubMed] [Google Scholar]
- 2.Carroll PV, Christ ER, Sonksen PH. Growth hormone replacement in adults with growth hormone deficiency: Assessment of current knowledge. Trends Endocrinol Metab. 2000;11:231–8. doi: 10.1016/s1043-2760(00)00268-x. [DOI] [PubMed] [Google Scholar]
- 3.Holt RI, Sonksen PH. Growth hormone, IGF-I and insulin and their abuse in sport. Br J Pharmacol. 2008;154:542–56. doi: 10.1038/bjp.2008.99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.World Anti-Doping Agency. The World Anti-Doping Agency International Standard- The 2013 Prohibited List. [Accessed 26/07/2013]. Available from: http://www.wada-ama.org/en/World- Anti- Doping-Program /Sports-and-Anti-Doping-Organizations/International-Standards/Prohibited-List .
- 5.Duchaine D. Venice, California, USA: HLR Technical Books; 1982. Underground Steroid Handbook. [Google Scholar]
- 6.Jorgensen JO, Pedersen SA, Thuesen L, Jorgensen J, Ingemann-Hansen T, Skakkebaek NE, et al. Beneficial effects of growth hormone treatment in GH-deficient adults. Lancet. 1989;1:1221–5. doi: 10.1016/s0140-6736(89)92328-3. [DOI] [PubMed] [Google Scholar]
- 7.Salomon F, Cuneo RC, Hesp R, Sonksen PH. The effects of treatment with recombinant human growth hormone on body composition and metabolism in adults with growth hormone deficiency. N Engl J Med. 1989;321:1797–803. doi: 10.1056/NEJM198912283212605. [DOI] [PubMed] [Google Scholar]
- 8.Widdowson WM, Healy ML, Sonksen PH, Gibney J. The physiology of growth hormone and sport. Growth Horm IGF Res. 2009;19:308–19. doi: 10.1016/j.ghir.2009.04.023. [DOI] [PubMed] [Google Scholar]
- 9.Maison P, Chanson P. Cardiac effects of growth hormone in adults with growth hormone deficiency: A meta-analysis. Circulation. 2003;108:2648–52. doi: 10.1161/01.CIR.0000100720.01867.1D. [DOI] [PubMed] [Google Scholar]
- 10.Colao A, Marzullo P, Di Somma C, Lombardi G. Growth hormone and the heart. Clin Endocrinol (Oxf) 2001;54:137–54. doi: 10.1046/j.1365-2265.2001.01218.x. [DOI] [PubMed] [Google Scholar]
- 11.Juul A, Hjortskov N, Jepsen LT, Nielsen B, Halkjaer-Kristensen J, Vahl N, et al. Growth hormone deficiency and hyperthermia during exercise: A controlled study of sixteen GH-deficient patients. J Clin Endocrinol Metab. 1995;80:3335–40. doi: 10.1210/jcem.80.11.7593447. [DOI] [PubMed] [Google Scholar]
- 12.Cuneo RC, Salomon F, Wiles CM, Hesp R, Sonksen PH. Growth hormone treatment in growth hormone-deficient adults. I. Effects on muscle mass and strength. J Appl Physiol. 1991;70:688–94. doi: 10.1152/jappl.1991.70.2.688. [DOI] [PubMed] [Google Scholar]
- 13.Johannsson G, Marin P, Lonn L, Ottosson M, Stenlof K, Bjorntorp P, et al. Growth hormone treatment of abdominally obese men reduces abdominal fat mass, improves glucose and lipoprotein metabolism, and reduces diastolic blood pressure. J Clin Endocrinol Metab. 1997;82:727–34. doi: 10.1210/jcem.82.3.3809. [DOI] [PubMed] [Google Scholar]
- 14.Janssen YJ, Doornbos J, Roelfsema F. Changes in muscle volume, strength, and bioenergetics during recombinant human growth hormone (GH) therapy in adults with GH deficiency. J Clin Endocrinol Metab. 1999;84:279–84. doi: 10.1210/jcem.84.1.5411. [DOI] [PubMed] [Google Scholar]
- 15.Rutherford OM, Beshyah SA, Schott J, Watkins Y, Johnston DG. Contractile properties of the quadriceps muscle in growth hormone-deficient hypopituitary adults. Clin Sci (Lond) 1995;88:67–71. doi: 10.1042/cs0880067. [DOI] [PubMed] [Google Scholar]
- 16.Johannsson G, Grimby G, Sunnerhagen KS, Bengtsson BA. Two years of growth hormone (GH) treatment increase isometric and isokinetic muscle strength in GH-deficient adults. J Clin Endocrinol Metab. 1997;82:2877–84. doi: 10.1210/jcem.82.9.4204. [DOI] [PubMed] [Google Scholar]
- 17.Cuneo RC, Salomon F, Wiles CM, Hesp R, Sonksen PH. Growth hormone treatment in growth hormone-deficient adults. II. Effects on exercise performance. J Appl Physiol. 1991;70:695–700. doi: 10.1152/jappl.1991.70.2.695. [DOI] [PubMed] [Google Scholar]
- 18.Widdowson WM, Gibney J. The effect of growth hormone replacement on exercise capacity in patients with GH deficiency: A metaanalysis. J Clin Endocrinol Metab. 2008;93:4413–7. doi: 10.1210/jc.2008-1239. [DOI] [PubMed] [Google Scholar]
- 19.Colao A, Baldelli R, Marzullo P, Ferretti E, Ferone D, Gargiulo P, et al. Systemic hypertension and impaired glucose tolerance are independently correlated to the severity of the acromegalic cardiomyopathy. J Clin Endocrinol Metab. 2000;85:193–9. doi: 10.1210/jcem.85.1.6318. [DOI] [PubMed] [Google Scholar]
- 20.Ezzat S, Forster MJ, Berchtold P, Redelmeier DA, Boerlin V, Harris AG. Acromegaly. Clinical and biochemical features in 500 patients. Medicine (Baltimore) 1994;73:233–40. [PubMed] [Google Scholar]
- 21.McNab TL, Khandwala HM. Acromegaly as an endocrine form of myopathy: Case report and review of literature. Endocr Pract. 2005;11:18–22. doi: 10.4158/EP.11.1.18. [DOI] [PubMed] [Google Scholar]
- 22.Nagulesparen M, Trickey R, Davies MJ, Jenkins JS. Muscle changes in acromegaly. Br Med J. 1976;2:914–5. doi: 10.1136/bmj.2.6041.914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Liu H, Bravata DM, Olkin I, Friedlander A, Liu V, Roberts B, et al. Systematic review: The effects of growth hormone on athletic performance. Ann Intern Med. 2008;148:747–58. doi: 10.7326/0003-4819-148-10-200805200-00215. [DOI] [PubMed] [Google Scholar]
- 24.Graham MR, Baker JS, Evans P, Kicman A, Cowan D, Hullin D, et al. Physical effects of short-term recombinant human growth hormone administration in abstinent steroid dependency. Horm Res. 2008;69:343–54. doi: 10.1159/000117390. [DOI] [PubMed] [Google Scholar]
- 25.Meinhardt U, Nelson AE, Hansen JL, Birzniece V, Clifford D, Leung KC, et al. The effects of growth hormone on body composition and physical performance in recreational athletes: A randomized trial. Ann Intern Med. 2010;152:568–77. doi: 10.7326/0003-4819-152-9-201005040-00007. [DOI] [PubMed] [Google Scholar]
- 26.Powrie J, Weissberger A, Sonksen P. Growth hormone replacement therapy for growth hormone-deficient adults. Drugs. 1995;49:656–63. doi: 10.2165/00003495-199549050-00002. [DOI] [PubMed] [Google Scholar]
- 27.Jenkins PJ, Mukherjee A, Shalet SM. Does growth hormone cause cancer? Clin Endocrinol (Oxf) 2006;64:115–21. doi: 10.1111/j.1365-2265.2005.02404.x. [DOI] [PubMed] [Google Scholar]
- 28.Brown P, Gajdusek DC, Gibbs CJ, Jr, Asher DM. Potential epidemic of Creutzfeldt-Jakob disease from human growth hormone therapy. N Engl J Med. 1985;313:728–31. doi: 10.1056/NEJM198509193131205. [DOI] [PubMed] [Google Scholar]
- 29.Prinz PN, Weitzman ED, Cunningham GR, Karacan I. Plasma growth hormone during sleep in young and aged men. J Gerontol. 1983;38:519–24. doi: 10.1093/geronj/38.5.519. [DOI] [PubMed] [Google Scholar]
- 30.Savine R, Sonksen P. Growth hormone-hormone replacement for the somatopause? Horm Res. 2000;53(Suppl 3):37–41. doi: 10.1159/000023531. [DOI] [PubMed] [Google Scholar]
- 31.Baumann G. Growth hormone heterogeneity in human pituitary and plasma. Horm Res. 1999;51(Suppl 1):2–6. doi: 10.1159/000053128. [DOI] [PubMed] [Google Scholar]
- 32.Wu Z, Bidlingmaier M, Dall R, Strasburger CJ. Detection of doping with human growth hormone. Lancet. 1999;353:895. doi: 10.1016/S0140-6736(99)00775-8. [DOI] [PubMed] [Google Scholar]
- 33.Irie M, Ueki M, Kishikawa Y, Nishii M, Kawahara T. 20K-GH and its use in detecting GH abuse. Growth Horm IGF Res. 2009;19:352–6. doi: 10.1016/j.ghir.2009.04.013. [DOI] [PubMed] [Google Scholar]
- 34.Holt RI. Meeting reports: Beyond reasonable doubt: Catching the growth hormone cheats. Pediatr Endocrinol Rev. 2007;4:228–32. [PubMed] [Google Scholar]
- 35.Wallace JD, Cuneo RC, Bidlingmaier M, Lundberg PA, Carlsson L, Boguszewski CL, et al. Changes in non-22-kilodalton (kDa) isoforms of growth hormone (GH) after administration of 22-kDa recombinant human GH in trained adult males. J Clin Endocrinol Metab. 2001;86:1731–7. doi: 10.1210/jcem.86.4.7379. [DOI] [PubMed] [Google Scholar]
- 36.Wallace JD, Cuneo RC, Bidlingmaier M, Lundberg PA, Carlsson L, Boguszewski CL, et al. The response of molecular isoforms of growth hormone to acute exercise in trained adult males. J Clin Endocrinol Metab. 2001;86:200–6. doi: 10.1210/jcem.86.1.7129. [DOI] [PubMed] [Google Scholar]
- 37.Bidlingmaier M, Suhr J, Ernst A, Wu Z, Keller A, Strasburger CJ, et al. High-sensitivity chemiluminescence immunoassays for detection of growth hormone doping in sports. Clin Chem. 2009;55:445–53. doi: 10.1373/clinchem.2008.112458. [DOI] [PubMed] [Google Scholar]
- 38.Newton gets 2 years for world-first hGH finding. [Accessed 26/07/2013]. Available from: http://www.ukad.org.uk/news/article/newton-gets-two-years-for-world-first-hgh-finding .
- 39.CCES announces four anti-doping rule violations from University of Waterloo football team testing including the first for an adverse analytical finding of human growth hormone in North America. [Accessed 26/07/2013]. Available from: http://www.cces.ca/en/news-137-ccesannounces-four-anti-doping-rule-violations .
- 40.Statement on positive hGH test in Minor League Baseball. [Accessed 26/07/2013]. Available from: http://www.wada-ama.org/en/Media-Center/Archives/Articles/Statement-on-positive-hGH-test-in-Minor-League-Baseball .
- 41.CAS 2011/A/2566 Andrus Veerpalu v. International Ski Federation. [Accessed 26/07/2013]. Available from: http://www.tas-cas.org/d2wfiles/document/6633/5048/0/256620FINAL20Award20_internet_.pdf .
- 42.Keller A, Wu Z, Kratzsch J, Keller E, Blum WF, Kniess A, et al. Pharmacokinetics and pharmacodynamics of GH: Dependence on route and dosage of administration. Eur J Endocrinol. 2007;156:647–53. doi: 10.1530/EJE-07-0057. [DOI] [PubMed] [Google Scholar]
- 43.Giannoulis MG, Boroujerdi MA, Powrie J, Dall R, Napoli R, Ehrnborg C, et al. Gender differences in growth hormone response to exercise before and after rhGH administration and the effect of rhGH on the hormone profile of fit normal adults. Clin Endocrinol (Oxf) 2005;62:315–22. doi: 10.1111/j.1365-2265.2005.02216.x. [DOI] [PubMed] [Google Scholar]
- 44.Wu RH, St LY, Martino-Nardi J, Wesoly S, Sobel EH, Sherman B, et al. Preservation of physiological growth hormone (GH) secretion in idiopathic short stature after recombinant GH therapy. J Clin Endocrinol Metab. 1990;70:1612–5. doi: 10.1210/jcem-70-6-1612. [DOI] [PubMed] [Google Scholar]
- 45.Wallace JD, Cuneo RC, Lundberg PA, Rosen T, Jorgensen JO, Longobardi S, et al. Responses of markers of bone and collagen turnover to exercise, growth hormone (GH) administration, and GH withdrawal in trained adult males. J Clin Endocrinol Metab. 2000;85:124–33. doi: 10.1210/jcem.85.1.6262. [DOI] [PubMed] [Google Scholar]
- 46.Wallace JD, Cuneo RC, Baxter R, Orskov H, Keay N, Pentecost C, et al. Responses of the growth hormone (GH) and insulin-like growth factor axis to exercise, GH administration, and GH withdrawal in trained adult males: A potential test for GH abuse in sport. J Clin Endocrinol Metab. 1999;84:3591–601. doi: 10.1210/jcem.84.10.6037. [DOI] [PubMed] [Google Scholar]
- 47.Powrie JK, Bassett EE, Rosen T, Jorgensen JO, Napoli R, Sacca L, et al. Detection of growth hormone abuse in sport. Growth Horm IGF Res. 2007;17:220–6. doi: 10.1016/j.ghir.2007.01.011. [DOI] [PubMed] [Google Scholar]
- 48.Erotokritou-Mulligan I, Bassett EE, Cowan DA, Bartlett C, Milward P, Sartorio A, et al. The use of growth hormone (GH)-dependent markers in the detection of GH abuse in sport: Physiological intra-individual variation of IGF-I, type 3 pro-collagen (P-III-P) and the GH-2000 detection score. Clin Endocrinol (Oxf) 2010;72:520–6. doi: 10.1111/j.1365-2265.2009.03668.x. [DOI] [PubMed] [Google Scholar]
- 49.Healy ML, Dall R, Gibney J, Bassett E, Ehrnborg C, Pentecost C, et al. Toward the development of a test for growth hormone (GH) abuse: A study of extreme physiological ranges of GH-dependent markers in 813 elite athletes in the postcompetition setting. J Clin Endocrinol Metab. 2005;90:641–9. doi: 10.1210/jc.2004-0386. [DOI] [PubMed] [Google Scholar]
- 50.Sonksen P. The International Olympic Committee (IOC) and GH-2000. Growth Horm IGF Res. 2009;19:341–5. doi: 10.1016/j.ghir.2009.04.015. [DOI] [PubMed] [Google Scholar]
- 51.Erotokritou-Mulligan I, Bassett EE, Cowan DA, Bartlett C, McHugh C, Sonksen PH, et al. Influence of ethnicity on IGF-I and procollagen III peptide (P-III-P) in elite athletes and its effect on the ability to detect GH abuse. Clin Endocrinol (Oxf) 2009;70:161–8. doi: 10.1111/j.1365-2265.2008.03319.x. [DOI] [PubMed] [Google Scholar]
- 52.Holt RI, Erotokritou-Mulligan I, McHugh C, Bassett EE, Bartlett C, Fityan A, et al. The GH-2004 project: The response of IGF1 and type III pro-collagen to the administration of exogenous GH in non-Caucasian amateur athletes. Eur J Endocrinol. 2010;163:45–54. doi: 10.1530/EJE-09-0978. [DOI] [PubMed] [Google Scholar]
- 53.Erotokritou-Mulligan I, Bassett EE, Bartlett C, Cowan D, McHugh C, Seah R, et al. The effect of sports injury on insulin like growth factor-I and procollagen III peptide: Implications for detection of growth hormone abuse in athletes. J Clin Endocrinol Metab. 2008;93:2760–63. doi: 10.1210/jc.2007-2801. [DOI] [PubMed] [Google Scholar]
- 54.Nelson AE, Howe CJ, Nguyen TV, Leung KC, Trout GJ, Seibel MJ, et al. Influence of demographic factors and sport type on growth hormone-responsive markers in elite athletes. J Clin Endocrinol Metab. 2006;91:4424–32. doi: 10.1210/jc.2006-0612. [DOI] [PubMed] [Google Scholar]
- 55.Velloso CP, Aperghis M, Godfrey R, Blazevich AJ, Bartlett C, Cowan D, et al. The effects of two weeks of recombinant growth hormone administration on the response of IGF-I and N-terminal pro-peptide of collagen type III (P-III-NP) during a single bout of high resistance exercise in resistance trained young men. Growth Horm IGF Res. 2013;23:76–80. doi: 10.1016/j.ghir.2013.01.002. [DOI] [PubMed] [Google Scholar]
- 56.Kniess A, Ziegler E, Kratzsch J, Thieme D, Muller RK. Potential parameters for the detection of hGH doping. Anal Bioanal Chem. 2003;376:696–700. doi: 10.1007/s00216-003-1926-x. [DOI] [PubMed] [Google Scholar]
- 57.Nelson AE, Meinhardt U, Hansen JL, Walker IH, Stone G, Howe CJ, et al. Pharmacodynamics of growth hormone abuse biomarkers and the influence of gender and testosterone: A randomized double-blind placebo-controlled study in young recreational athletes. J Clin Endocrinol Metab. 2008;93:2213–22. doi: 10.1210/jc.2008-0402. [DOI] [PubMed] [Google Scholar]
- 58.Latest Testing Methods Result in Suspension of Two Russian Powerlifters for Anti-Doping. [Accessed 26/07/2013]. Available from: http://www.paralympic.org/press-release/latest-testing-methods-result-suspensiontwo-russian-powerlifters-anti-doping .